
Abstract
BACKGROUND/OBJECTIVE:
Persistent postural-perceptual dizziness (PPPD) is worsened in a standing posture, or by body movement, or visual stimulation. We aimed to evaluate postural stability in PPPD patients using foam posturography and to investigate the dependence on visual and somatosensory input in the standing posture.
METHODS:
Foam posturography was performed on 53 PPPD patients, and data from the PPPD patients were compared with the data from an age- and sex-matched healthy controls. The PPPD patients were divided into four groups based on the findings of vestibular function tests and the effect of vestibular function on posturographic data was examined.
RESULTS:
Romberg’s ratios were significantly higher in PPPD patients than in controls. The median Romberg’s ratios in PPPD patients with normal vestibular function were also higher than those in controls. However, foam ratio was significantly lower in PPPD patients than in controls. The median foam ratios in PPPD patients with vestibular dysfunction were also lower than those in controls.
CONCLUSIONS:
In a standing posture, PPPD patients may be more dependent on visual input and less dependent on somatosensory input than healthy subjects. Higher dependence on visual and lower dependence on somatosensory input in PPPD may be a feature unaffected by vestibular function.
Introduction
Persistent postural - perceptual dizziness (PPPD) is characterized by one or more of the following symptoms: unsteadiness, a sensation of floating, or non-rotating dizziness that is present almost every day for more than three months. The diagnostic criteria for PPPD were defined by the Barany Society and added to the 11th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-11) in 2017 [31]. PPPD is precipitated by conditions that cause a balance disorder, including vestibular, psychiatric, and traumatic diseases, but the dizziness in PPPD cannot be explained by the conditions.
Dizziness in PPPD is worsened by three exacerbating factors: standing posture, body movement, and visual stimulation. Most PPPD patients complain that their symptoms are more severe when standing or walking than when sitting or lying down [2, 30]. Environmental visual stimuli that exacerbate symptoms are primarily those where there is visual flow across the visual field, large complex patterns, or wide-open spaces with distant or indistinct visuospatial reference points [4, 26]. Patients with visual vertigo with pathologies similar to PPPD manifested dependence on visual input, tendency to rely on visual information for spatial orientation [4, 25]. A possible association between PPPD and dependence on visual input has been suggested. Posture in humans is maintained by muscular actions governed by the central nervous system. The central processing integrates information from vestibular, visual, and somatosensory input [1, 15]. Foam posturography is a method which measures the center of pressure (COP) sway while standing on a foam rubber surface. Standing on foam rubber disrupts the somatosensory input from the lower limbs, and closing the eyes blocks any visual input. Measuring COP movement under these conditions makes it possible to quantitatively evaluate dependence on visual and somatosensory input while in a standing posture. In foam posturography, patients with unilateral or bilateral peripheral vestibulopathy show more severe balance deficits than healthy controls and reveal higher dependence on visual and somatosensory input [13].
In the present study, we examined the postural characteristics of PPPD patients by comparing them to healthy controls, using foam posturography. For further analysis, we investigated the effect of vestibular dysfunction comorbid with PPPD on postural stability.
Materials and methods
Participants
53 PPPD patients [12 men and 41 women; age range 18–84 years, mean (±SD) age 52.1(±14.6) years] were enrolled in this study. Subjects were recruited between January 2017 and April 2022 from the Balance Disorder Clinic, Department of Otolaryngology and Head and Neck Surgery, at the University of Tokyo Hospital. We diagnosed PPPD according to the PPPD guidelines published in a consensus statement of the Barany society [31]. The subjects underwent testing of air-conducted sound elicited cervical vestibular evoked myogenic potentials (ACS cVEMP) and bone-conducted vibration elicited ocular vestibular evoked myogenic potentials (BCV oVEMP) to examine the function of the otolith organs [22, 28], and also the video head impulse test (vHIT) to examine semicircular canal function [19, 21]. We used observational study data obtained from 194 healthy subjects in Japan [95 men and 99 women; age range 15–89 years, mean (±SD) age 51.0 (±22.8) years] with no history of dizziness or balance dysfunction between January 2010 and December 2011 [10, 11]. From this observational study data, 53 age- and sex-matched healthy subjects [12 men and 41 women; age range 18–84 years, mean (±SD) age 52.1(±14.7) years] were selected as the control group. Data from the 53 PPPD patients were compared with data from the 53 healthy subjects.
The present study was approved by the Research Ethics Committee, Graduate School of Medicine and Faculty of Medicine, the University of Tokyo (#2487). The procedures were conducted in accordance with the tenets of the Declaration of Helsinki. Written informed consent was waived for the present study, because retrospective data from medical records were used. We performed the opt-out approach in our hospital.
