
Abstract
BACKGROUND:
Maintaining adequate working ability of construction workers is of considerable importance for society, as the construction sector is burdened with high prevalence of work-related diseases and health-issues.
OBJECTIVE:
To determine the number and age of construction workers in Croatia with temporary or permanent work limitation status, as well as to identify the most common health causes of such work limitation.
METHODS:
A retrospective cross-sectional study was performed using the data from 2534 construction workers, aged between 18 and 65 years, who underwent standardized routine occupational health examinations between 2011 and 2015. Thorough medical history and medical record reviews, blood and urine analyses, vision parameters and hearing range evaluation, as well as mental health assessment were conducted on every study participant.
RESULTS:
A total of 210 construction workers (8.29%) received occupational/work limitation status (either temporary or permanent). Four main categories of work limitation were high blood pressure, disorders of the liver and digestive system, hearing loss and amblyopia, comprising 61.69% of all diagnoses. A total of 37.62% of workers with work limitation status had two or more different diagnoses (i.e. co-morbid conditions). Those with work limitation (either temporary or long-term) were significantly older than those fit enough to work (p-value <0.00001).
CONCLUSIONS:
This type of organized screening represents a significant preventative effort in the construction industry, as workers may become more cognizant of the conditions that may affect their work ability.
Introduction
Working conditions in the construction industry have improved considerably over the last several decades; nevertheless, heavy physical work, lifting and handling heavy loads, static works, unfavorable climatic conditions, noise and other factors may adversely affect workers’ health [1–3]. Furthermore, the construction industry around the world is characterized by a significant number of fatal and nonfatal injuries, and even higher prevalence of work-related diseases [4–6].
Therefore, maintaining adequate working ability of construction workers is of great importance for the society, mainly by reducing the number of days spent on sick leave, lessening the burden of early retirement and attaining a better quality of life for the workers [7]. Occupational medicine – a branch of medicine that emphasizes prevention and aims to maintain and improve the health of workers (as well as their long-term work capabilities) – has a specific role in assessing potential work limitation in individuals working in the construction industry [8].
In Croatia, the construction sector accounts for a substantial part of the economy, and the latest data from June 2015 show that construction industry employs 90,464 workers (which accounts for 6.7% of the total number of employed individuals) [9]. Legislation in Croatia consists of two pivotal documents, both issued in 1984: “Ordinance on jobs in special work conditions” which describes the jobs with special working conditions and prerequisites that must be met by workers performing these tasks [10], and “Ordinance on determining general and specific health ability of workers and skills for special working conditions”, which provides the content and procedures of conducting medical examinations of workers with specific tasks [11].
Construction workers are inevitably a subject to these regulations, as description of their duties encompasses specific work conditions such as the management and handling of mechanized machines and equipment, management of self-propelled mechanized systems, management of mechanically powered cranes, jobs to raise scaffolding, formwork and to set up fences, work that require hard physical strain, jobs performed at height, work in unfavorable microclimate conditions and work in noise [10–12].
There is some evidence that construction workers are faced with a higher risk of occupational disability when compared to workers in less physically demanding jobs [13, 14]. Also, the proportion of older workers in the construction industry will probably increase as a result of the demographic change and the proclivity among young individuals to choose jobs that are less physically demanding [15]. Hence, the role of occupational medicine specialists is to determine general working ability, but also to appraise in which cases specific work tasks cannot be entrusted to workers without adequate physical traits or with certain health deficits that are not disqualifying for the job itself, but only for certain segments of it [12]. Accordingly, age should also be taken into consideration.
Thus, the aim of our research was to determine the number and age of construction workers who fulfill criteria for temporary or permanent work limitation status in the construction industry during a five-year period, and also to identify the most common health causes of such work limitation, with a public health end-goal of protecting the workers’ health and maintaining their long-term work ability.
Material and methods
This observational, cross-sectional study was performed using the data from 2534 construction workers based in Croatia, aged between 18 and 65 years, who underwent standardized routine occupational health examinations between 2011 and 2015 at the Occupational Health and Sports Medicine Unit of the Health Care Institution “Profozić” in the city of Zagreb. Their previous health history that consisted of comprehensive medical documentation provided by their general practitioner also formed a part of our methodological approach.
