
Abstract
BACKGROUND:
The upright head roll test (UHRT) is a recently introduced diagnostic maneuver for lateral semicircular canal benign paroxysmal positional vertigo (LSC-BPPV).
OBJECTIVE:
This study aimed to evaluate the reliability and validity of the UHRT.
METHODS:
Two separate studies were conducted. Study 1 analyzed 827 results of videonystagmography (VNG) to assess UHRT reliability, and Study 2 analyzed 130 LSC-BPPV cases to evaluate UHRT validity.
RESULTS:
The inter-test reliability between UHRT and the supine head roll test (SHRT) showed substantial agreement (Cohen’s kappa = 0.753) in direction-changing positional nystagmus (DCPN) and almost perfect agreement (Cohen’s kappa = 0.836) in distinguishing the direction of DCPN. The validity assessment of UHRT showed high accuracy in diagnosing LSC-BPPV (80.0%) and in differentiating the variant types (74.6%). UHRT was highly accurate in diagnosing the canalolithiasis type in LSC-BPPV patients (Cohen’s kappa = 0.835); however, it showed only moderate accuracy in diagnosing the cupulolithiasis type (Cohen’s kappa = 0.415). The intensity of nystagmus in UHRT was relatively weaker than that in SHRT (P < 0.05).
CONCLUSION:
UHRT is a reliable test for diagnosing LSC-BPPV and distinguishing subtypes. However, UHRT has a limitation in discriminating the affected side owing to a weaker intensity of nystagmus than SHRT.
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common type of vertigo [12, 25], followed by lateral semicircular canal (LSC) benign paroxysmal positional vertigo (BPPV), occurring in 1.9– 22% of vertigo cases [2]. The most commonly used diagnostic test for LSC-BPPV is the supine head roll test (SHRT), also called the Pagnini– McClure maneuver [12, 21]. In the SHRT, the head is bent forward approximately 30° in the supine position and is then turned 90° to observe the nystagmus for approximately 30 s. The contralateral side is assessed in the same way. Two variants of nystagmus can be observed in the presence of LSC-BPPV, geotropic and apogeotropic [11, 21]. When the otoconia is located in the posterior arm of the LSC, the debris moves toward the ampulla because of gravity when the head is turned, stimulating the ampullary receptor. Geotrophic direction-changing positional nystagmus (DCPN) can be observed transiently at this time. Conversely, when otoconia occurs in the ampullary arm of the LSC or adheres to the cupula, ampullofugal flow of endolymph occurs due to gravity, resulting in apogeotrophic DCPN [15]. The lesion side can be determined by comparing the amplitude of nystagmus. According to Ewald’s law, the side with stronger nystagmus is the lesion side in the geotrophic variant, while the side with weaker nystagmus is the lesion side in the apogeotrophic variant [26]. Moreover, the ‘bow and lean test’ (or ‘Choung’s test’) can be helpful in confirming the lesion side of LSC-BPPV. However, the SHRT and bow and lean test must be performed together because the latter itself cannot differentiate between canalolithiasis and cupulolithiasis variants.
Recently, a method for diagnosing LSC-BPPV was proposed by Martellucci et al. This ‘upright BPPV protocol’ combines three maneuvers that can be performed in a sitting position: the upright head roll test (UHRT), pseudo-spontaneous nystagmus test, and head pitch test [18, 19]. While the pseudo-spontaneous nystagmus test and head pitch test are well-known, UHRT is introduced for the first time in this protocol. UHRT, which involves simply rolling the head from side to side while in a sitting position, stimulates the cupula of the lateral canal through a mechanism similar to that of SHRT. Therefore, UHRT and SHRT are believed to induce similar nystagmus. However, the initial study introducing UHRT involved only 12 cases [18], and a subsequent study compared the reliability with that of the upright BPPV protocol [19]. Consequently, a direct comparison with SHRT is necessary to fully understand the characteristics of the newly introduced UHRT. Additionally, both previous studies had limitations in that they did not produce objective videonystagmography (VNG) results.
Therefore, the current study was conducted to evaluate the reliability and validity of UHRT compared to SHRT. Study 1 evaluated the test reliability based on VNG results. Study 2 assessed the UHRT validity in cases of confirmed diagnosis of LSC-BPPV based on symptoms and VNG results.