Posturography test
Real time measurements of changes in the position of the COP were provided using Gravicorder G-620 (Anima, Tokyo, Japan). We measured the following two COP parameters in the XY plane (Fig. 1): the mean velocity of the COP movement (velocity) and the area enclosed by the COP movement (area). We measured these two parameters under four conditions: Fixed/Open (eyes open without foam rubber), Fixed/Closed (eyes closed without foam rubber), Foam/Open (eyes open with foam rubber), Foam/Closed (eyes closed with foam rubber). Instantaneous fluctuations of the COP were obtained at a sampling rate of 20 Hz with or without foam rubber. The recording time was 60 seconds or until the subject needed assistance to prevent falling. The tests were performed according to the following procedures. 1) Subjects stood on a force plate with their toes closed and both feet together. The test was recorded in 60 seconds in both open and closed eye conditions. 2) The subject was removed from the force plate, and the foam rubber was placed on the force plate. 3) The subject stood on the foam rubber with the heels of both feet touching and the toes open at 45 degrees. 4) The test was recorded in 60 seconds under both open and closed eye conditions. The material of the foam rubber was made of natural rubber, with a tensile strength of 2.1 kgf/cm2, an elongation stretch percentage of 110%, a density of 0.06 g/cm3, and a thickness of 3.5 cm.

An example of statokinesigram. This data was obtained from 57-year-old female PPPD patient. The COP sway of the subject was displayed as a continuous curve.
We divided the PPPD patients into four groups based on the findings of vestibular function tests: 1) VEMP normal and vHIT normal, 2) VEMP abnormal and vHIT normal, 3) VEMP normal and vHIT abnormal, 4) VEMP abnormal and vHIT abnormal. Patients with abnormalities in either or both oVEMP and cVEMP were considered to have abnormal VEMP (Table 1).
Clinical features of 53 PPPD patients
Abbreviations: ACS cVEMP, Air-conducted sound elicited cervical vestibular evoked myogenic potentials. BCV oVEMP, Bone-conducted vibration elicited ocular vestibular evoked myogenic potentials. vHIT, video head impulse test.
We calculated Romberg’s ratio of the velocity and area, without and with the foam rubber. Romberg’s ratio was defined as the ratio of a measured value with the eyes closed to that with eyes open. The four conditions were defined as follows: Velocity/Fixed (Romberg’s ratio of the velocity without the foam rubber), Area/Fixed (Romberg’s ratio of the area without the foam rubber), Velocity/Foam (Romberg’s ratio of the velocity with the foam rubber), Area/Foam (Romberg’s ratio of the area with the foam rubber). We also measured the foam ratio, defined as the ratio of a measured value with the foam rubber to without the foam rubber. If the foam ratio is greater, the effect of standing on foam rubber on balance deterioration is considered to be greater, thus indicating a higher dependence on lower extremity somatosensory perception in the standing posture. We calculated the foam ratio of the velocity and the area, with the eyes open and closed. The four conditions were defined as follows: Velocity/Open (the foam ratio of the velocity with the eyes open), Area/Open (the foam ratio of the area with the eyes open), Velocity/Closed (the foam ratio of the velocity with the eyes closed), Area/Closed (the foam ratio of the area with the eyes closed).
Electromyographic (EMG) activity was recorded from a surface electrode placed on the upper half of each sternocleidomastoid muscle, with a reference electrode on the side of the upper sternum and a ground electrode on the chin. During the recording, subjects were tested in sitting position with the head rotated away from the side of stimulation. The EMG signal from the stimulated side was amplified and bandpass-filtered (20–2000 Hz) using Neuropack MEB-2306 (Nihon Kohden, Tokyo, Japan). The stimulation rate was 5 Hz, and the analysis time was 100 ms. Muscle activation was monitored through the display of EMG activity to maintain muscle contraction. We verified that the mean rectified EMG was greater than 50μV for each test. Short tone bursts of 500 Hz (105 dBnHL, 135 dBpSPL (peak value), rise/fall time 1 ms, plateau time 2 ms) were also presented. The latencies and amplitudes of the first positive–negative peaks (p13–n23) of the cVEMP were evaluated. Amplitude and latency were determined from the average of 2 runs. Averages of two sets of 100 stimuli each were computed. For the evaluation of amplitude, the asymmetry ratio for p13–n23 amplitude (cVEMP AR) was calculated as 100 [(Au -Aa)/(Aa + Au)], where Au is the p13–n23 amplitude on the unaffected side and Aa is the p13–n23 amplitude on the affected side. The upper limit of normal for the ACS cVEMP AR was set at 41.6 [12]. When no reproducible p13–n23 was present in 2 runs, we regarded it as an “absent response”. When a reproducible p13–n23 was present and the cVEMP AR (%) was greater than the normal upper limit, we regarded it as a “decreased response”. We regarded both “absent” and “decreased” responses as abnormal responses for the purpose of our analyses.