Occupational health examination were based on the legislation on health and safety at work [10, 11], while the study population included construction workers with specific work conditions such as the management and handling of mechanized machines and equipment, management of self-propelled mechanized systems, management of mechanically powered cranes, jobs to raise scaffolding, formwork and to set up fences, work that require hard physical strain, jobs performed at height, work in unfavorable microclimatic conditions and work in noise – as delineated in legislation specific for the Republic of Croatia [10–12].
From a total of 2534 construction workers that were a part of this study, 523 of them were unskilled manual laborers, 211 were bricklayers, 39 were engineers (machinists), 330 were crane workers, 132 were bar benders and fixers (concrete workers), 262 were welders, 909 were carpenters, 21 were scaffolders, 46 were painters and/or decorators, and 61 were electrical laborers. The average length of their working history was 23.14 years (and ranged from 1 to 42 years).
The occupational medicine specialist conducted a detailed assessment of each study participant which comprised of a thorough medical history taking, notation of all previous medical diagnoses and the meticulous insights into all antecedent official medical records. In addition, the occupational medicine specialist conducted a detailed physical examination according to the guidelines and aforementioned legislation, with a special emphasis on blood pressure and cardiovascular system, vertebral and musculoskeletal system, pulmonary system, gastrointestinal system, and nervous system.
Blood was taken from each participant for the analysis of essential parameters such as complete blood count, erythrocyte sedimentation rate, glucose levels and diagnostic markers for liver and digestive tract disorders (aspartate aminotransferase, alanine aminotransferase and gamma-glutamyl transpeptidase), while at the same time urine sample was taken for biochemical and microscopic examination (including glucose and protein level measurement).
Visual acuity, color-blindness tests, deep vision and night vision were determined by using Vistec Rodatest 3902 device, and in case of any abnormal findings, ophthalmology specialist was consulted to conduct a more precise pathology determination. Hearing range was interrogated by using Interacoustics AD226 Diagnostic Audiometer, and cases with abnormal findings underwent additional examination by otorhinolaryngology specialist for hearing loss and other hearing pathology. Mental health assessment was conducted by a trained psychologist, and patients with abnormal results were thoroughly examined by a consultant psychiatrist.
In accordance with the official criteria abided by all occupational medicine specialists in Croatia, temporary work limitation status was given when examinees were not capable of performing specific work tasks for a certain period of time, which was determined by the duration of the illness or rehabilitation due to specific injuries [12]; this category is considered only temporary, with the main goal that workers during that period undergo a detailed medical examination and any necessary treatments that will prevent potential work disabilities. On the other hand, permanent work limitation status was given in instances when certain chronic illnesses or injuries were considered disabling for safe performing of specific work tasks, despite any medical treatments or rehabilitation endeavors that were pursued [12].
All the diagnoses that resulted in temporary or permanent work limitation were grouped into nine “umbrella” categories: high blood pressure, disorders of the liver and digestive system, hearing loss and other auditory impairments, amblyopia and other vision impairments, diabetes and glucose intolerance, diseases of the vertebral column and musculoskeletal system, psychiatric diseases, diseases of the cardiovascular system, and other diseases. Descriptive statistics, Student’s t-test and chi-square test were used to analyze the data.
Results
Among the 2534 construction workers screened between 2011 and 2015, a total of 210 workers (8.29%) received work limitation status (either temporary or permanent). Of the total number of workers with work limitation, 43 of them were unskilled manual laborers, 22 were bricklayers, 3 were engineers (machinists), 27 were crane workers, 8 were bar benders and fixers (concrete workers), 19 were welders, 77 were carpenters, 2 were scaffolders, 4 were painters and/or decorators, and 5 were electrical laborers.
The age range of those fit to work was 18–65 (mean: 39.74, median: 38), while the age range of workers that received work limitation status was 21–64 (mean: 48.08, median: 51). The difference in ages between the two aforementioned groups was statistically significant (p < 0.00001), i.e. those with work limitation status were older on average than those who were deemed capable to work.