Methods
Videonystagmography
\enlargethispage 2pt
A total of 5,817 VNG tests was performed at a tertiary referral center from January 2014 to June 2021 using VisualEyes (Interacoustics, Middelfart, Denmark) for screening. Even before the introduction of UHRT, our hospital’s VNG protocol included a maneuver involving rolling the head right and left while in a sitting position, similar to the UHRT method. Therefore, UHRT and SHRT were performed simultaneously in all our VNG recordings. Nystagmus was recorded for a duration of 10 s in each direction for every position. During the SHRT, the subject’s head was rotated 90° to both sides while in the supine position, and nystagmus was recorded in the yaw plane. For the UHRT, the subject was seated, the head was tilted to each side, and the nystagmus was recorded in the roll plane. Nystagmus intensity was defined as the maximum slow-phase velocity (SPVmax) measured in degrees per second after each diagnostic maneuver. Nystagmus observed during the transition from one position to another was ignored [20].
Study 1. Reliability assessment: Method comparison between the UHRT and SHRT
Among 5,817 VNG results, we extracted 1,452 VNG results with any type of nystagmus observed in the SHRT or UHRT. The results with non-horizontal nystagmus (n = 25) or with intensity of nystagmus less than SPVmax 3°/s (n = 600) were excluded based on the definition of pathologic nystagmus [9]. After screening, the VNG results of 827 participants were used for analysis in Study 1. Reliability analysis was conducted by assessing agreement of the SHRT and UHRT using Cohen’s kappa statistics.
Study 2. Validity assessment: UHRT diagnostic accuracy
Of the 827 individuals analyzed in Study 1, 232 demonstrated DCPN and were suspected of LSC-BPPV. Their medical records including age, sex, and dizziness symptoms were retrospectively reviewed to confirm the diagnosis of LSC-BPPV, defined as repeated episodes of vertigo with changes in head position relative to gravity and the presence of DCPN on the SHRT [1]. Patients with a central lesion causing dizziness were excluded. A total of 130 patients was confirmed to have LSC-BPPV and were included in Study 2. Validation assessment was performed based on the diagnostic accuracy of UHRT by comparing the final diagnosis based on symptoms and the SHRT. Cohen’s kappa was used for statistical analysis.
