
Abstract
Introduction
Musculoskeletal disorders
Work-related musculoskeletal disorders (WMSDs) characterize a broad range of illnesses affecting mainly soft tissues. They are the most common causes of pain, work absence, early retirement, disability, and death worldwide in the working population [1]. This topic has been recognized as a priority research area in various occupations in recent years.
Researchers have considered musculoskeletal complaints as a common occupational health problem and a significant threat to nurses’ health. Widespread back injuries have been reported among home health care nurses due to their specific job features, which influence the adoption of risk behaviors [2]. Previous study found a disproportionate incidence of back and lower limb disorders among Japanese hospital nurses [3]. In a survey carried out among registered nurses working for at least one year in New York and Illinois, the prevalence rates of musculoskeletal symptoms in the neck, shoulder, and back (47%) were reported 46%, 35% and 47%, respectively [4].
Risk factors
Most studies have consistently documented that the working conditions and intensity of job stressors would likely lead to musculoskeletal injuries [5–9]. Etiologic studies have proposed numerous risk factors frequently associated with musculoskeletal complaints. These are awkward work posture, manual handling of heavy loads, repetitive movements, forceful exertion, job stress, work scheduling, long working hours and individual characteristics [10–13]. Literature reviews have commonly categorized risk factors for musculoskeletal symptoms into physical, individual and psychosocial stressors.
Results of studies have provided evidence that physical job demands in nursing contribute to an increased risk of musculoskeletal symptoms. In general, nursing profession often involve extreme and sudden body postures of bending, twisting and lifting of heavy loads. Such demands may increase the risk of developing musculoskeletal complaints [14].
Psychosocial factors are broad and encompass non-physical areas of work. Such factors include psychological workload, job satisfaction, perceived fatigue, and the relationship between colleague and management. There has been less investigation into the contribution of psychosocial factors to the development of musculoskeletal symptoms. However, literature has reported empirical support for the direct and indirect roles of psychosocial factors in developing musculoskeletal complaints [15]. Mehrdad et al. carried out a research among Iranian nurses in a large hospital applied a questionnaire that includes both task levels and social and organizational factors. They reported a significant association between psychosocial factors and self-reported musculoskeletal symptoms at various body sites among Iraniannurses [16].
Epidemiological research has pointed out that fatigue possibly plays a significant role in musculoskeletal disorders vulnerability. The result proposed evidence for a relation between psychosocial and physical factors with perceivedfatigue [17].
Although researchers have found evidence for the association of Job satisfaction and musculoskeletal symptoms, the results have not been consistent across studies [18]. Research has supported that individual factors such as age, gender and health conditions may contribute to the development of musculoskeletal pains [19].
In overall, findings from studies suggest multiple variables for musculoskeletal disorders. The combined exposure to stressors must be analyzed to understand the cause of the symptoms. Prior studies have mainly examined direct relationships of demographic, psychosocial and work-related factors with musculoskeletal disorders. However, few studies have provided information concerning the interactions of risk factors and the extent of their influence on musculoskeletal disorders.
Structural equation model
A structural equation modeling approach may be used to examine simultaneously both direct and indirect effects of predictive variables on the outcome simultaneously. The method tests hypotheses about the relationships among observed and latent variables incorporating both variables. Beyond identifying linear regression of risk factors, structural analysis statistically evaluates the covariance in various sets of observed and latent variables. Furthermore, this method distinguishes the causal relationship and modeling multivariate relations of variables under study [20]. Structural equation models comprise the analyses of the measurement and structural models. These two conceptually distinct models proposed by Joreskog and Sorbom (2006), who discussed that testing the initial structural model may not be significant unless the measurement model holds [21]. The rationale is that the indicators of a construct must measure that construct before examining the structural relationships [22].
Research objectives
The present research relied upon the conceptual framework that described assumed interactions of work posture, role-related stressors, psychological workloads, fatigue, and job satisfaction influencing musculoskeletal complaints as the outcome (Fig. 1). The purpose was to analyze the direct and indirect associations of various risk factors with musculoskeletal complaints. To this end, we tested a proposed model of musculoskeletal complaints on a sample of Iranian hospital nurses. We also examined the relative importance of risk factors in explaining musculoskeletal complaints. This research is significant since it plays a role in recognizing related components and proposing corrective and preventive actions.