A detailed breakdown of diagnoses that resulted in a work limitation status, as well as the differentiation between temporary work limitation and permanent work limitation, are shown in the Fig. 1 and Table 1, respectively (the number is higher than a total number of workers with work limitation status due to two or more diagnoses in 37.62% of workers). Statistically significant age related differences of workers with work limitation (both classifications) and those capable to work have been found for the diagnostic categories of high blood pressure (p < 0.00001), disorders of the liver and digestive system (p = 0.0002), hearing loss and other auditory impairments (p < 0.00001), diabetes and glucose intolerance (p < 0.00001), diseases of the vertebral column and musculoskeletal system (p = 0.0265), as well as for diseases of the cardiovascular system (p = 0.00592).
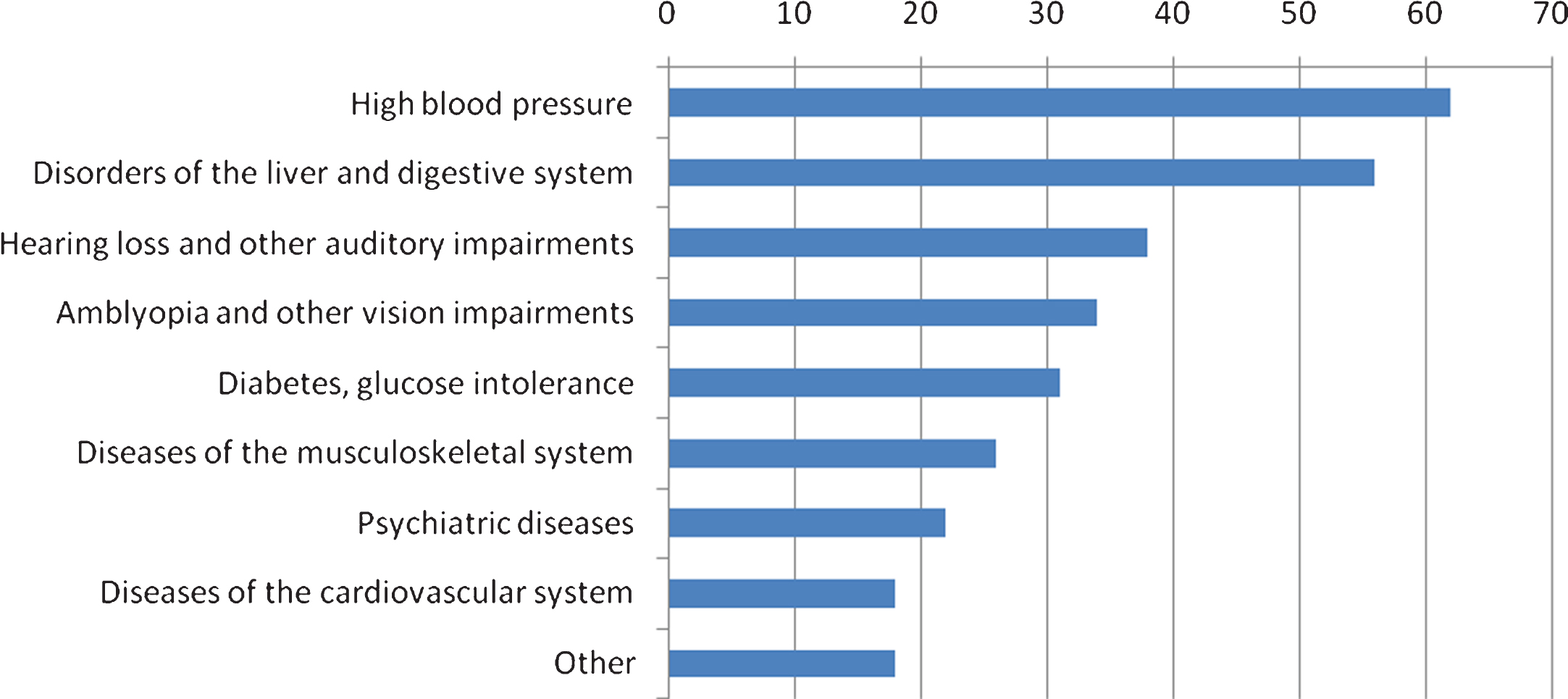
Work limitation according to the diagnostic groups.
