
Abstract
BACKGROUND:
Stigma and disclosure are important work-related issues for people living with HIV (PLWH). To gain better understanding and improve the position of PLWH in the labor market, further insight in these issues is needed.
OBJECTIVE:
This study reviews the scientific evidence related to work-related stigma and disclosure.
METHODS:
A sensitive literature search was performed in the databases of Medline, Embase, Cochrane Library, Cinahl and Psychinfo for articles published between 1996 and 2016. All studies on PLWH in western countries and investigating disclosure or stigma in relation to work were included.
RESULTS:
Of the 866 identified studies, 19 met the inclusion criteria: 4 addressed both disclosure and stigma (2 quantitative), 9 addressed only disclosure (4 quantitative) and 7 studies addressed only stigma (4 quantitative).
CONCLUSION:
This review provides a unique overview of the research on work-related disclosure and stigma, which will enable health care providers to support PWLH to make well-considered decisions. However, the available literature was heterogeneous and in most studies the topics of our interest were secondary outcomes and provided only basic insight.
Introduction
Living with HIV as a chronic disease is associated with psychological and social problems, such as HIV-related stigma. Stigma is a discrediting social label that changes the way persons view themselves and the way they are viewed by others [1]. Stigma can lead to social exclusion and depression among people living with HIV (PLWH) [2]. Moreover, a higher prevalence of depression and anxiety is reported among PLWH compared with both the general population and with persons experiencing other chronic diseases [3, 4]. Among the population of PLWH, over half experience some type of stigma [4]. Due to the fear of stigma, disclosure has become an important issue to be taken into account. Unfortunately, fear of stigma and social exclusion are important reasons for nondisclosure [5].
Disclosure of HIV diagnosis is a complex issue in daily living, with a considerable impact on the quality of life of PLWH [6]. The advantages of disclosure include safer sex, better (mental) health, more social support, and increased adherence to antiretroviral therapy [7–9], whereas the negative aspects of disclosure can include rejection, loneliness, stigma and discrimination [10].
The dilemma of disclosure and stigma plays an important role in various social interactions, including sexual relations, family, health care, and work. Because the vast majority of PLWH is of working age, it is important to investigate work-related disclosure and stigma. Of nurses working with HIV patients, 98% reported that the dilemma of disclosure was an important work-related issue of PLWH in their clinics [11]. People who experienced HIV-related discrimination had an increased risk of employment loss [12]. Also, in the workplace, PLWH may be confronted with gossip, contempt, and social isolation from co-workers and/or employers [13].
Participation in the labor force is a key concern for many PLWH [14, 15]. However, PLWH still have a lower employment rate than the general population in several European countries [16, 17], and face various problems at work or when returning to work [18]. With the aim to improve vocational counseling, a multidisciplinary, evidence-based guideline on HIV and work was developed in 2012 in the Netherlands [19]. This guideline provided recommendations for PLWH and for healthcare providers about how work-related care can be improved. Qualitative research conducted in the context of the guideline development, showed that disclosure and stigma were major work-related concerns of PLWH in the Netherlands [15]. However, little scientific evidence/related data were available.
Therefore, stigma and disclosure as barriers for sustainable work participation among PLWH needs additional study to elucidate the daily issues experienced by these individuals in western countries and to improve counseling methods. Therefore, this review focuses on the scientific evidence for stigma and disclosure at the place of work.
Methods
A scoping review of the literature was conducted to summarize the findings on stigma and/or disclosure in relation to work. This study was guided by the Arksey and O’Malley framework for scoping studies [20].
Identification of studies
Types of studies
Included were qualitative and quantitative studies reporting original data on stigma and/or disclosure related to work among adults with HIV, conducted in a western country. Excluded were case reports, conference proceedings, books, dissertations, and letters to the editor. There were no restrictions on the language of publication.
Search methods
A literature search was performed in February 2016 in the databases Medline, Embase, Cochrane Library, Cinahl and Psychinfo using a combination of the following keywords (and their synonyms): employment, HIV, stigma, and disclosure. The complete search strategy can be found in Appendix 1. The search was limited to articles published after 1996 because of the introduction of HAART (Highly Active Antiretroviral Therapy) after that date.