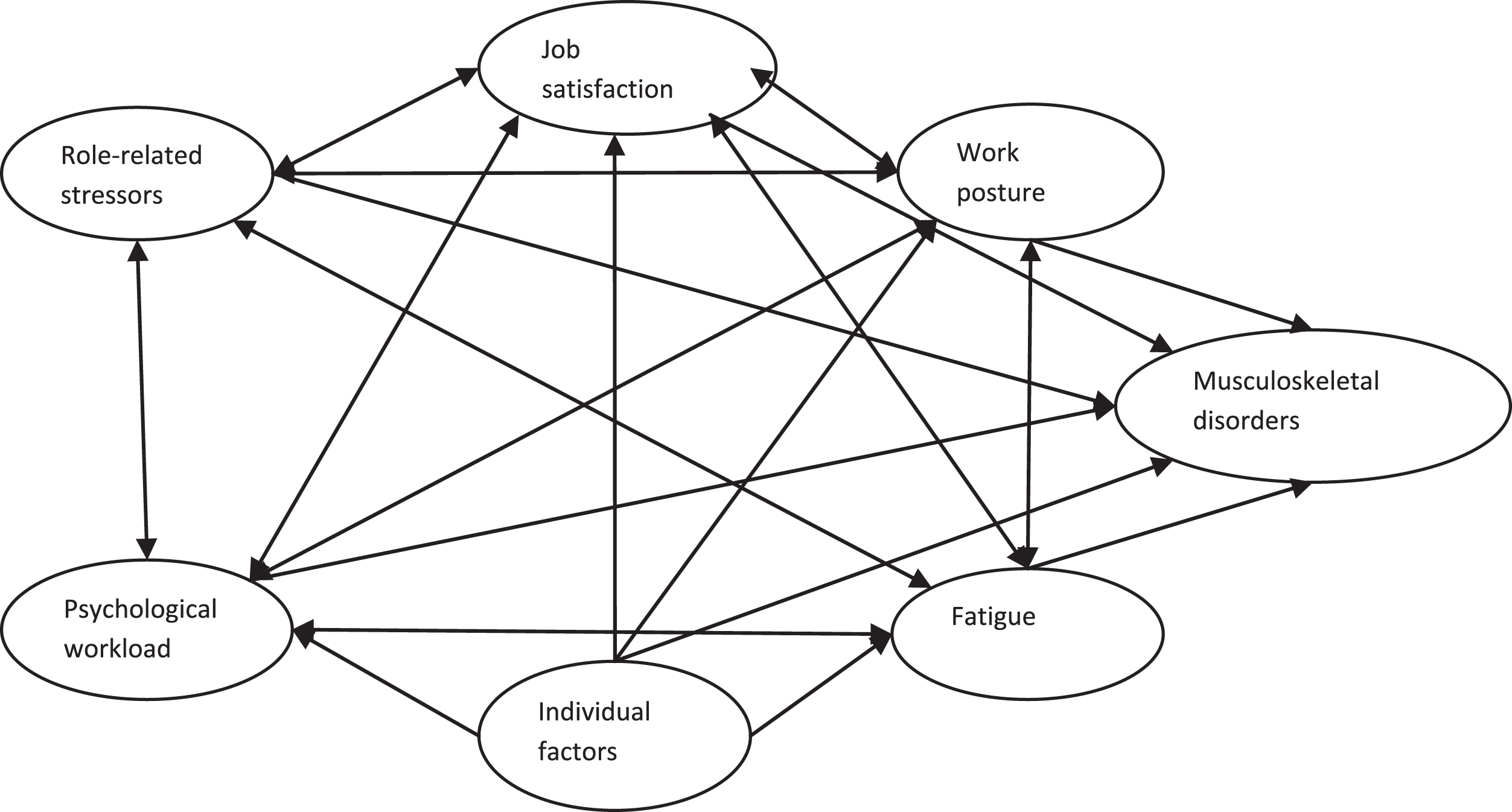
Conceptual framework of the risk factors and musculoskeletal disorders.