Work limitation status according to the underlying diagnoses and age comparison with the total population of “healthy” workers
*The number is higher than a total number of workers with work limitation status due to two or more diagnoses in 37.62% of workers.
Age related differences have not been demonstrated for the diagnostic categories of amblyopia and other vision impairments, psychiatric diseases, and a plethora of other smaller categories such as the diseases of the nervous system and respiratory system, as well as post-malignant disease state. Likewise, mutual comparison of workers assigned temporary work limitation or permanent work limitation (in diagnostic categories that contained both) did not show any statistically significant differences regarding the age of workers.
Whilst four of the categories encompassed only construction workers with permanent work limitation status, five categories comprised workers with both temporary and permanent work limitation status. One of them is a high blood pressure group, in which temporary work limitation was given to workers with treatable hypertension, whereas permanent work limitation status was declared when the blood pressure could not be regulated at all, or when there were certain co-morbid issues.
Similar pattern was observed in other categories. Temporary work limitation was given to those with elevated transaminases in the group of the liver and digestive system disorders, those with blood sugar levels that could be easily regulated in diabetes and glucose intolerance group, as well as those with acute stress disorder in psychiatric group. On the other hand, permanent work limitation was reserved for construction workers with liver fibrosis and cirrhosis in liver dysfunction group, insulin-dependent or recalcitrant diabetes mellitus in diabetes and glucose intolerance group, as well as those with permanent psychiatric issues.
A total of 131 workers (25 unskilled manual laborers, 12 bricklayers, 2 engineers/machinists, 15 crane workers, 5 bar benders and fixers, 13 welders, 52 carpenters, 1 scaffolder, 3 painters and/or decorators, and 5 electrical laborers) had one diagnosis that was sufficient for to assign work limitation status, 60 of them (13 unskilled manual laborers, 7 bricklayers, 1 engineer/machinist, 8 crane workers, 2 bar benders and fixers, 5 welders, 21 carpenters, 1 painter and/or decorator, and 2 electrical laborers) had two diagnoses, whereas 19 of them (5 unskilled manual laborers, 3 bricklayers, 4 crane workers, 1 bar bender and fixer, 1 welder, 4 carpenters, and 1 scaffolder) had three or more diagnoses (Table 2). Chi-square test did not reveal any significant difference in the number of workers with work limitation from 2011 to 2015 (p = 0.4748) (Table 3, Fig. 2).
A number of different diagnoses per construction worker with work limitation status (Total: 210 workers)
A number of workers with work limitation status from 2011 to 2015
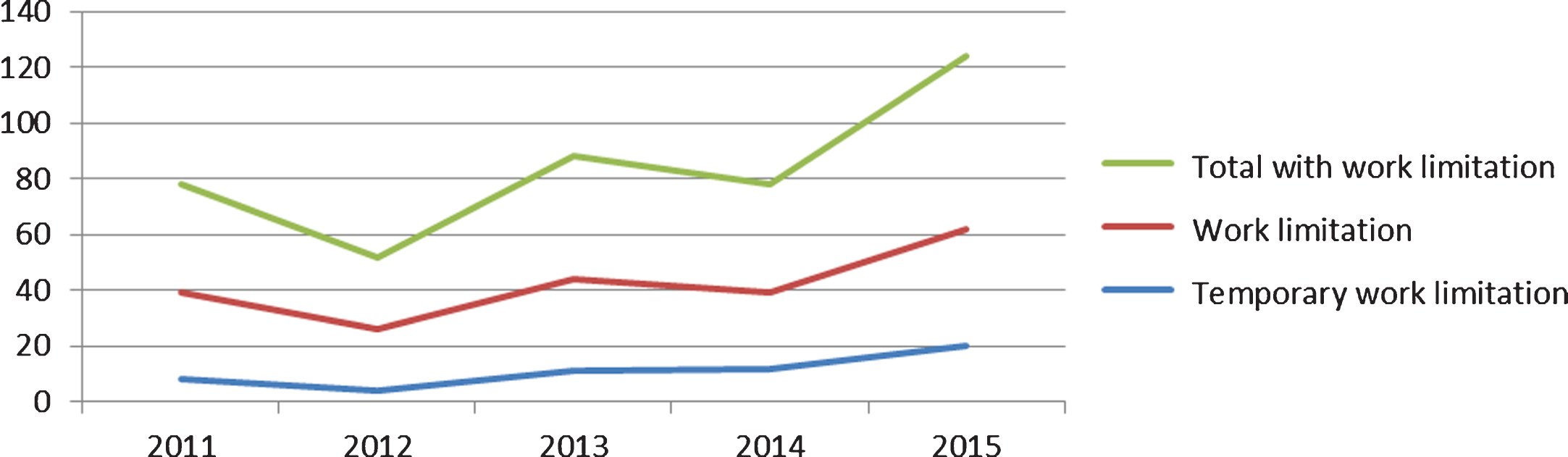
Graphical presentation of a number of workers with work limitation status from 2011 to 2015.