Selection of studies
After conducting the search, two authors (MW and SvO) independently screened all search results. First, relevant articles were selected by screening titles and abstracts. Subsequently, we retrieved full-texts of all included articles and the two authors screened these remaining articles for eligibility. Any dissensus about eligibility was resolved through discussion, or through recourse to an independent author (PR).
Data extraction
Data were extracted directly from the full-text articles by the first author (MW). A pre-structured form was used covering the research design, the main topic of the study (stigma and/or disclosure), sample description, and key findings of each study.
Collating, summarizing, and reporting results
Data were classified by the two main themes, i.e. disclosure and stigma. Data on disclosure were divided into subsections (the reported levels of disclosure, background characteristics, reasons for (non) disclosure and consequences of disclosure) in order to integrate the available evidence for each topic. Data on stigma were divided into the following subsections: level of perceived stigma, reported reasons for stigma, background characteristics related to stigma, fear of stigma, and consequences of stigma.
Results
Selection of studies
Figure 1 presents the flow-chart of the selection process. Of the 866 citations retrieved from the search, most were excluded because they did not address work-related problems. A total of 19 studies met the inclusion criteria: 4 addressed both disclosure and stigma (2 quantitative), 9 addressed only disclosure (4 quantitative) and 7 studies addressed only stigma (4 quantitative). In 30% of the eligible studies, disclosure and/or stigma was not the main focus of the study.
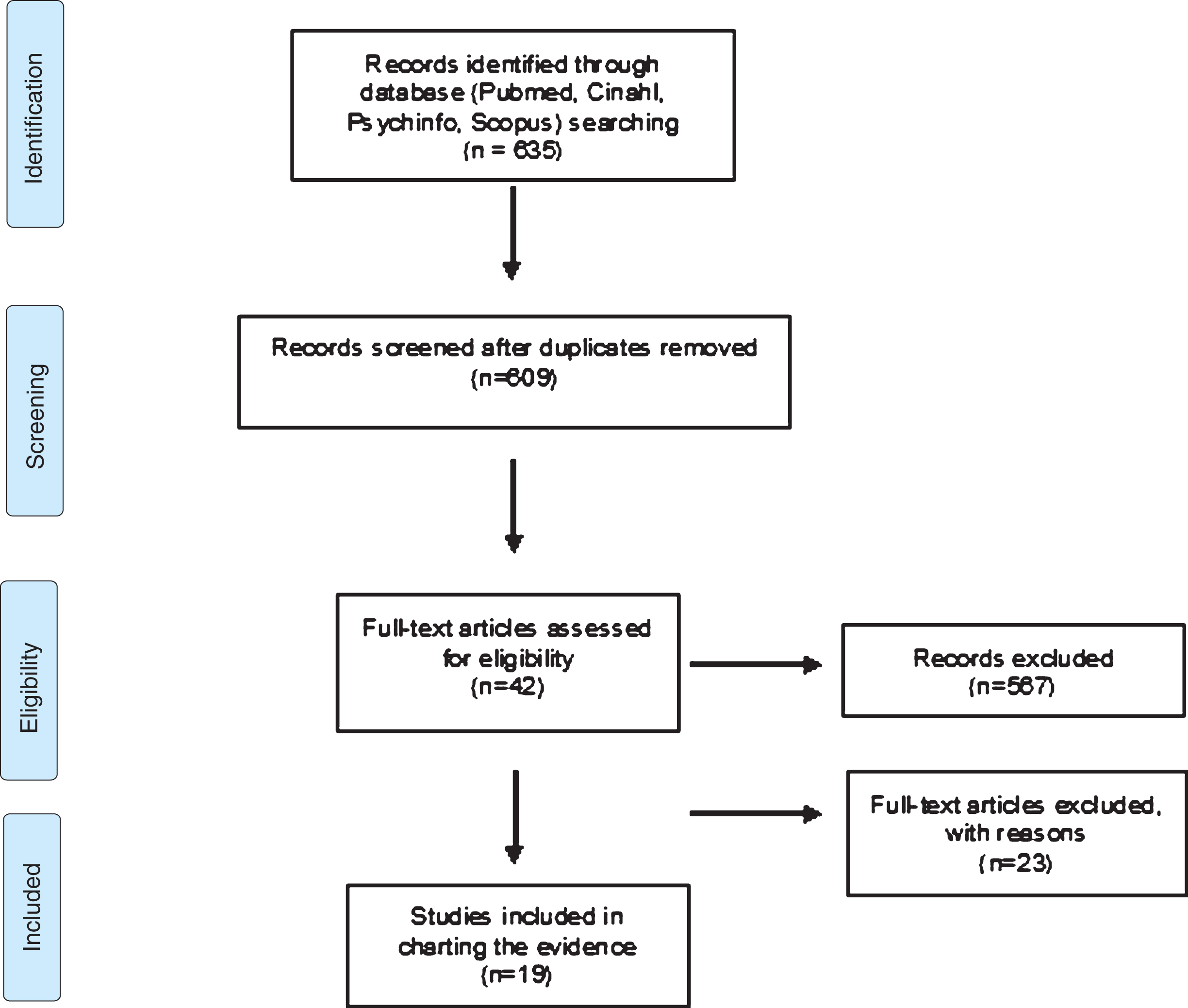
Selection of the eligible studies.