The participant enrollment of Studies 1 and 2 is summarized in Fig. 1.
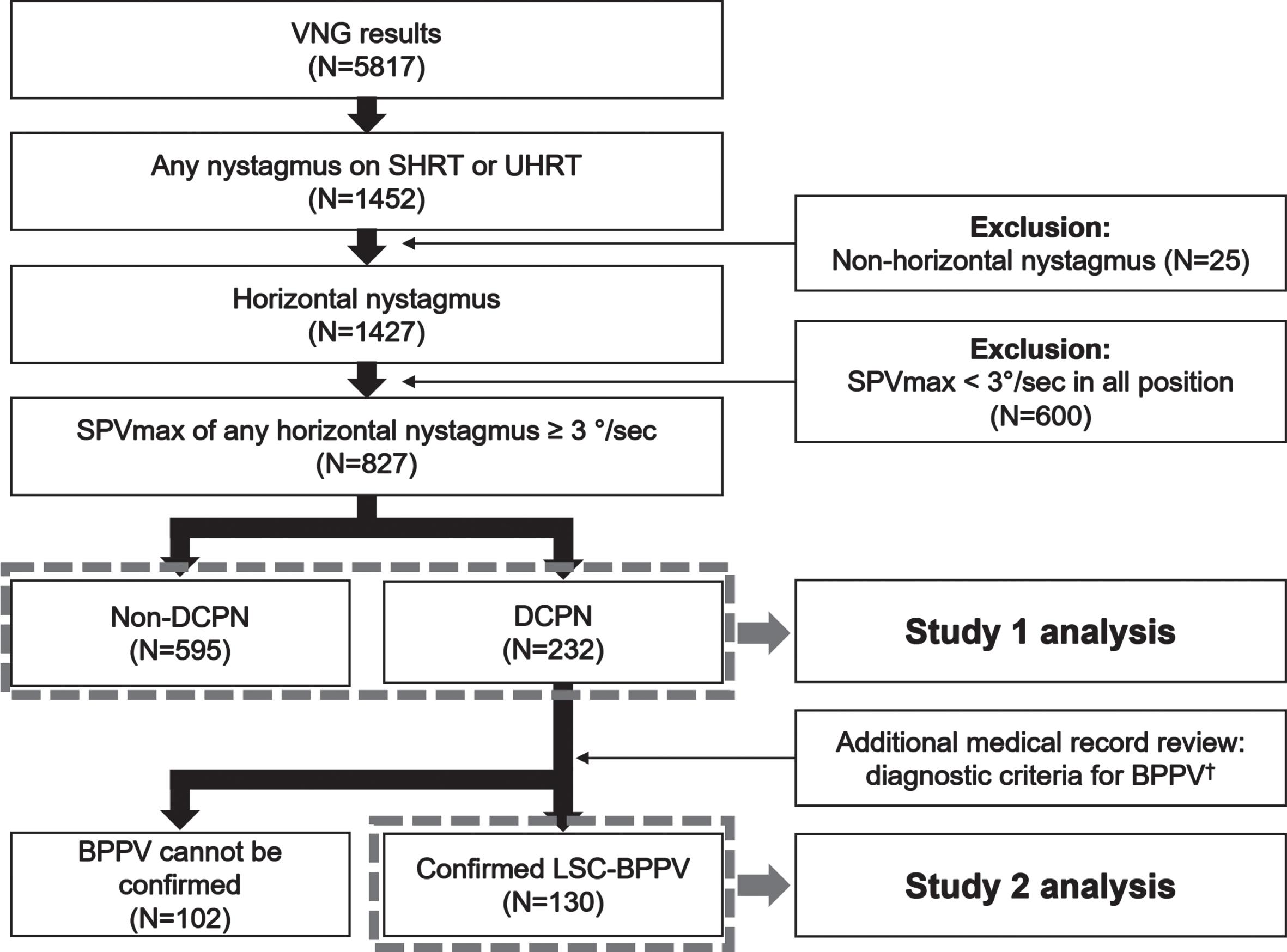
Flowchart of patient inclusion in data analysis. The reliability of UHRT was investigated through inter-test agreement in Study 1, while validation analysis based on LSC-BPPV-confirmed patients was conducted in Study 2. † Repeated episodes of vertigo with head movement and the presence of DCPN on SHRT. (VNG, videonystagmography; SHRT, supine head roll test; UHRT, upright head roll test; SPVmax, maximum slow-phase velocity; DCPN, direction-changing positional nystagmus; LSC-BPPV, lateral semicircular canal benign paroxysmal positional vertigo).
Both agreement and accuracy were calculated by Cohen’s kappa statistics, and categories of Landis and Koch were used, with values of 0.81 to 1.00 indicating almost perfect, 0.61 to 0.80 indicating substantial agreement, 0.41 to 0.60 indicating moderate agreement, 0.21 to 0.40 indicating fair agreement, and 0.00 to 0.20 indicating poor agreement [14]. Independent sample t-test and Chi-square test were used to compare the demographic data and the velocity of nystagmus. Statistical analysis was performed using Excel (Microsoft Cooperation, Redmond, WA, USA) and SPSS version 24 (SPSS Inc., Chicago, IL, USA). P-values < 0.05 were considered statistically significant.
Ethical approval
The study was approved by the Ethical Committee of Seoul St. Mary’s Hospital (KC22RISI0075). This study was a retrospective cross-sectional analysis of publicly available information; therefore, requirement of informed consent from participants was waived by the Ethics Committee of the Medical Governance Research Institute. This study was performed in accordance with relevant guidelines and regulations.
Demographic data of Study 1
Demographic data of Study 1
*Unpaired t-test for age and Chi-square test for gender and pathologic side. †Direction of the DCPN was determined by SHRT in case of opposite result between SHRT and UHRT. ††Pathologic side was determined by SHRT in case of opposite result between SHRT and UHRT. (DCPN, direction-changing positional nystagmus; SHRT, supine head roll test; UHRT, upright head roll test).
