
Abstract
BACKGROUND:
A great number of antineoplastic drugs (ANPDs) are used globally in cancer treatment. Due to their adverse health effects, occupational exposure to ANPDs is considered a potential health risk to health care workers.
OBJECTIVE:
The current study aimed to evaluate safe-handling practices of ANPDs, exposure controls, and adverse health implications for health care providers exposed to ANDPs.
METHODS:
Prevention measures, including engineering, administrative, and work practice controls, as well as personal protective equipment (PPE), were recorded daily through a questionnaire for six weeks. Acute adverse health effects experienced by health care workers were also documented.
RESULTS:
The implemented exposure controls for preparation, administration, cleaning, and waste disposal were not in accordance with the safe handling guidelines. Central nervous system disorders (26.33%) were the most frequent acute adverse effects reported by health care workers. A significant correlation was found between the number of experienced adverse effects and handling characteristics, including the number of preparations (r = 0.38, p < 0.05), dose, and the number of prepared drugs (r = 0.46, p < 0.01 and 0.39, p < 0.05), and working hours in different locations of oncology setting for six weeks (preparation room: r = 0.38, P < 0.05, treatment room: r = 0.46, P < 0.01, patient room: r = 0.63, P < 0.01, and station: r = 0.68, P < 0.01).
CONCLUSIONS:
Due to inadequate control measures, oncology health care workers were in danger of exposure to ANPDs and experienced acute adverse health effects. Implementation of appropriate exposure controls is required to prevent occupational exposure to ANPDs.
Introduction
The widespread use of ANPDs in the treatment of cancer has led to an increased number of health care workers occupationally exposed to these cytotoxic agents [1, 2]. Health care workers who handle, prepare, and/or administer ANPDs as part of their daily work activities are subject to many health hazards [3–6].
Exposure to ANPDs has been proven to have serious health implications. Common acute adverse health effects include sore throat, chronic cough, dizziness, headaches, allergic reaction, hair loss, nausea, vomiting, and skin rash. In addition, several reproductive toxicities and carcinogenic potential, including miscarriage, congenital malformations, infertility, leukaemia, and other cancers have been documented as long-term effects [1, 9–15]. Nonetheless, there are no safe occupational exposure threshold limits for exposure to ANPDs as hazardous drugs [11, 16].
To help protect health care personnel, safe handling guidelines from professional associations such as Occupational Safety and Health Administration (OSHA) [17], National Institute for Occupational Safety and Health (NIOSH) [18], American Society of Health-System Pharmacists (ASHP), and Oncology Nursing Society (ONS) have been issued [19, 20]. Despite the longstanding availability of safety handling guidelines which highlight the importance of exposure controls, recent studies have shown that environmental contamination and different levels of exposure to ANPDs are still present [1, 21–24].
Evidence of continued risk of occupational exposure to hazardous drugs has shown that safety protocols were not always applied by health care workers [5, 25]. Low adherence to the safe handling practice may be related to some limitations, including workload, understaffed, improper equipment, budget deficit, lack of knowledge, and appropriate training [1, 27].
In Iran, chemotherapeutic medications are prepared in oncology ward and health care workers are involved in ANPDs handling (shipping/receiving, transport and distribution, compounding, administration, and waste disposal). Our oncology setting uses a combination of the hierarchy of control methods to mitigate unintended occupational exposures to ANPDs, including engineering and administrative controls and personal protective equipment (PPE). However, daily reporting of adverse health effects indicating that health care workers are still exposed to ANPDs and assessment of safe-handling practices is necessary [28].
Therefore, the aim of this study was to evaluate the ANDPs’ safe-handling practices and the extent of use of exposure controls by health care workers. Furthermore, we investigated the association between safe handling practices of ANPDs and the related adverse health effects experienced by health care workers.