Design and sample
In a cross-sectional design based on a questionnaire survey, we invited hospital nurses affiliated to Semnan University of Medical Sciences located in Semnan, Iran, to participate in the study.
The inclusion criteria were working full time in the nursing profession with at least one year of employment, willingness to participate and complete the survey. The target study population was 653 nurses from different hospital wards who participated in a questionnaire survey. Nurses with at least one year of employment, who agreed to participate and complete the survey, were considered eligible for inclusion. The mean age of the participants was 36.2 years old (SD = 19.1). The average length of tenure was 17.4 years (SD = 8.9).
Our study was a registered research project approved by the institutional ethical review board of Semnan University of Medical Sciences. All the participants were asked to provide written informed consent. We assured all nurses about the confidentiality of their responses.
Statistical methods
The proposed model hypothesized to reflect work posture, psychological workload, role-related stressors, and job satisfaction as exogenous latent variables, fatigue as a mediating latent variable, and musculoskeletal complaints as an endogenous dependent variable. Scale items were used as indicators to form the latent constructs.
Cronbach alpha coefficients measured the internal consistency reliability of the survey constructs. Confirmatory factor analyses were performed for the items of latent constructs to confirm the validity of the instrument and the measurement model [22]. We also computed bivariate correlations for all the measured variables to check for multicollinearity. Kline (2011) argues that any pair of observed variables with a correlation higher than 0.85 suggests a potential problem in predicting a latent variable [23].
Structural equation model was calculated to assess the relations among observed and latent variables using maximum likelihood method with LISREL 8.8 version [21]. The model measured linear regression weights for continuous variables. Logistic regression measured the direct effects of variables on musculoskeletal complaints.
A review of the literature indicated no agreement concerning acceptable values for total fit indices. Researchers are recommended to report various fit indices [22]. Chi-square was used to determine how well the proposed theoretical model sufficiently fits our empirical data. A non-significant chi-square suggests that the proposed construct model does fit the sample data but in a large sample size, it commonly may result in a poor fit. A ratio of chi-square divided by the relevant degrees of freedom with a value less than five represents an appropriate fit. Goodness of Fit (GFI) determines the relative amount of the observed variance and covariance explained by the model. A value of GFI more than 0.95 recommends a good fit. The less Standardized Root Mean square Residuals (SRMR) (<0.05), means the lower amount of error and thus represents a better model fit. Mean Square Error of Approximation (RMSEA) corrects the tendency of the chi-square to reject a model. A value of RMSEA lower than 0.05 indicates a good fit. Path coefficients for the hypothesized relationships were computed to evaluate the magnitude and statistical significance of the associations [23].
Studied variables
Participants’ body postures at work were assessed using the self-report questionnaire items based on the Ovako working posture analysis system (OWAS) [24]. Nurses responded to four items including “lifting far from the body”, “bending work performance”, “standing position”, “keeping awkward working position”. Responses based on a five-point Likert scale rating from “never not at all = 1” to “the highest extent = 5”. Finally, the total rating classified as low, moderate and high posture risk. The Cronbach’s alpha was 0.78 for the working posture scale. The result supported the internal consistency reliability for assessing nurses’ perceptions.
This study evaluated nurse’s perception of their psychological workload imposed upon them by the work environment using five observed variables, which focused on “working excessive hours”, “performing more than one job”, “working under time pressure”, and “effort-reward imbalance”. The items in the scale align with Karasek’s job demand-control model [25]. Summing nurses’ rating on the five items yielded the relevant scale scores. Each item had five fixed response options ranging from “not at all” to “a very great degree”. Corresponding Cronbach’s alpha internal reliability was 0.81 that showed a reliable scale.
Role-related stressors were measured using items including “incompatible demands from supervisors” as role conflict and “work- family conflict” as inter-role conflict. There were five fixed response alternatives given points from 1 to 5. The Cronbach’s alpha of the role-related stressors scale was 0.72.
Job satisfaction scale contained three items including “satisfaction of nursing profession”, “enjoys working for the institution” and “positive feelings towards work” [18]. Each item had five fixed response alternatives. The Cronbach’s alpha reliability was 0.62 for the job satisfaction construct.