BCV oVEMP testing
EMG electrodes were positioned on the skin 1 cm below (active) and 3 cm below (indifferent) the center of each lower eyelid. The ground electrode was placed on the chin. During testing, the subject looked up approximately 30 degrees above straight ahead and maintained their focus on a small dot approximately 1 m from their eyes while in a seated position. The EMG signals were amplified by a differential amplifier (bandwidth: 0.5–500 Hz), and the unrectified signals were averaged (n = 50) using Neuropack MEB-2306. The bone-conducted vibration stimuli were 4 ms tone-bursts of 500 Hz vibration (rise/fall time = 1 ms and plateau time = 2 ms) delivered by a hand-held 4810 mini-shaker (Bruel and Kjaer, Naerum, Denmark) fitted with a short rod terminated in a bakelite cap 1.5 cm in diameter, which was placed perpendicularly on the forehead at the hairline, in the midline (Fz). The driving voltage was 80 V peak to peak, and it produced a peak force level of 128 dB re 1μN. The stimuli were applied 3 times per second, and the time window for analysis was 50 ms. Consecutive runs were performed to confirm the reproducibility of the oVEMP responses. We analyzed the latency of the first negative peak (nI) and the subsequent positive peak (pI), and the amplitude between nI and pI. Amplitude and latency were determined from the average of 2 runs. Averages of two sets of 50 stimuli each were computed. For the evaluation of amplitude, the asymmetry ratio for nI–pI amplitude (oVEMP AR) was calculated as 100 [(Au - Aa)/(Aa + Au)], where Au is the nI–pI amplitude on the unaffected side and Aa is the nI–pI amplitude on the affected side [6]. Responses recorded from the eye contralateral to stimulation were used for calculating oVEMP AR. The upper limit of the normal BCV oVEMP AR was set at 27.3 [16]. When no reproducible nI–pI was present in 2 runs, we regarded it as an “absent response”. When a reproducible nI–pI was present and the oVEMP AR (%) was greater than the normal upper limits, we regarded it as a “decreased response”. We regarded both “absent” and “decreased” responses as abnormal responses for the purpose of our analyses.
vHIT
The vHIT was performed to assess the vestibulo-ocular reflex (VOR) in the three semicircular canal planes using an ICS impulse (Otometrics, Taastrup, Denmark). Subjects were seated 1 m from a wall with a black fixation dot that served as the visual target. While the subject was asked to stare at the fixation dot, the examiner briefly and unpredictably rotated the subject’s head. The head rotations were made in the lateral, the left anterior-right posterior, and the right anterior left posterior planes. If a mean VOR gain in vHIT of <0.7 for the vertical canals or <0.8 for the lateral canals was detected, the semicircular canal function was regarded as abnormal [21].
Statistical analysis
Continuous variables are summarized as means and ranges. Categorical variables are represented by frequencies and percentages. We used the Wilcoxon signed-rank test to assess differences between the PPPD group and the control group using BellCurve for EXCEL (Social Survey Research Information Co., Ltd. Tokyo, Japan) to examine the postural characteristics in PPPD patients. Patients who required intervention to prevent them falling under any of the conditions, were assigned the most extreme value over the maximum among the values recorded by the subjects who could stand unaided for 60 s through the trial. There were three patients who required intervention to prevent them falling in the eyes open without foam rubber condition. It was assumed that these three patients would need intervention to prevent falling in the other three conditions, and so the analysis was performed assuming a maximum value. For Romberg’s ratio and the foam ratio, if the denominator could be measured but the numerator could not be measured due to the cessation due to fall prevention, the ratio was considered large and a hypothetically large value was set, but the cases where the denominator could not be measured due to the cessation due to fall prevention were excluded from the analyses. A p-value of less than 0.05 indicated the presence of a statistically significant difference. Descriptive statistics were performed due to the small number of subjects in the analysis divided by vestibular function. We did not adjust for multiple testing due to the exploratory nature of this study.
Results
Comparison of posturographic findings between PPPD patients and healthy control
First, we compared the velocity and area of the PPPD group to the control group to investigate their balance function in a standing posture (Figs. 2, 3). The velocity in the PPPD group was significantly higher than that in the control group in the Fixed/Open, Fixed/Closed and Foam/Closed conditions (Fig. 2, Wilcoxon signed-rank test). In the Foam/Open condition, the difference was not statistically significant (Fig. 2c, p = 0.186, Wilcoxon signed-rank test). The area in the PPPD group was significantly higher than that in the control group in the Fixed/Open, Fixed/Closed, Foam/Open and Foam/Closed conditions (Fig. 3, Wilcoxon signed-rank test). These results suggest that the PPPD group showed more severe balance deficits than the control group.