Study 1
Demographic data
On the SHRT or/and UHRT, 232 patients showed DCPN, while 595 patients did not. The mean±standard deviation age of the DCPN group was 59.2±14.1 years, which was significantly older than the 54.7±15.5 years of the non-DCPN group (P < 0.001). The female ratio was higher in the DCPN group (82/232, 64.7%) than in the non-DCPN group (334/595, 56.1%), with a significant difference (P < 0.05).
Among 232 DCPN patients, geotropic variants (canalolithiasis type LSC-BPPV) were identified in 52 (22.4%) and apogeotropic variants (cupulolithiasis type LSC-BPPV) were identified in 181 (77.6%) based on the SHRT as a gold-standard diagnostic maneuver. There were no statistical differences in age, sex, or pathologic side effects according to type of LSC-BPPV (Table 1).
Agreement assessment between the SHRT and UHRT
Agreement assessments between the SHRT and UHRT were performed and defined as ‘positive’ when DCPN was observed and ‘negative’ when another type of nystagmus was observed or nystagmus was absent. Among the 827 patients, the positive rate on the SHRT was 26.5% (219/827), and that on the UHRT was 20.7% (171/827). The percentage of agreement was 91.1% and the percentage positive agreement was 81.0% between the two tests. In addition, the inter-test reliability for the two tests was ‘substantial agreement,’ with a Cohen’s kappa of 0.753 (Table 2a).
Method comparison between UHRT and SHRT
Method comparison between UHRT and SHRT
*Interpretation according to the Landis and Koch scale. aAmong the 36 patients with geotropic nystagmus in both supine and upright head roll test, 29 patients were analyzed excluding 7 patients who could not determine the pathologic side due to the same nystagmus velocity. bAmong the 112 patients with geotropic nystagmus in both supine and upright head roll test, 72 patients were analyzed excluding 40 patients who could not determine the pathologic side due to the same nystagmus velocity (DCPN, direction-changing positional nystagmus; UHRT, upright head roll test; SHRT, supine head roll test).
The direction of nystagmus between the two tests was analyzed by geotropic and apogeotropic DCPN. Among the 232 patients who showed a positive result in the SHRT or/and UHRT, 148 (63.7%) showed the same direction, 61 (26.3 %) showed DCPN only on the SHRT, 13 (5.6%) showed DCPN only on the UHRT, and 10 patients (4.3%) showed opposing directions.
Statistical analysis of DCPN directional agreement was conducted among the 158 patients with positive results in both tests. The percentage agreement of the two tests was 93.7%, and the inter-test reliability was ‘almost perfect,’ with a Cohen’s kappa of 0.836 (Table 2b).
In the geotropic variant cases, after excluding seven cases whose SPVmax of nystagmus showed some intensity, 29 patients were included in the analysis. In the apogeotropic variants, 72 patients were included in the analysis after omitting 40 in whom the dominant side could not be determined. In the geotropic variant cases, the percentage agreement was 62.1% and the inter-test reliability was ‘fair,’ with a Cohen’s kappa of 0.283. In the apogeotropic variant cases, the percentage agreement was 63.9% and the inter-test reliability was ‘fair,’ with a Cohen’s kappa of 0.275 (Tables 2c and 2d).
Demographic data
The clinical demographics of Study 2 are presented in Table 3. No significant variation was observed in the demographic factors.
Demographic data of Study 2
Demographic data of Study 2
*Unpaired t-test for age and Chi-square test for gender and pathologic side. (LSC-BPPV, lateral semicircular canal benign paroxysmal positional vertigo; ISSNHL, idiopathic sudden sensorineural hearing loss; SCDS, superior canal dehiscence syndrome).