Research literature has proposed different definitions, and thus different measurement tools of fatigue. This study measured self-reported fatigue using Occupational Fatigue Inventory developed for the measurement of work-related fatigue [26]. We asked nurses about their feeling of fatigue at the end of a work day. The questionnaire consisted of items to measure factors about “lack of motivation” (ex. Passive, indifferent), “sleepiness” (ex. fall asleep, lazy), “lack of energy” (overworked, worn out, exhausted), and “physical effort” (ex. Breathing). The items had five fixed response options ranging from “not at all” to “most of the time”. The Cronbach’s alpha for the fatigue construct was 0.82 considered an internally reliable scale.
Individual variables were years of employment and body mass index (BMI). The latter calculated as the weight divided by the square of the height and classified as underweight, overweight and obesity [27].
A modified Persian questionnaire survey based on the standardized Nordic musculoskeletal questionnaire was applied to measure subjective nurse’s musculoskeletal complaints [28]. We asked nurses to indicate whether they experienced pain or discomfort in ten different body regions during the last one year-period. Criteria for muscular complaints were severity, duration, and frequency of the symptoms. We measured musculoskeletal complaints on a five-point score from “never = 0” to“very often = 5”.
We did confirmatory factor analysis within the measurement model of musculoskeletal complaints. The result indicated that three observed items including back, shoulder, and neck complaints achieved factor loadings higher than 0.4 compared to other parts of body complaints. Therefore, the model included shoulder, neck and back parts of the body, which are mainly exposed to the effects of risk factors, to measure musculoskeletalcomplaints.
Results
Structure of constructs
Confirmatory factor analyses of the constructs identified the subscales for the measurement of work body posture, psychological workload, role-related stressors, individual variables, fatigue, job satisfaction and musculoskeletal complaints.
Measurement model identification and fit statistics
The matrix of correlation coefficients between the pairs of observed variables within latent variables ranged from 0.01 to 0.49 (Table 1). The figures suggest that the measured variables are not too highly related. An examination of model fit on the measurement models was performed to show how observed variables measured each latent variable. Relative low correlations for the observed indicators indicated that the items within latent categories may be used to measure the proposed given construct. Therefore, the items within each group are different but measuring the latent variable.
The matrix of bivariate correlation residuals for all measured variables
The matrix of bivariate correlation residuals for all measured variables
*P < 0.05.
Table 2 shows chi-square values with the relevant degrees of freedom (df), Goodness of Fit Index (GFI), Standardized Root Mean Square Residuals (SRMR), and Root Mean Square Error of Approximation (RMSEA) for each variable in the measurement model and structural model. The fit indices indicate that the proposed model fits the data reasonably.
Hypothesized measurement model fit statistics for each latent variable (Chi-square/degree of freedom, Good of Fit Index, Standardized Root Mean square Residuals, Root Mean Square Error of Approximation)
Using structural equation, we developed a correlation model consisting of the exogenous work body posture, psychological workload, role-related stressors, job satisfaction, the proposed mediating fatigue, and endogenous work-related musculoskeletal complaints. Figure 2 shows the results for the empirical structural model. The factor loadings from the latent constructs to the observable variables revealed the weighting of the measured variables that set the latent construct. All the factor loading estimates were statistically significant suggesting that the items were reliable in measuring their related latent constructs.