Table 1 summarizes the main findings of the studies on disclosure, which are briefly described below.
Main findings of the studies on disclosure
Main findings of the studies on disclosure
The level of disclosure to employers/colleagues was reported in six studies and ranged from 22–50% [21–26]. In two studies a comparison was made between employers and colleagues [21]; the conclusion was that the level of disclosure to the employer is lower than that to colleagues (22–27% vs. 30–33%). One study showed that most participants only partly disclosed to a few people at their work [15].
Background characteristics associated with disclosure
In 6 studies background characteristics were reported as factors associated with disclosure, i.e. age, gender, ethnicity, disease-related factors, and characteristics of the workplace [21–26]; these are described below.
3.2.2.1 Age. One study reported the role of age in relation to disclosure and concluded that disclosure was not associated with age (p > 0.05) [22].
3.2.2.2 Gender. The role of gender was reported in two studies. One study found no difference [22], whereas the other concluded that women were less likely than men to disclose their HIV-positive status at the workplace [24].
3.2.2.3 Ethnicity. Three studies investigated ethnicity [23, 27]; all concluded that a black African ethnic background was associated with a lower level of disclosure.
3.2.2.4 Disease-related factors. Three studies reported on the role of time since diagnosis in relation to disclosure [21, 27]; two concluded that disease duration and number of years with HIV were associated with a higher level of disclosure [21, 27]. The odds ratio for disclosure to the employer increased with 43% for each additional year (p < 0.05) [21]. One study reported the influence of the way of transmission, concluding that being exposed to HIV because of heterosexual contact is negatively associated with disclosure [27].
3.2.2.5 Characteristics of the workplace. Two studies reported characteristics of the workplace [21, 22]. Both concluded that a higher position in the organization (e.g. managers) or non-manual work (e.g. professional or administrative) were positively associated with the level of disclosure. Furthermore, the degree to which HIV interfered with one’s ability to work was an important predictor of disclosure [21].
Reasons for disclosure
The reasons for disclosure were divided into four subgroups: personal, work-related, changing health status, and relation with colleagues or employer.
3.2.3.1 Personal reasons. Three articles described different personal reasons for disclosure, such as not wanting to live with a secret and honesty [22], personal acceptance of the HIV status [24], and the need to be accepted without prejudice.
3.2.3.2 Work-related reasons. The need for accommodation and support at work was mentioned in two studies [24, 28]. Furthermore, the need to provide an explanation for choices regarding work, and concerns about workability, were important reasons to disclose HIV status at work.
3.2.3.3 Changing health status Three studies reported that disclosure is sometimes necessary because of a change in health status, such as progression of the illness which may lead to absences [22, 29].
3.2.3.4 Relation with colleagues and employer. One study examined the level of trust in colleagues and employer and found this to be an important aspect in the decision to disclose [30].
Reasons for non-disclosure
The reasons for non-disclosure can be divided in two groups: need for privacy, and fear of stigma.
3.2.4.1 Need for privacy. Two studies reported that the main reason for concealment of the HIV status at work was the need for privacy [24, 28]. One study concluded that the perceived irrelevance of the HIV status for work was important for the decision not to disclose [15].
3.2.4.2 Fear of stigma. Five studies described that fear of stigma is one of the main reasons for non-disclosure [24, 28–30]. Also limited disclosure (to only one, or a few colleagues) can be an important strategy to avoid stigma [30].