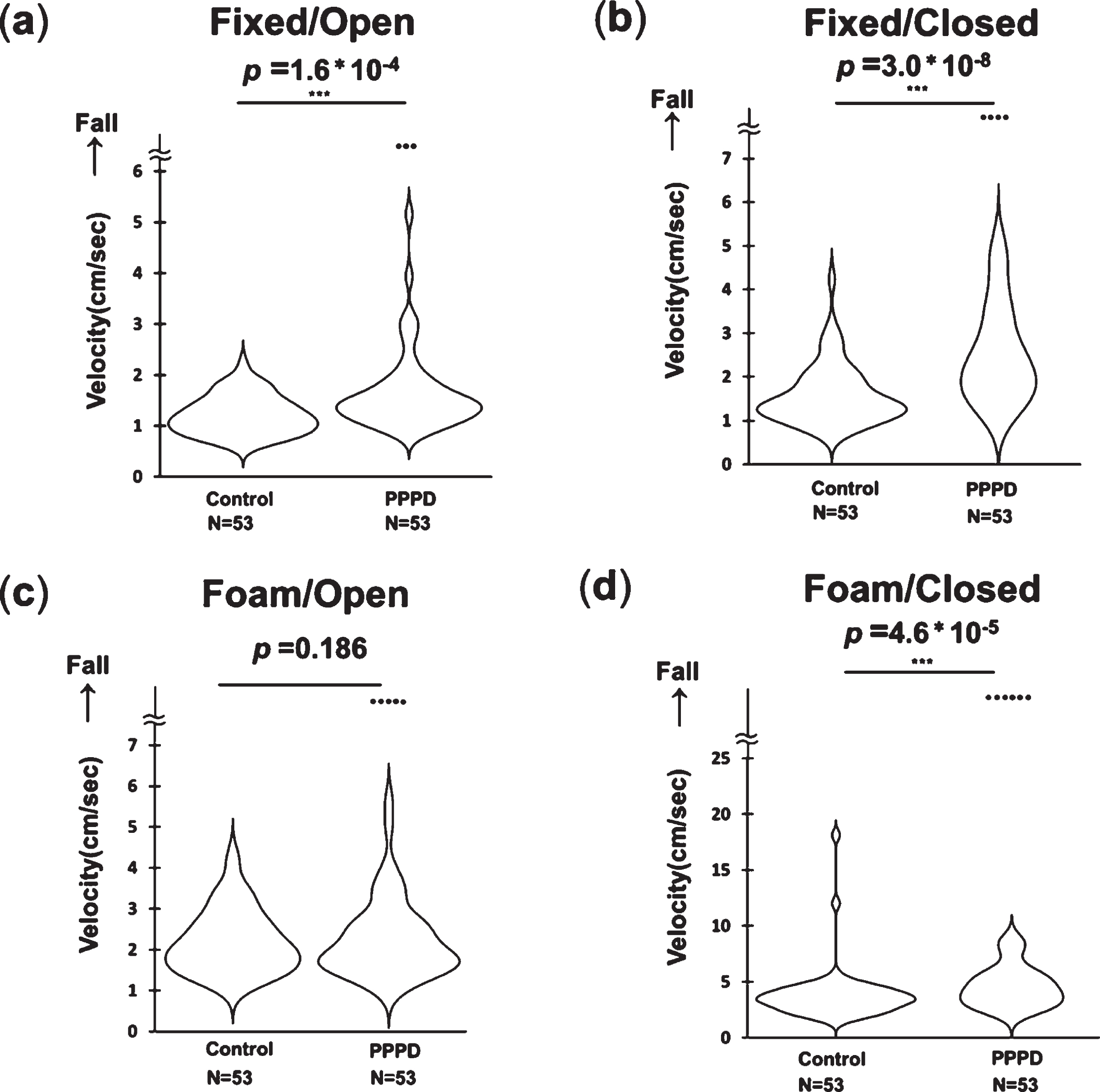
Violin plots of the velocity in the PPPD group and control group. (a) Fixed/Open: eyes open without the foam rubber, (b) Fixed/Closed: eyes closed without the foam rubber, (c) Foam/Open: eyes open with the foam rubber, (d) Foam/Closed: eyes closed with the foam rubber. The dots above the undulating lines represent the data of subjects who required assistance to prevent falling. *p < 0.05, **p < 0.01, ***p < 0.001 (for Wilcoxon signed-rank test).
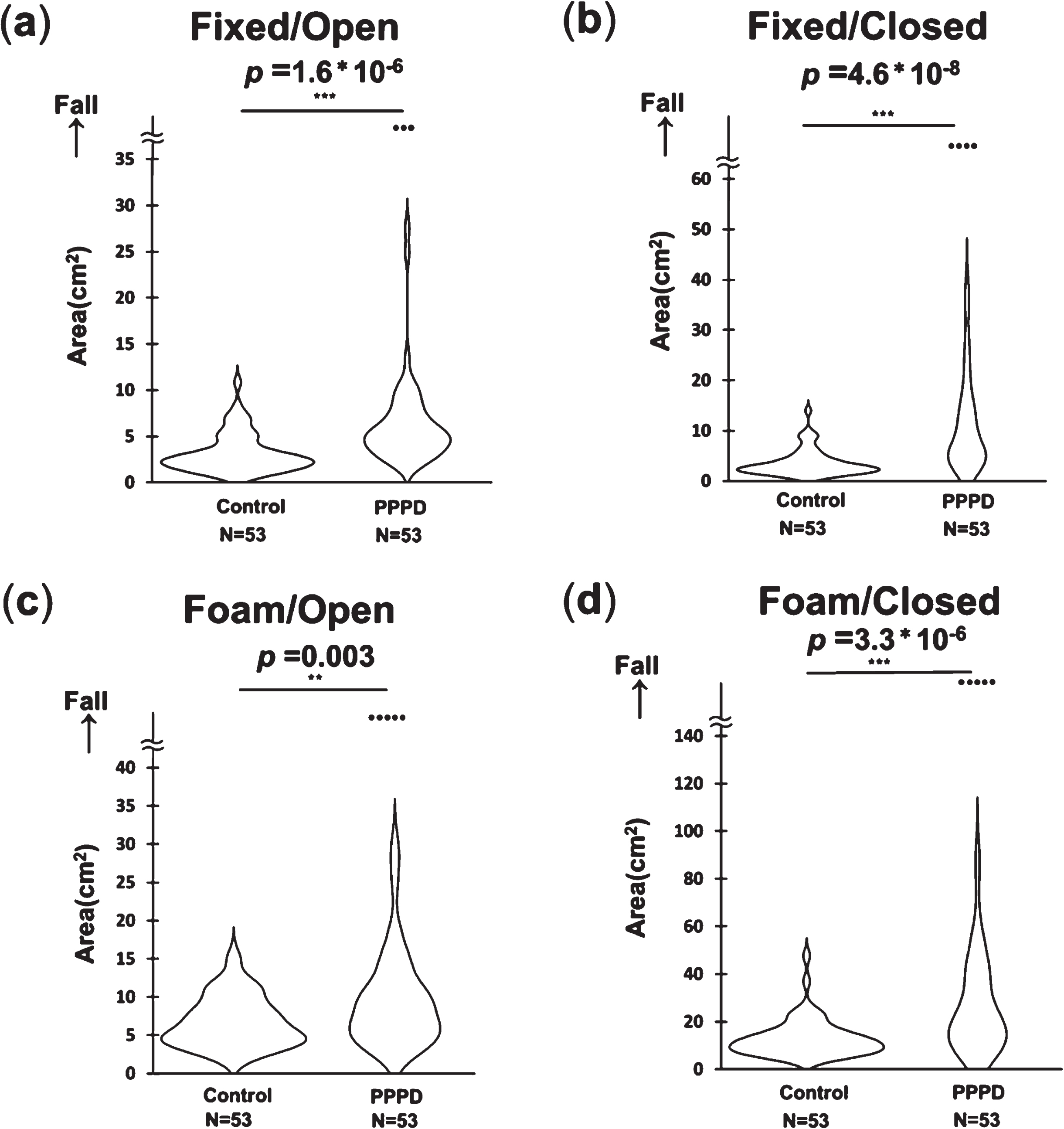
Violin plots of the area in the PPPD group and control group. (a) Fixed/Open: eyes open without the foam rubber, (b) Fixed/Closed: eyes closed without the foam rubber, (c) Foam/Open: eyes open with the foam rubber, (d) Foam/Closed: eyes closed with the foam rubber. The dots above the undulating lines represent the data of subjects who required assistance to prevent falling. *p < 0.05, **p < 0.01, ***p < 0.001 (for Wilcoxon signed-rank test).
Next, we compared Romberg’s ratios of the velocity and area between the two groups. Romberg’s ratios were significantly higher in the PPPD group than in the control group in the Velocity/Fixed, Area/Fixed, Velocity/Foam and Area/Foam conditions (Fig. 4, Wilcoxon signed-rank test). These results suggest that the PPPD group showed more dependence on visual input in a standing posture than the control group. Then, we compared the foam ratios of the velocity and area between the two groups. The foam ratios were significantly higher in the control group than in the PPPD group in the Velocity/Open, Area/Open, Velocity/Closed and Area/Closed conditions (Fig. 5, Wilcoxon signed-rank test). These results suggest that the PPPD group tend to have lower dependence on somatosensory input in a