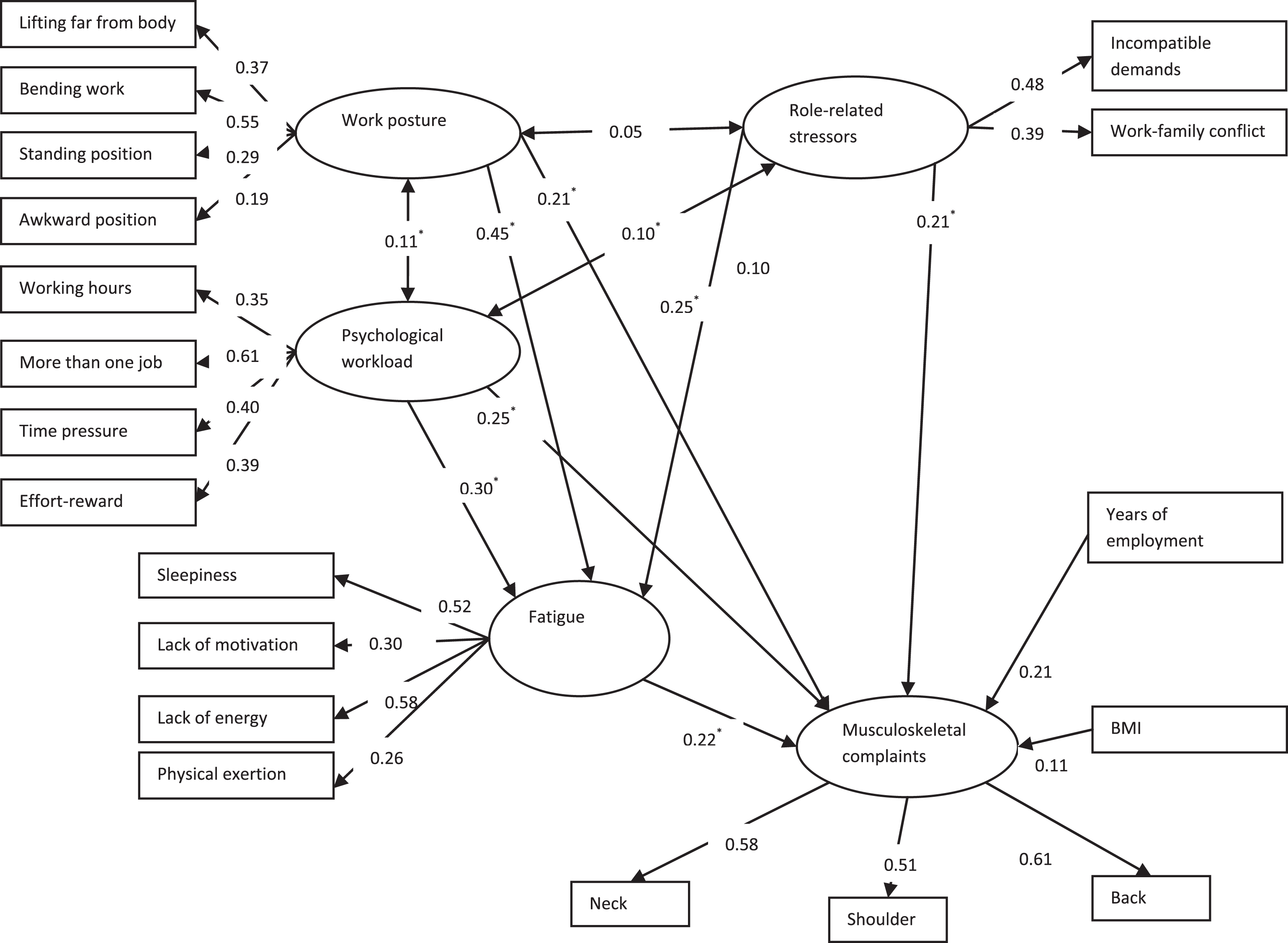
Representation of structural relationships for the empirical model between measures constructs for predicting musculoskeletal complaints from work posture, role related stressors, psychological workload, individual factors, and fatigue. The model test based on self-reported questionnaire data from employed hospital nurses in Semnan, Iran. Rectangles and ovals represent observed and latent variables, respectively. Figures indicate standardized path coefficients estimated for the model. (*p < 0.05; X2/df = 3.01; GFI = 0.94; RMSEA = 0.034).
Paths of standardized regression coefficients determined the extent to which exogenous work body posture, psychological workload, role-related stressors, and individual factors relate to mediating fatigue and dependent work-related musculoskeletalcomplaints. We adjusted the path coefficients between the latent variables for the other latent variables in the proposed model.
The direction of the arrow indicates the direction of the association. The one- headed arrow lines indicate directional effects, whereas the two-headed arrow lines show bivariate correlations between different latent structures. Besides the direct effects which represent the relationship between one latent variable to another, several indirect effects were found via pathway mediated by a latent variable. The total effects measure a sum of the direct and indirect effects between two variables. We examined the direct and indirect effects of the significance and magnitude.