Consequences of disclosure
After the decision to disclose or conceal their HIV status PLWH faced different consequences, varying from more accommodations at the workplace [26] to social isolation [24] or gossiping [15].
Stigma
Table 2 summarizes the main findings of the studies on stigma; these are briefly discussed below.
Main findings of the studies on stigma
Main findings of the studies on stigma
Three studies reported the level of perceived stigma at work; this ranged from 6–11% [25, 31]. One study reported that over two-thirds of PLWH reported that they were not allowed to go to a medical appointment during working hours without losing payment, which might be considered as stigma [26]. Another study reported that 24% of their participants indicated facing discrimination when applying for a job [31]. One study made an analysis of the complaints submitted to the Equal Employment Opportunity Commission about discrimination at work because of a chronic disease (including HIV): of all complaints filed by people with disabilities under the employment provisions of the Americans with Disabilities Act in the period 1992–2003, 7.3% concerned discrimination of PLWH. The most important reasons for complaints were resignation, a change of contract, harassment, or not being offered work accommodations [32]. In a Swiss study, no discrimination was found in legal texts or regulations. In contrast, stigmatization and practices of individual discrimination seems to be present based on interviews with informants.
Reported reasons for stigma
Several reasons for stigma and discrimination emerged, including fear of contamination, lack of awareness, homophobia [30], and the general perception that it is a person’s own fault that they are HIV positive [24]. In two other studies all employers indicated having difficulties when hiring PLWH, because of their concerns about possible biological and/or social contagion [34, 35].
Background characteristics related to stigma
Older people, men who have sex with men, drug users, and migrant women experienced significantly more discrimination [31]. A comparative study of PLWH in different geographical regions concluded that work-related stigma and discrimination appeared more often and was more severe in the Caribbean area than in the UK [30].
Fear of stigma
In four studies fear of stigma was described, but without a relation to (non) disclosure. Three studies noted that, for people currently not working, fear of being stigmatized by colleagues was a major barrier to obtaining employment [25, 36]. The other study described the perception of many participants, that employers are not HIV sensitive and that the Americans with Disabilities Act would not protect them from discrimination [37]. In another study, 98% of HIV nurses reported that fear of stigma was one of the main work-related issues of PLWH in their clinics [19].
Consequences of stigma
Possible consequences of stigma can include: the undermining of care and treatment (e.g. delaying medical appointments), limited opportunities for integration into society, and economic independence [30]. Furthermore, a consequence of stigma might be that PLWH refrain from certain types of jobs (not specified) [37].
Discussion
Discussion
Due to improved life expectancy, work participation, and working conditions, disclosure of HIV status and stigma have become important issues in the daily lives of PLWH. This study is the first scoping review to examine the work-related issues disclosure and stigma.
This study shows that the level of disclosure at work is low, ranging from 22–50%. The main reason for non-disclosure is the fear of stigma. However, the level of reported stigma is low (6–11%). Since the HIV virus can be successfully suppressed by medication, the need to disclose this status has become less urgent and does not need to influence the ability to work. Reasons for disclosure include mainly personal reasons, such as the desire to be honest or to be accepted, or reasons related to the extent to which HIV influences the ability to work.
Compared to work-related disclosure in other chronic diseases the level of disclosure at work of PLWH is average. For example, people with diabetes are more likely to disclose their health status at work, i.e. 84%, compared with about 50% among breast cancer survivors, and only 37% disclosure among people with a mental illness [38, 39]. The level of disclosure of PLWH among other persons (such as spouses and friends) was higher, ranging from 60–96% [8]. The increased level of knowledge among the general population is one of the reasons why, at least in these settings, discussing seropositivity is easier compared to a decade ago [6]. Although not yet investigated, increasing knowledge on HIV in the context of work might also encourage disclosure.
Determinants of disclosure at work which were only slightly touched upon by the studies in the present review, are ethnicity and sexual preference. However, it is important to take into account that, in other settings, immigrant PLWH are probably less likely to disclose their HIV status due to the perception of HIV/AIDS in their country of origin, and the fear of rejection [40]. This also applies to men who have sex with men, who may suffer from homonegativity, i.e. the stigma associated with homosexuality [41]. PLWH often experience multiple stigmatized identities which influence their decisions about disclosing their HIV status in various settings, including work. In the counseling of PLWH it is important to take these multiple stigmatized identities into account.