standing posture than the control group. We performed a sensitivity analysis to determine if the 3 PPPD patients who required intervention to prevent them falling in the eyes open without foam rubber condition biased the results. After removing those 3 individuals, the results were not different.
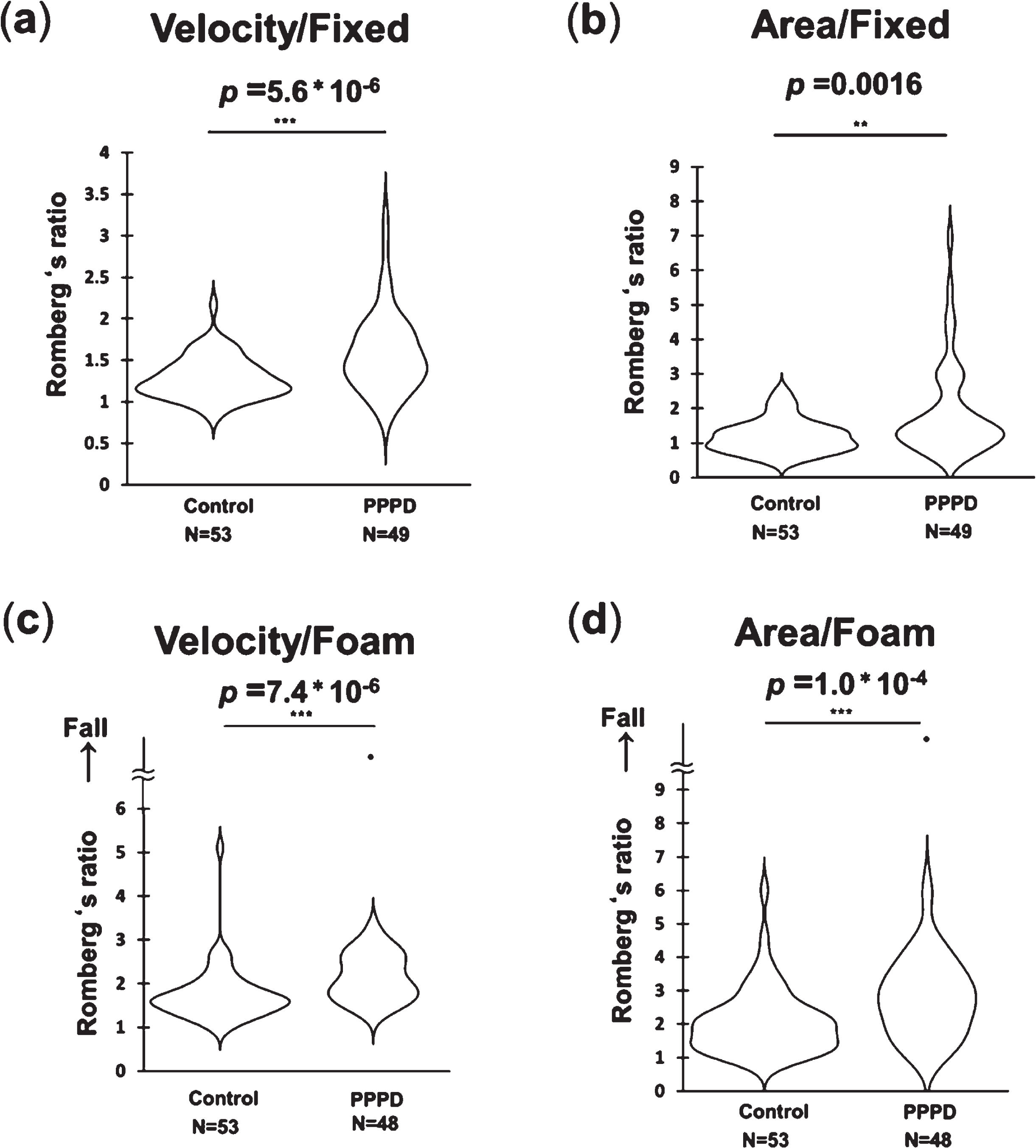
Violin plots of Romberg’s ratios in the PPPD group and control group. (a) Velocity/Fixed: Romberg’s ratio of the velocity without the foam rubber, (b) Area/Fixed: Romberg’s ratio of the area without the foam rubber, (c) Velocity/Foam: Romberg’s ratio of the velocity with the foam rubber, (d) Area/Foam: Romberg’s ratio of the area with the foam rubber. The dots above the undulating lines represent data of subjects who required assistance to prevent falling. Romberg’s ratio was defined as the ratio of a measured value with eyes closed to that with eyes open. *p < 0.05, **p < 0.01, ***p < 0.001 (for Wilcoxon signed-rank test).
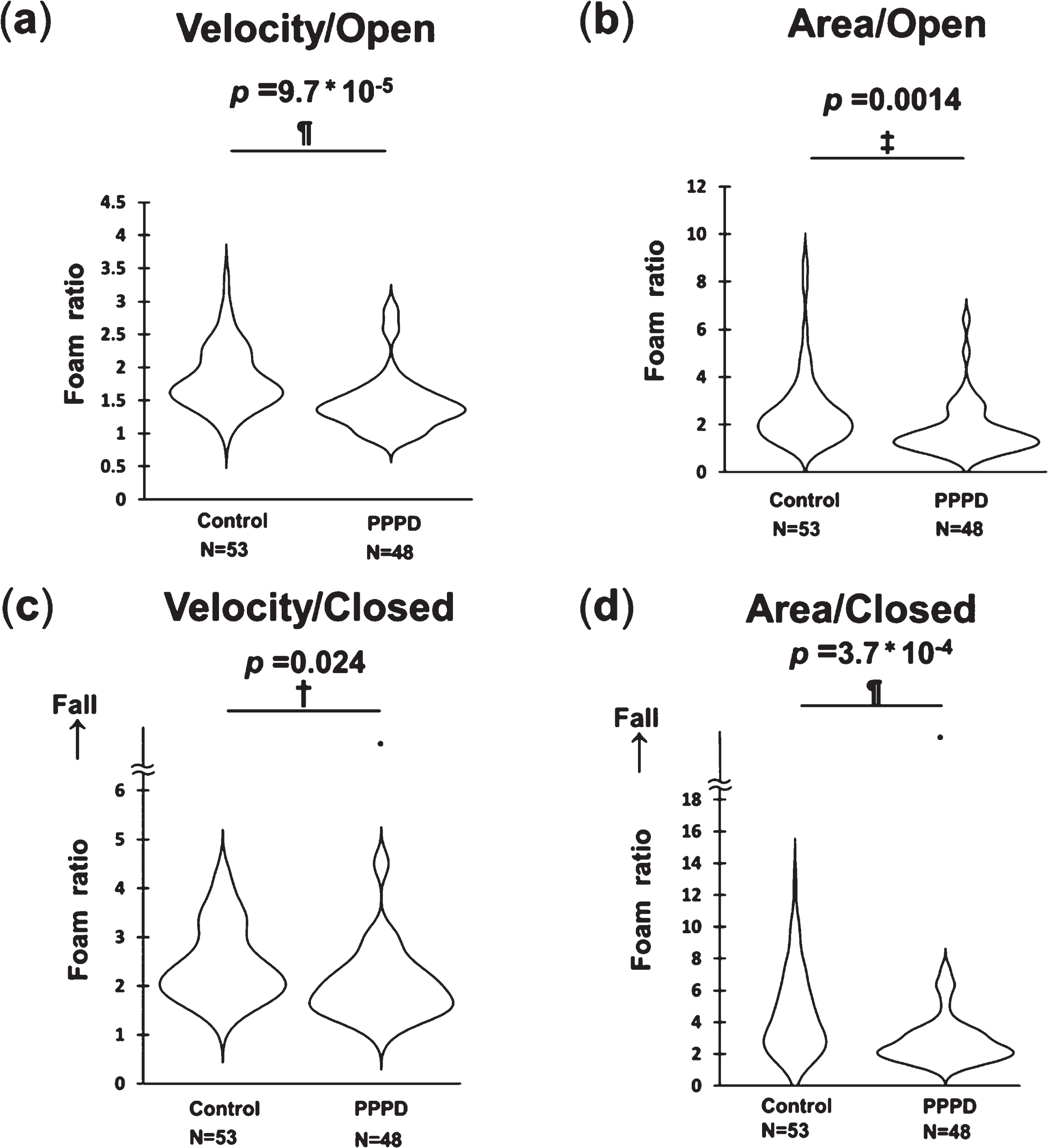
Violin plots of the foam ratios in the PPPD group and control group. (a) Velocity/Open: foam ratio of the velocity with the eyes open, (b) Area/Open: foam ratio of the area with the eyes open, (c) Velocity/Closed: foam ratio of the velocity with the eyes closed, (d) Area/Closed: foam ratio of the area with the eyes closed. The dots above the undulating lines represent data of subjects who required assistance to prevent falling. Foam ratio was defined as the ratio of a measured value with the foam rubber to without the foam rubber. †p < 0.05, ‡p < 0.01, ¶p < 0.001 (for Wilcoxon signed-rank test).