Table 3 highlights the effects of independent (exogenous) variables on dependent (endogenous) variables. Indeed, the path coefficients of the model suggest that for each standard deviation increase in psychological and role conflict stressors, work-related musculoskeletal complaints increased by 0.25 and 0.21, respectively. These results imply that psychological and role-related stressors appear to have had a positive and moderate direct effect on musculoskeletal disorders among nurses. Moreover, psychological workload had a significant and relatively a strong indirect effect of 0.46 on musculoskeletal disorders via mediating variable of fatigue stressor.
Direct, indirect and total effects of study variables on perceived fatigue and musculoskeletal complaints
*P < 0.05.
Role-related stressors had a significant but small indirect effect of 0.12 via fatigue variable on musculoskeletal symptoms. Overall, the more nurses’ perceived psychological workload and role-related stressors, the more they perceived musculoskeletal symptoms. Meanwhile, psychological workload and role-related stressors demonstrated statistically significant positive relationship to each other.
Work body posture had a significant and moderate direct effect of 0.21 as well as a strong indirect effect via fatigue of 0.50 on musculoskeletal disorders. Therefore, the total effect of body posture was strong on the nurses’ perception of musculoskeletal symptoms (0.71). While our study could not find a significant direct effect of the years of employment on musculoskeletal disorders, the result showed a moderate and significant indirect effect of 0.38 via fatigue on musculoskeletal complaints. Thus, the years of employment indicated a moderate total effect on the perception of musculoskeletal complaints.
Psychological stressors showed moderately strong and positive relationship with body posture at work. This means that the more nurses perceived to have greater work posture demands, the more they perceived psychological workload. There were small correlations between independent role-related stressors and work posture and individual factors, thereby indicating almost no association.
We found that psychological stressors had a negative association with Job satisfaction. That means that psychological stressors influenced the extent to which nurses perceived job satisfaction. Thus, probably psychological stressors are a contributing cause of job dissatisfaction. However, Job satisfaction had no significant direct or indirect effects on both dependent fatigue and musculoskeletal symptoms variables when controlling for the effects of psychological stressors. Therefore, we omitted job satisfaction from the model.
This study has been motivated by the widespread interest in better understanding the musculoskeletal disorders in the work environment. Several researchers have focused on the impacts of risk factors and the incidence of musculoskeletal disorders. We applied linear structural relations analysis technique to enable empirical testing of the proposed process model. The method explained the relationships among the risk factors contributed to musculoskeletal symptoms.
In general, the developed structural equation model seemed useful for studying musculoskeletal disorders in occupational settings. Linear structural relations resulted in several direct and indirect associations between perceived variables related to musculoskeletal complaints. The level of associations would explain the relative importance of various risk factors and their inter-relations in developing musculoskeletal disorders. We concluded that the direct and indirect effects are the two mechanisms by which work environment risk factors may affect musculoskeletal complaints.
Musculoskeletal disorders may directly relate to adverse work posture, and psychological workload, and role-related stressors. We found strong support for the hypothesized relationship of work posture on musculoskeletal complaints. The result is consistent with the previous study reported an association between poor work posture and upper- extremity musculoskeletal symptoms [29]. Probably nursing tasks require more reaching and awkward movement and posture. Such demands put nurses at higher risk of musculoskeletal symptoms and injuries. Our finding concurs with earlier studies indicated that the influence of physical factors was greatest in developing of work related musculoskeletal disorders [10, 14].
Our study confirmed that the psychological workloads were related to the musculoskeletal complaints. The finding does confirm previous studies that psychologically stressful work may increase the musculoskeletal symptoms in the neck shoulder and upper and lower back [7, 15].
Role-related stressors were related to the musculoskeletal complaints. That means that the nurses’ perceived stresses due to the conflicts between work and family responsibility and incompatible demands from supervisors might influence their perceptions of musculoskeletal disorders. The result is in line with previous literature suggesting that the role-related stressors are believed to be highly frequent and problematic in a variety of occupations as a result of changing in the work organization andperformance [5].