Methods
A cross-sectional study was conducted between November 2014 and January 2015 in an oncology setting of a tertiary care center. Ethical permission for the study was obtained from the ethics review board of the National Research Institute of Tuberculosis and Lung Diseases. Safe handling practices of ANPDs (preparation, administration, cleaning, and waste disposal) in terms of exposure controls (engineering, administrative, and work practice controls as well as personal protective equipment (PPE) usage) were recorded daily by oncology health care workers through a questionnaire. Moreover, demographic profile and medical history of respondents, dose and number of prepared medications, occupational accidents, and acute adverse health effects (type, appearance time, and duration) experienced by the personnel were documented.
SPSS version 21.0 was used for data analysis. The mean and standard deviations (M±SD) were calculated for quantitative variables. Linear models were used to test the relationships between quantitative data. For qualitative variables, chi-square and fisher test were performed. Statistical significance was considered when P < 0.05.
Results
A total number of 224 questionnaires were filled by 14 oncology health care workers during the study period (7-8 healthcare workers were working in oncology ward every day. They filled the questionnaire for 6 weeks or 30 working days). The mean age of the respondents was 32.80±6.87 years and their median work experience in oncology ward was one year (range 0.08–10). Half the personnel graduated from medical universities. The mean number and dose of prepared medications were 10.62±4.52 and 9.74±4.72 g per day respectively.
Ifosfamide, gemcitabine, cyclophosphamide, carboplatin, fluorouracil, and etopside were the most frequent medications prepared and administered. During the study, a total amount of 389.83 g of chemotherapeutic drugs was prepared. Table 1 shows the frequency of preparations, dose and number of prepared drugs and duration of preparations.
The frequency of preparations, dose and number of prepared drugs, and preparations duration during the study period
The frequency of preparations, dose and number of prepared drugs, and preparations duration during the study period