We examined the effect of vestibular function on the standing posture in PPPD patients (Table 2). One patient was unable to undergo cVEMP testing and 16 were unable to undergo vHIT due to neck problems (Table 1). In the VEMP abnormal vHIT abnormal group, there were cases of falling in all four conditions, while in the VEMP abnormal vHIT normal group, there were cases of falling in all conditions except for the Fixed/Open condition (Table 2). In terms of the velocity, the VEMP normal vHIT normal group had the smallest median value in the Foam/Closed and Foam/Open conditions, but this was not observed in the other conditions (Table 2, descriptive statistics). In terms of the area, the VEMP normal vHIT normal group had the smaller median value than the group with vestibular dysfunction in all four conditions (Table 2, descriptive statistics).
Results of the posturography test divided into four groups based on the findings of vestibular function
Results of the posturography test divided into four groups based on the findings of vestibular function
Abbreviations: IQR, interquartile range. VEMP N vHIT N, VEMP Normal vHIT Normal. VEMP A vHIT N, VEMP Abnormal vHIT Normal. VEMP N vHIT A, VEMP Normal vHIT Abnormal. VEMP A vHIT A, VEMP Abnormal vHIT Abnormal.
Next, we examined the effect of the vestibular function on Romberg’s ratios. The VEMP normal vHIT normal group had the smaller median value than the group with vestibular dysfunction in the Velocity/Foam condition and the median values in the VEMP normal vHIT normal group were larger than those of controls in all four conditions (Table 2, descriptive statistics).
Then, we examined the effect of the vestibular function on foam ratios. The VEMP normal vHIT normal group had the smaller median value than the group with vestibular dysfunction in the Velocity/Closed condition. The median values in the VEMP normal vHIT normal group and the other three PPPD group with vestibular dysfunction were smaller than those of the control group in all four conditions (Table 2, descriptive statistics).
In this study, we performed posturography under four conditions in PPPD patients and a control group to investigate the characteristics of body equilibrium in PPPD patients. The results of this study suggest that PPPD patients have higher postural instability and dependence on visual input in a standing posture than healthy subjects. In addition, PPPD patients tended to have lower dependence on somatosensory input in a standing posture than healthy subjects.
Postural instability in PPPD patients has been previously reported. In one study, the EquiTest® Sensory Organization Test was performed in 20 PPPD patients, 15 patients with complete recovery from acute peripheral dizziness, and 15 healthy subjects [29]. The PPPD group showed significantly lower scores than the other two groups not only when multiple sensory input were disrupted, but also when a single sensory input was disrupted. Another study using the sensory organization test revealed greater anterior-posterior sway associated with dependence on visual input and greater medial-lateral sway in low demand conditions than healthy subjects [20]. Then, PPPD patients showed significantly higher COP velocity values and COP area values compared to healthy subjects in postural sway analysis with rotating dots [8]. However, previous studies have not examined vestibular function in PPPD patients, and it is unclear whether there are posturographic features of PPPD that are independent of vestibular function. In our study, we divided the PPPD patients into four groups based on the findings of vestibular function tests and compared the results of the posturography test.