Among the 130 patients diagnosed with LSC-BPPV, 104 (80%) demonstrated DCPN during the UHRT, while the remaining 26 (20%) patients showed no nystagmus in the UHRT. In terms of LSC-BPPV variant type, 97 patients (74.6%) showed the same diagnosis as the SHRT, with 23 patients were diagnosed with canalolithiasis and 74 patients were diagnosed with cupulolithiasis. Conversely, seven patients (5.4%) showed opposing variant types, all of whom showed geotropic DCPN in the SHRT and apogeotropic DCPN in the UHRT. The diagnostic accuracy, including both LSC-BPPV type and affected side, was 44.6% (58/130). Of the 23 patients diagnosed with the canalolithiasis type of LSC-BPPV by both tests, 14 showed the same affected side, five were diagnosed with opposing side type, and four were unable to be diagnosed regarding the affected side using the UHRT. Among the 74 patients diagnosed with cupulolithiasis type of LSC-BPPV, 44 showed concordance with the affected side, 17 showed opposing side effects, and 13 were undetermined for direction using the UHRT. The results are shown in Fig. 2.

Diagnostic accuracy of the UHRT. Among the 130 patients, LSC-BPPV was identified in 80% (104/130) based on the UHRT, while 26 patients (20%) showed no nystagmus. Diagnostic accuracy in term of LSC-BPPV type (canalolithiasis or cupulolithiasis) was 75% (97/130). Diagnostic accuracy including both variant type and affected side was 45% (58/130). (UHRT, upright head roll test; LSC-BPPV, lateral semicircular canal benign paroxysmal positional vertigo.)
The diagnostic accuracy of patients with canalolithiasis and cupulolithiasis types of LSC-BPPV was analyzed respectively. Diagnostic accuracy of the canalolithiasis type was 94.6% (123/130) and Cohen’s kappa was 0.835 (almost perfect agreement). In addition, diagnostic accuracy in the cupulolithiasis type was 74.6% (97/130) and Cohen’s kappa was 0.415 (moderate agreement). Detailed results of the diagnostic accuracy assessment are presented in Table 4.
Diagnostic accuracy assessment of UHRT
*Interpretation according to the Landis and Koch scale. a All seven patients showed apogeotropic direction-changing positional nystagmus (DCPN) in UHRT. b All seven patients showed geotropic DCPN in SHRT. c All 26 patients showed no nystagmus in UHRT. (UHRT, upright head roll test; SHRT, supine head roll test.
The intensity of nystagmus (SPVmax results calculated by VNG) was compared and statistically analyzed in 97 patients who showed the same direction of DCPN in both tests. The mean SPVmax of the SHRT was significantly greater than that of the UHRT regardless of side (stronger or weaker) (P < 0.001). SPVmax values showed significantly greater differences between the stronger side and the weaker side in the SHRT (P = 0.003). In the geotropic type, SPVmax of the SHRT was larger than that of the UHRT on both stronger and weaker sides, although the difference was not significant (P > 0.05). In the apogeotropic type, SPVmax of the SHRT was significantly larger than that of the UHRT (P < 0.001). SPVmax differences were larger with the SHRT in both geotropic and apogeotropic types of LSC-BPPV. Detailed results are presented in Table 5.
Comparison of nystagmus intensity between 97 patients who had direction-changing positional nystagmus on both supine and upright head roll tests
Comparison of nystagmus intensity between 97 patients who had direction-changing positional nystagmus on both supine and upright head roll tests
Nystagmus intensity was defined as maximum slow-phase velocity (SPV, degree per second) and all data presented as mean and 95% confidence interval. P-values were calculated using the paired t-test. (UHRT, upright head roll test; SHRT, supine head roll test; LSC-BPPV, lateral semicircular canal benign paroxysmal positional vertigo.).
Nystagmus intensity was defined as maximum slow-phase velocity (SPV, degree per second) and all data presented as mean and 95% confidence interval. P-values were calculated using the paired t-test. (UHRT, upright head roll test; SHRT, supine head roll test; LSC-BPPV, lateral semicircular canal benign paroxysmal positional vertigo.).
The purpose of this study was to evaluate the reliability and validity of the UHRT as a diagnostic method for LSC-BPPV. Despite its potential as a simple and accessible outpatient test, the lack of evidence regarding its reliability has limited itsuse [18].