The frequency of handling practices and PPE usage are shown in Table 2. Gloves and surgical masks were used for 100% of the preparation, cleaning, and waste disposal. From all drug administrations, 20.56% carried out without any PPE. All preparations were done in a biological safety cabinet (BSC) located in a separate room.
The frequency of handling practices and PPE usage
The frequency and time of cleaning (for preparation room and BSC) and waste disposal (for BSC, preparation room, and patient room) are mentioned in Table 3. There was not a schedule for disposal of ANPDs waste in oncology setting.
The frequency and time of cleaning, biohazard waste container cleaning, and waste disposal during the study period
*Mentioned activities were not performed everyday within the study period.
Figure 1 shows that central nervous system disorders (26.33%) were the most frequent acute symptoms reported by health care workers. Gastrointestinal (23.86%), vision (20.98%), skin and appendages (20.57%), and respiratory (5.34%) adverse effects were also reported within the study period.
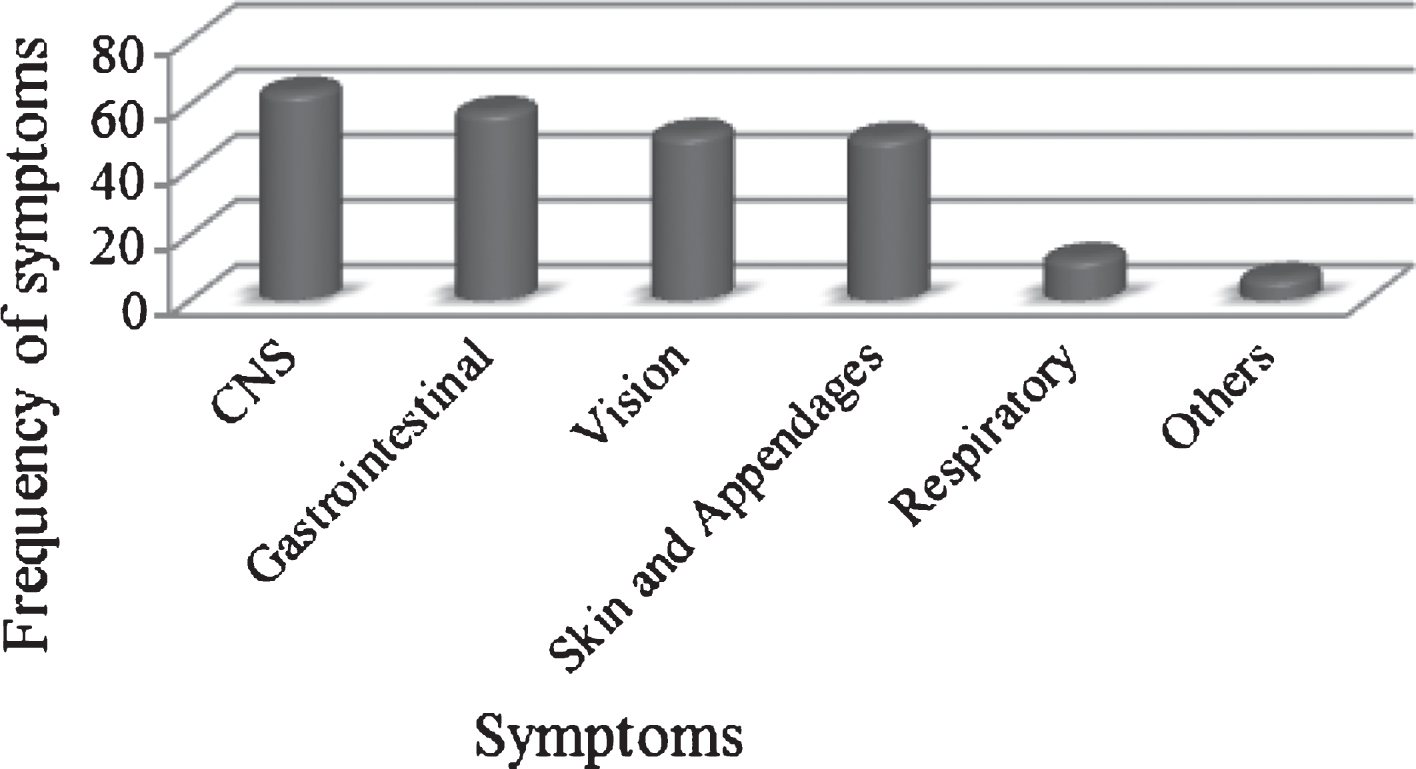
The frequency of reported adverse health effects. CNS: Headache and vertigo; Gastrointestinal: Bitter mouth, sore throat, and nausea; Vision: Eye irritation, eye pain, itchy, and red eye; Skin and appendages: Itchy and dry skin; Respiratory: Runny nose, chest pain, and dyspnea.
There was a significant correlation between frequency of adverse health effects (number of acute adverse health effects reported daily by healthcare workers) and frequency of preparations (r = 0.38, p < 0.05), dose and number of prepared drugs (r = 0.46, p < 0.01 and r = 0.39, p < 0.05). No significant relationship was found between the duration of preparation and the frequency of reported adverse health effects.
ANDPs were often prepared in the first (7.00–9.30 AM) and middle (9.30–12.00 AM) of the work shift, and most symptoms were reported at the middle of the work shift (Fig. 2). Of all reported acute adverse effects, 21.81% disappeared before the end of the work shift while 78.18% extended beyond the work shift.

Frequency of preparation (A), symptom appearance (B), and symptom disappearance (C) in different time of work shift.
Figure 3 depicts the percentage of working hours in different locations of the ward. Working hours in each location (preparation room: r = 0.38, P < 0.05, treatment room: r = 0.46, P < 0.01, patient room: r = 0.63, P < 0.01, and station: r = 0.68, P < 0.01) were significantly correlated with the number of reported adverse health effects.