In foam posturography, Romberg’s ratio, which reflects dependence on visual input in a standing posture, tends to be higher in patients with peripheral vestibulopathy and the foam ratio, which reflects dependence on somatosensory input while in a standing posture, tends to be higher in patients with peripheral vestibulopathy [13]. Although statistical comparisons could not be made in this study due to the small number of subjects in each group, the median Romberg’s ratio of PPPD patients tended to be higher than that of normal subjects, even when their vestibular function was normal. It was also shown that the median foam ratio of PPPD patients tended to be lower than that of normal subjects, even when they had vestibular dysfunction. Higher dependence on visual and lower dependence on somatosensory input may be a characteristic of PPPD, which is not affected by vestibular function. However, a more detailed statistical analysis is needed to draw conclusions.
In our study, the PPPD group showed significantly larger median Romberg’s ratios than the control group. The PPPD patients experienced a greater degree of deterioration in standing posture when visual input was blocked by eye closure compared to the normal subjects. PPPD patients may be more dependent on visual input in a standing posture. A previous functional magnetic resonance imaging study showed that activity in response to visual stimulation in the visual cortex in PPPD patients correlated with severity of dizziness handicap [27]. Another functional magnetic resonance imaging study revealed higher levels of neuroticism in PPPD patients were associated with increased activity in the inferior frontal gyrus, and enhanced connectivity between the inferior frontal gyrus and visual regions in the response to visual stimulation [24]. The inferior frontal gyrus mediates functional coupling between motor and visual cortex [23]. PPPD patients are thought to be susceptible to visually induced dizziness by reweighting the processing of vestibular, visual, and somatosensory information in favor of visual input [7, 31]. Collectively, PPPD patients are more sensitive to visual stimuli, suggesting that the exacerbation of dizziness by visual stimuli in PPPD patients may be due to the enhancement of brain networks.
The foam ratio reflects dependence on somatosensory input while standing. In our study, the PPPD group showed significantly lower median foam ratios than the control group. PPPD patients may be less dependent on somatosensory input while standing. Previous research has shown an association between higher space-motion discomfort, a disorder related to PPPD, and an increased dependence on somatosensory information for postural control in patients with anxiety [17]. Our study compared a group of PPPD patients with healthy subjects, and the difference in the results regarding dependence on somatosensory input between the previous study and ours may be due to a difference in the selection of the control group to be compared with the patient group. The reason for lower dependence on somatosensory input from the lower limbs in PPPD patients in the standing posture is unknown. Phobic postural vertigo, a classic disease concept with clinical features similar to PPPD, has been reported to present with increased swaying in the 3.53–8 Hz frequency band when standing on a foam rubber [18]. Standing on the foam rubber creates a maladaptive persistent perception in PPPD patients. Situations that may threaten postural stability may cause PPPD patients to alter their postural control strategies during upright standing and perpetuate persistent vertigo symptoms [5]. However, the present study showed that the foam ratio was smaller in PPPD patients than healthy controls, i.e., the increase in body sway due to standing on the foam rubber was rather small. Further research is needed on the effect of the somatosensory input on postural control in PPPD.
We acknowledge there are several limitations in this study. First, the present study is retrospective, and the possibility of a selection bias is present. Second, an institutional bias might exist because the institution that collected data on the PPPD patients was different from the institution that collected data on the healthy subjects. Third, the present study had a small number of cases and did not examine the effect of other factors on the posturographic findings such as the duration of PPPD or preceding conditions that cause balance disorders. Fourth, amplitude of cVEMP was not corrected by background muscular activity of sternocleidomastoid muscle and that this might affect the AR values in this study. Fifth, we did not perform vestibular function tests, including VEMP or vHIT, on the healthy subjects in our study. Sixth, we did not consider the uncertainty of intraindividual reliability of Romberg’s ratios [32]. Seventh, type 1 errors may exist because many tests were performed in this study.
Conclusion
In a standing posture, PPPD patients may be more dependent on visual input and less dependent on somatosensory input than healthy subjects. Higher dependence on visual and lower dependence on somatosensory input in PPPD may be a feature unaffected by vestibular function.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author contributions
K.I., M.O., T. Kawahara and C.F. contributed to conception and design of the study. K.I. organized the database, performed the statistical analysis, and wrote the first draft of the manuscript. T. Kawahara and I.T. made important contributions in the statistical analyses. K.I., M.O., K.K., T. Kamogashira, M.K., K.S., C.F. and S.D. contributed to data acquisition. C.F. and T.Y. revised the manuscript for research design and important intellectual content. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This study was funded by JSPS KAKENHI Grant Number 21H03083 and 22H03662.
Footnotes
Acknowledgments
We are deeply grateful to Toshiko Nishi, Mami Nagatoishi, Ryohei Harada and Mai Yashima for assistance with data collection.