Additionally, our study provided new findings concerning the indirect links of independent risk factors and musculoskeletal complaints. Fatigue not only caused a strong direct effect, but also partially mediated the relations between work posture, and psychological workload, and role-related stressors with musculoskeletal complaints. The direct and indirect relations indicated that the risk factors had not a unique effect on musculoskeletal symptoms. An interpretation of the results is that the exposure to high levels of psychological stressors and adverse work posture may increase the possibility of musculoskeletal symptoms with first causing fatigue. In a research Parhizi et al. (2013), argued that cumulative fatigue might have a potential link with musculoskeletal symptoms through a reduced capacity for stress. Consequently, decreased threshold stress might cause the muscle tissue fails [30]. Nimbarte et al. (2013) found that self-reported fatigue might result in a reduced position sense perception and by disturbing motor control might cause musculoskeletal disorders [31].
In essence, perceived fatigue as a mediator may explain how occupational and environmental factors affect the health outcome. Potential mediating effect of fatigue may provide evidence that inappropriate posture at work may be hazardous to musculoskeletal system to the level that it causes fatigue. Our finding suggests that after exposure to a high level of physical and psychological stressors, perceived fatigue may be regarded as a warning sign that recovery is needed to prevent the individual from suffering musculoskeletal symptoms and injuries.
In the present study low job satisfaction was not a significant risk for the adverse musculoskeletal outcomes as statistically there was no direct or indirect association. In general, previous researchers examined job satisfaction reported different and contradictory results. Some studies have found support for the association of low job satisfaction with low back pain and neck pain [8, 20]. In contrast, another study indicated no relation between job satisfaction and neck or shoulder symptoms [32]. The result was further in accordance with a review study discussed that the evidence was not consistent across different study designs [24]. Different results may be due to different theories and approaches to define and measure overall job satisfaction. Probably in the previous studies, the instruments applied did not adequately represent the construct.
Above all, the role of job satisfaction should not be ignored because when the symptoms occur, the delayed recovery may be attributed to low job satisfaction [33]. Moreover, our study found support for a correlation between psychological workload and the level of job satisfaction.
The variance in musculoskeletal complaints was explained for 55% by direct and indirect relations with a combination of work posture, psychological workload, role-related stressors, individual factors and perceived fatigue. Therefore, there would be still some room for developing an empirical structural model by taking into account other variables not included in the current study. Our findings revealed that individual factors arising from years of employment and BMI explained only 6% of the variance in musculoskeletal complaints.
There might be limitations with the dataset and the method used in the analyses. We collected data in a cross-sectional design, which limited the analyses of data over a short time and therefore could not establish causality. However, since the model was based on previous theories and study findings, structural equation model analysis may provide an initiative of a causal relationship. Further, the subjects were limited to hospital nurses in a single area of Semnan province. Our results should therefore be validated by longitudinal designs in the nursing context and extended groups of hospitals.
A further limitation was the use of self-reported measures for all the studied concepts. The nurses were asked to recall musculoskeletal pains for a twelve-month period to reduce the risk of a memory bias. However, it might be difficult for them to assess the work-relatedness of their symptoms. Arguably, subjective measures were not related to objective indicators. Thus, the subjects had their theories of causal relationships when answering questions about stressors and symptoms. However, this study supposed validity for the self-reported data because nurses have knowledge about their work environment and challenges. Even so, the result of this study should be confirmed by future research using another method of data collection like objective data.
Conclusion
Structural equation modeling has provided a useful method to develop a comprehensive model representing the relationships between aspects of work environment stressors and musculoskeletal complaints in a relatively large sample of hospital nurses. The proposed empirical structural model fitted the data relatively well and explained around half of the variance.
The results provided compelling evidence of an association between awkward work postures, psychological, and role-related stressors with an increased risk of work-related musculoskeletal symptoms. Additionally, we concluded that perceived fatigue to some extent acts as a mediator between the stressors and musculoskeletal symptoms. We recommend that in any health care and prevention measures attention should be paid to physical and psychosocial conditions at the workplace. The contribution of these results to manage work-related musculoskeletal disorders is a promising proposition.
Conflict of interest
The authors have no conflict of interest to report.
Footnotes
Acknowledgments
The research reported in the current paper was supported by a research grant (ref: 567) from Research Center for Social Determinants of Health at Semnan University of Medical Sciences. The author would like to extend thanks to all nurses who contributed in the surveys and Semnan academic hospitals for their permission and cooperation in carrying out the research.