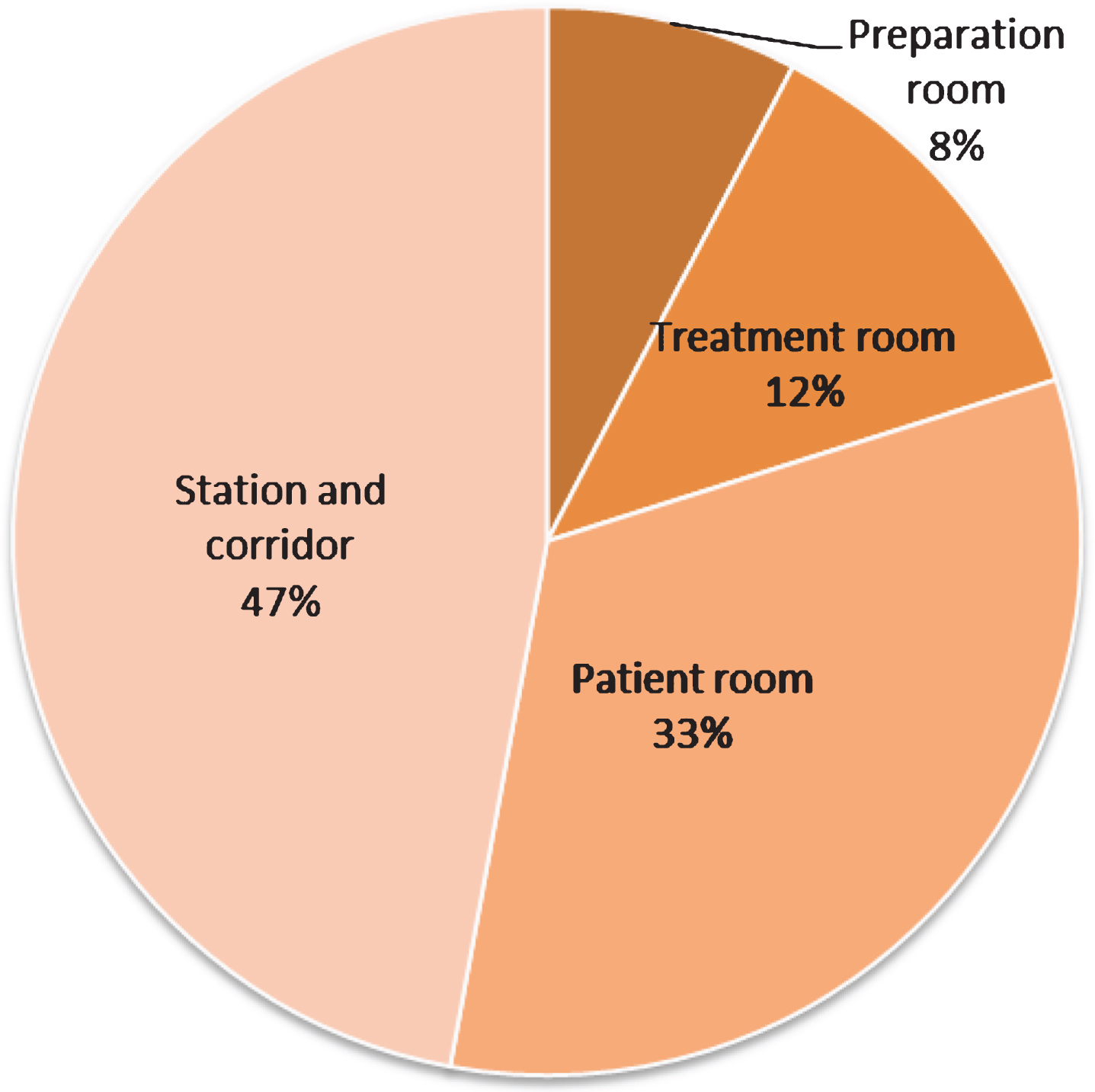
Percentage of working hours in different locations.