A majority of industrialized countries have instituted specific public health programmes in order to protect the workers who demonstrate some sort of work limitation due to their underlying conditions. Nevertheless, studies addressing this issue in distinct professional groups are scarce; in addition, construction workers are particularly cumbersome to study due to their frequent change of working sites and/or employers, as well as a high number of temporary contracts [16].
This study, to our knowledge, represents the first research endeavor on the work limitation status in construction workers in Croatia. The results of our study point to four main reasons of occupational/work limitation among construction workers – high blood pressure, disorders of the liver and digestive system, hearing loss and amblyopia – comprising 61.69% of all diagnoses. Furthermore, we established that 37.62% of workers with work limitation status had two or more different diagnoses, which can be considered a significant burden of co-morbid medical conditions in this professional group.
In our study, those with work limitation (either temporary or permanent) were significantly older than those without any work limitation. The mean age of the latter group was 39.74, whereas the mean age of construction workers that received work limitation status was 48.08, which was found to be a statistically significant difference. This finding is reinforced by other studies as well, where older age was associated with the presence of a medical condition and reduced physical functioning [17, 18].
Dissimilar legislation and various data collection issues in different countries hamper direct comparison with the available literature; nevertheless, some parallels can be drawn. In a German cohort study on 14,474 male construction workers, musculoskeletal disorders were a major cause of work disability (45%), followed by cardiovascular diseases (19%) [15]. Furthermore, the prevalence of musculoskeletal disorders among 267 bricklayers and 232 supervisors in the Netherlands was 67% and 57%, respectively [19]. American authors have established that musculoskeletal conditions in construction roofers are strongly associated with work limitation, work absenteeism and reduced physical functioning – factors that are predictive of premature departure from the workforce [20].
Moreover, Finnish researchers have demonstrated that musculoskeletal disorders can be responsible for more than a third of all sick leaves that last over nine days in the construction sector [21]. In their study, the proportion of construction workers suffering from repetitive or chronic neck and shoulder, shoulder or arm, or low-back disorders was 55.6%, 44.8% and 42.1%, respectively [21]. Also, a long-term follow-up of Swedish construction workers has shown that musculoskeletal disorders were the most common cause of working years lost due to disability pensions [22].
This is in contrast to our study where diseases of the vertebral column and musculoskeletal system were only the 6th cause of work limitation, comprising 8.44% of all diagnoses. Still, one must consider methodological differences between our study and aforementioned studies. For example, we concentrated on observable predictors of work limitation, as well as on previous medical documentation, while other researchers often relied on questionnaires and self-reported symptoms to assess occupational limitation or disability [19–21].
Hypertension or high blood pressure was the most common cause of work limitation in our study (i.e. 29.52% of workers with work limitation), while other diseases of cardiovascular system (such as cardiomyopathies, atrial fibrillation, suspected Wolff–Parkinson–White syndrome, varices and rheumatic fever) also contributed with 8.57% (Fig. 1). If we considered all the workers in this study (and not just the ones with work limitation status), the prevalence of hypertension and cardiovascular disease was 3.16%.