Stigma, as a social construct, is not rigid but varies between different cultures, groups and organizations. Stigma can be divided into subtypes, such as enacted stigma, perceived stigma, and internalized stigma [42]. Although the studies included in this review describe enacted, perceived and internalized stigma, the interactions between these forms of stigma remain unclear, as does the distinction between groups and organizations. It can be assumed that there is a difference in the understanding of the construct of stigma across studies.
The included studies did not clarify the relation between (fear of) stigma and subgroups of PLWH based on health status or psychological consequences. The prevalence of anxiety and depression among PLWH is higher than that of the general population [4]. HIV-related stigma can have a negative impact on health aspects and the wellbeing of PLWH [43]. It is recommended to further examine the role of stigma on health and wellbeing at work in order to provide appropriate counseling.
This review found no evidence for the constructs which play a role in the disclosure process in relation to work. The Disclosure Processes Model describes different constructs that play a role in the disclosure process, such as antecedent goals (approach or avoidance), the disclosure event itself, mediating processes (i.e. inhibition or alleviation), and outcomes such as social and physical wellbeing [44]. Further insight into the complexity of disclosure in relation to work will help PLWH to develop strategies to cope with this complex issue.
The available literature was heterogeneous and in most studies the topics of our interest were secondary outcomes and provided only basic insights. A limitation of this scoping review is the restriction to western countries. Studies from other geographical regions might have added information which might be relevant for western countries. Despite these limitations, the data synthesized in this study provide a broader understanding of work-related stigma and disclosure.
Conclusion
This review provides a unique overview of the available research on work-related disclosure and stigma, which is indispensable for understanding and improving the position of PLWH in the labor market. This study also shows that further investigation of the underlying mechanisms of work-related stigma and disclosure is needed because research in this field is still in its early stages.
Practice implications
Disclosure and stigma are some of the main work-related issues for PLWH. In the counseling of PLWH it is important that healthcare providers are aware of the dilemma about disclosure at work and that they support PLWH to make a well-considered decision. In this context it should be considered that, although HIV is a chronic disease, its social acceptance is not yet comparable to other chronic diseases because it is predominantly sexually transmitted. Healthcare providers should take into account the possible differences between various subgroups, such as immigrants or homosexual PLWH, who may experience multiple stigmatized identities.
Conflict of interest
The manuscript has been seen and approved by all authors and all authors declare no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Appendix 1 Search strategy
(“Acquired Immunodeficiency Syndrome”[Mesh] OR “HIV”[Mesh] OR “HIV Infections”[Mesh] OR acquired immune deficiency syndrome*[tiab] OR aids[tiab] OR htlv-iii[tiab] OR human immunodeficiency virus*[tiab] OR human t cell lymphotropic virus type iii[tiab] OR lav-htlv-iii[tiab] OR lymphadenopathy-associated virus*[tiab] OR hiv infection*[tiab] OR htlv-iii-lav infection*[tiab] OR hiv seropositiv*[tiab] OR anti-hiv positiv*[tiab] OR seropositiv*[tiab] OR hiv-seroconvers*[tiab] OR aids seroconvers*[tiab] OR hiv antibody positiv*[tiab]) AND (“Employment”[Mesh] OR “Job Application”[Mesh] OR “Rehabilitation, Vocational”[Mesh] OR “Unemployment”[Mesh] OR “Vocational Guidance”[Mesh] OR “Sick Leave”[Mesh] OR “Absenteeism”[Mesh] OR employment[tiab] OR underemployment[tiab] OR occupational status*[tiab]) AND (prejudice*[tiab] OR stigma*[tiab] OR social discrimination[tiab] OR sexism[tiab] OR segregation[tiab] OR disclosure[tiab] OR “Prejudice”[Mesh] OR “Truth Disclosure”[Mesh])
AND
(“1996/01/01”[edat]: “2016/02/28”[edat]) OR (“1996/01/01”[mhda]: “2016/02/28”[mhda])
Acknowledgments
The authors thank Mrs. Winnie Schats, head of the Slotervaart Hospital Library, for her help with the literature search.