The overall inter-test reliability between the UHRT and SHRT showed substantial agreement (Cohen’s kappa = 0.753). Specifically, agreement of DCPN direction was almost perfect (Cohen’s kappa = 0.836), although agreement in distinguishing the dominant side of nystagmus was fair, both in geotropic type (Cohen’s kappa = 0.283) and apogeotropic type (Cohen’s kappa = 0.275). Additionally, using a cohort of patients diagnosed with LSC-BPPV, we evaluated the validity of the UHRT. The results showed high accuracy in diagnosing LSC-BPPV and differentiating variant types; however, the diagnostic accuracy of both variant types and affected side was relatively low. Specifically, the diagnostic accuracy of the UHRT in canalolithiasis type LSC-BPPV patients was almost perfect (Cohen’s kappa = 0.835), whereas the diagnostic accuracy of UHRT in the cupulolithiasis type was moderate (Cohen’s kappa of 0.415). Overall, these findings suggest that the UHRT may be a viable alternative to the SHRT for diagnosing LSC-BPPV; however, its limitations in distinguishing the affected side should be considered.
The limitation of the UHRT in confirming the affected side is attributed to the smaller SPVmax in the UHRT compared to SHRT. In geotropic variants (canalolithiasis type), the greater is the acceleration of otolith movement by gravitational force produced with head movement, the stronger is the endolymph flow that induces cupula deflection, resulting in higher intensity nystagmus [5]. Lim et al. [17] reported larger SPVmax of nystagmus when the SHRT was performed at 180° rather than at 90° in geotropic variants of LSC-BPPV. They explained their result using a biomechanical model. Based on their model, we investigated the cause of the difference in nystagmus intensity between the UHRT and SHRT. The gravitational potential energy (Ep) of the otoliths could be calculated using the following formula:
(g = gravitational acceleration, m = mass of otolith, h = otolith height from the lowermost part of the SCC).
In cases of canalolithiasis type LSC-BPPV, the otolith height is larger in the SHRT than in the UHRT. As otoliths descend due to gravity, potential energy is converted into kinetic energy. Consequently, in the SHRT, where there is greater potential energy, a faster velocity of endolymphatic flow is induced.
Furthermore, in a case of cupulolithiasis, the force induced by the otolith on the cupula varies based on the angle between the cupula and gravity, as described by the formula below.
(F = force of otolith movement, G = gravity force, θ= angle between gravity and cupula).
In cases of canalolithiasis type LSC-BPPV, the angle between gravity and the cupula is greater during the SHRT than during the UHRT. As a result, the force of otolith movement is stronger in the SHRT than in UHRT. The biomechanical models comparing UHRT and SHRT are presented in Fig. 3.

Biomechanical models comparing the supine head roll test (SHRT) and the upright head roll test (UHRT). In the case of the right-side canalolithiasis type, the UHRT exhibits lower gravitational potential energy (Ep) owing to the otolith’s shorter height from the lowermost part of the semicircular canal. In the case of right-side cupulolithiasis type, the angle (θ) between gravity and the cupula is smaller in the UHRT condition, inducing smaller endolymphatic flow (h = otolith height from the lowermost part of the semicircular canal, g = gravitational acceleration, G = gravity force, F = otolith movement force, θ= angle between gravity and the cupula).
Differentiation of the affected side in LSC-BPPV can be challenging, even with the SHRT [4, 23]. Thus, additional maneuvers have been introduced to improve diagnostic accuracy. The ‘lying down nystagmus’ proposed by Koo et al. is well known for effectively determining the affected side of LSC-BPPV [13]. Choung et al. [3] proposed the bow and lean test (or head pitch test) as an additional method to distinguish the affected side.
In our study, the UHRT was less effective in discerning the affected side compared to the SHRT. Therefore, it would be desirable to perform additional maneuvers alongside the UHRT to confirm the affected side in patients with LSC-BPPV. In this context, the upright BPPV protocol proposed by Martellucci et al. appears to be a rational approach for diagnosing LSC-BPPV [19]. Their protocol comprises the pseudospontaneous nystagmus test, bow and lean test, and the UHRT. It can be comfortably performed in a seated position, offering an accessible approach for diagnosing LSC-BPPV [16]. Moreover, it compensates the limitations of the UHRT by incorporating additional maneuvers.