This can be compared to the data from the United States (collected by the Centers for Disease Control and Prevention) and Hong Kong (collected by the University of Hong Kong), where 30% and 22.6% of construction workers have been diagnosed with hypertension, respectively [23, 24]. On the other hand, research from the United States shows quite higher general prevalence of heart disease in construction workers than our study, reaching 5.5% in 2010 [23]. Moreover, while in the United States 8% of construction workers have been diagnosed with diabetes [25], and there were 4.3% of them in Hong Kong [24], there were only 1.22% of diabetic workers in our study. All of this means that construction workers from different countries may have a different disease burden, albeit aforementioned methodological differences should be taken into account.
Disorders of the liver and digestive system, a diagnostic category that encompassed 18.18% of all diagnoses in our paper, was assessed indirectly via gamma-glutamyltransferase (gamma-GT) enzyme and other transaminases. As there is accumulating evidence that gamma-GT is not merely a sensitive marker for liver disorders, but also a risk marker for a panoply of other chronic diseases, it can be considered a significant risk indicator for work disability and work limitation [26]. Based on their research, Arndt et al. concluded that elevated gamma-GT (often in conjunction with aspartate aminotransferase) is a common finding among construction workers, thus it may represent a powerful tool for the identification of individuals at increased risk of early retirement and preterm mortality [27].
High alcohol consumption is one important cause of increased gamma-GT [28], but other factor such as the exposure to various chemicals in the construction industry (most notably paints, organic solvents, varnishes and adhesives) should be taken into account [29]. Furthermore, an infection with the bacterial pathogen Helicobacter pylori can also have a role in diseases of the liver and gastrointestinal tract, and induce increased levels of this enzyme [30, 31]. In that regard, gamma-GT assessment can be considered helpful in adequate targeting of prevention efforts.
Overall, the medical literature indicates that hearing loss represent a frequent diagnosis in the construction industry, albeit surprisingly only a handful of high-quality studies are published [32]. Lie et al. demonstrated that occupational noise exposure was responsible for 7 to 21% of the hearing loss among industry workers and other similar professions [32]. In our study, hearing loss and other auditory impairments were found in 18.10% of all construction workers with work limitation status, while the prevalence in all workers was 1.5%.
Patients with amblyopia are deterred from a wide range of jobs, which inevitably increases with the severity of the amblyopia [33]. Amblyopia, therefore, acts as a handicap when seeking employment, especially in the construction sector. As the best described long-term consequence of amplyopia is an increased risk of bilateral blindness caused by traumatic eye injury [34], it is not surprising that such vision issues are relevant for considering permanent work limitation. Thus far no studies have addressed the prevalence of amblyopia in a cohort of construction workers, which in our study dominates as a principal vision pathology (12.34% of all diagnoses) that results in work limitation status.
The advantages of our study are a large sample size, a five-year study period, as well as a possibility to assess co-morbidities and multiple diagnoses. One of the main limitations of our study is that our statistical analysis was restricted to only one sociodemographic factor (age), while the impact of other factors (most notably lifestyle habits or unrecognized work-related health/safety issues) have not been taken into account. Therefore, a larger study that employs multivariate analysis should also be conducted in the future. Also, construction workers were predominantly from one region (the capital city Zagreb and its surroundings). We are also concerned about those construction workers who quitted the industry due to a health reason, but before this baseline examination took place (resulting in a “healthy worker survivor effect”) [35].
Recently, it has been shown that the participation of construction workers in a periodic medical screening program can be linked to a favorable impact on a plethora of health outcomes [36]. Also, it has been shown that construction workers can be encouraged and engaged to share ideas in order to improve their health at work [37]. Still, everything stems from the multidisciplinary approach of general practitioners and occupational medicine specialists (but also internal medicine and physical medicine specialists) who should be cognizant of the most common causes of work limitation in order to prompt and achieve desired positive changes.
Conclusion
Our study has shown that the prevalence of cardiovascular risk factors (hypertension in particular), but also risk factors for liver/digestive system, vision and hearing damage can be considered significant in the population of construction workers. As workers are generally unaware of their presence, this type of organized screening represents a pivotal approach to prevention and promoting healthful behaviors that are much needed in the construction sector.
Conflict of interest
None declared.