Our study has several strengths. It is the first to analyze the inter-test reliability and diagnostic validity of the UHRT using a large number of VNG results and clinical data. Additionally, we conducted a quantitative comparison of nystagmus intensity and provided a biomechanical model to explain why nystagmus is weaker in the UHRT than in the SHRT.
Our study also has some limitations. First, additional maneuvers, such as the bow and lean test and/or pseudo-spontaneous nystagmus, which can be used to determine pathological sides, were not included in this analysis. In the study by Martellucci et al. [20], the UHRT was introduced as one of the maneuvers comprising the upright BPPV protocol, along with the bow and lean test and pseudo-spontaneous nystagmus. Since our VNG protocol does not include the bow and lean test and pseudo-spontaneous nystagmus, our approach is unable to verify the reliability of the entire upright BPPV protocol. However, unlike the renowned bow and lean test and pseudo-spontaneous nystagmus [1, 4], the UHRT is a relatively new maneuver that is not yet widely recognized. Thus, our study is significant for contributing to the understanding of its reliability and characteristics. Second, the number of canalolithiasis type patients was relatively small, despite a previous report that canalolithiasis types are more common than cupulolithiasis types [2]. This could be attributed to the retrospective VNG results from a tertiary referral hospital used in our study. The canalolithiasis type of LSC-BPPV has a higher likelihood of spontaneous resolution and a better success rate for repositioning maneuvers [22], which may have led to omission of such patients from our study. Furthermore, a one-week delay occurred between the initial patient visit and VNG testing, allowing the possibility that the patient condition may have changed. Third, the nystagmus recording time in the VNG used was short, preventing the differentiation between persistent and transient DCPN. For positional tests, if nystagmus persists for more than one or two minutes, it can be categorized as persistent nystagmus [8, 10]. Among patients with horizontal DCPN, approximately 5– 15% exhibit a persistent variant [10, 24]. The pathophysiology of persistent DCPN has not been fully established. Nevertheless, geotropic persistent DCPN can be explained by the light cupula theory, while apogeotropic persistent DCPN can be explained by the heavy cupula theory [24]. The presence of light or heavy cupula can be observed in cases of persistent DCPN a with null plane [7, 10]. Nonetheless, the VNG results used in our study did not include such information. In this study, owing to the inability to distinguish between persistent and transient types, a limitation existed in analyzing how the UHRT may differ in patients with light cupula or heavy cupula.
Despite its limitations, our study is meaningful in that it provides insights regarding the UHRT as a novel diagnostic maneuver for LSC-BPPV that can be easily performed in the clinic. We suggest that UHRT can be applied clinically as a simple means of identifying LSC-BPPV. For example, if a patient has already received treatment for LSC-BPPV and subjective symptoms have improved, it is not necessary to determine the pathologic side, only persistence of LSC-BPPV. In this case, the UHRT can reduce the discomfort of the patient and the effort of the physician. Second, the UHRT can be used in patients with phobia of vertigo. Severe dizziness can accompany maneuvers provoking positional nystagmus and might become a persistent psychogenic condition if the maneuvers are repeated [6]. However, since the UHRT has a relatively weak intensity of nystagmus, it can minimize patient dizziness. Third, the UHRT can be used if the SHRT is difficult to perform, such as in patients with cervical stenosis, severe kyphoscoliosis, limited cervical range of motion, or Down’s syndrome [22]. The URHT can be performed simply in patients with physical limitations, and identification of the pathologic side can be achieved using maneuvers performed in the sitting position, such as the bow and lean test and/or pseudo-spontaneous nystagmus. Therefore, the upright BPPV protocol introduced by Martellucci et al. appears to be a reasonable method for diagnosing LSC-BPPV.
The UHRT, which can be performed simply in a sitting position, is reliable in diagnosing LSC-BPPV and discriminating subtypes. However, the UHRT has a limitation in distinguishing the pathologic side. Therefore, use of additional maneuvers, such as the bow and lean test and/or pseudo-spontaneous nystagmus, should be considered when using UHRT for diagnosing LSC-BPPV.
Footnotes
Acknowledgments
The authors would like to thank Professor Saeyong Chae, who established the VNG protocol, including the UHRT, more than 10 years ago.