A few accidents such as skin contact with patient’s blood, drug, leakage, and spilling of the drug were recorded during the study period. The frequency of accident was once per week. Risky behaviors (smoking, eating, drinking, resting, and storing food) were not reported. Medical history and laboratory tests did not show any chronic diseases among the health care workers (data not shown).
The current study evaluates the safe-handling practices of ANDPs in an oncology setting with respect to use of international safety guidelines [29] as a criterion for occupational exposure to ANPDs. Previous studies from other countries have monitored different environmental and biological factors to assess occupational exposure, including surface contamination [16, 30–32], air contaminations [21, 33], urine drug concentrations [24, 34–37], genetic damage [21, 38–40], and the frequency of adverse effects [22, 41–43]. However, the correlation between work conditions and adverse health effects has less been considered an indicator of occupational exposure.
To date, no comprehensive study has been carried out to evaluate safe handling of ANPDs in Iran. Only a brief report has mentioned the adverse effects experienced by oncology nurses using a descriptive survey [44]. Therefore, we designed the current study to evaluate the safe-handling practices in the oncology setting in order to find out the limitations, improve and reform the practice of handling, and reduce the risk of occupational exposure.
According to previous research and published guidelines, chemotherapy agents (shipping/receiving, transport and distribution, compounding, administration, and waste disposal) need to be handled using exposure controls listed below (that we evaluated) to minimize workplace contamination and prevent occupational exposure [2, 29].
Engineering controls
Since one of the most important ways of exposure to ANPDs is inhalation, preparation should be performed inside a BSC with vertical air flow and HEPA filter (Class 2b or 3) in a separate room [3, 44–46]. The current finding showed that 100% of drug preparations were performed inside of a BSC in a separate room of oncology ward. Nevertheless, adverse health effects were frequently reported by health care workers during and after preparation. This indicates that engineering controls may not completely eliminate contamination [18]. It is in line with a study conducted in Cyprus that reported adverse health effects experienced by nurses who prepared ANDPs in the BSC [22]. Another study also identified that, despite using BSC and a clean room, environmental contamination was widespread [21].
Based on NIOSH recommendation, manipulation of hazardous drugs inside a well-functioning ventilation hood could protect health care workers from occupational exposure; however, periodic monitoring is essential to ensure suitable sash height and air flow [47]. We found that there was no regular monitoring of hood performance and face velocity in our oncology setting.
According to other study, improper location of BSC in the room was another factor for workplace contaminations. Placing BSC between the window and entrance leads to spread ANPDs aerosol to the ward area [41], which could be another reason for occupational exposure and adverse health effects in current study.
Moreover, Closed-system drug transfer device (CSTDs), Lure-lock fittings, and needleless system as other engineering controls [2, 49] were not available in our oncology ward.
Administrative controls
Training (initial and ongoing), which is an important measure to enhance nurses’ knowledge about safe handling of ANDPs, has been highly recommended by OSHA guidelines and several research studies [2, 50–55]. Echoing the results of previous studies [1, 56–58], our results indicated that the health care workers didn’t receive any special pre- or post-training related to safe handling of ANDPs and protection against its harmful effects.
With respect to use of safety guidelines, there were no local guidelines on the safe handling of ANPDs in Iran. Low adherence to international safe handling standards [29] in the current study reconfirms previous research [10, 59].
Medical surveillance for health care provider occupationally exposed to ANPDs is highly suggested by OSHA and NIOSH. However, previous studies indicate that medical monitoring of health care workers is not routinely carried out [2, 59]. In our oncology setting, all health care workers had annual medical monitoring but not specified for workers exposed to ANPDs.
Time pressure, shortage of staff, high work load, large number of drug preparation and administration, and multi-task (multiple responsibilities) were shown to be some of the other reasons for occupational exposures [2, 41].
Work practice controls
Several studies have revealed that, despite control measures, contaminants were detected in the air and surfaces of work area. This is because unreported spills, ANPDs residue on exterior vial surfaces, inappropriate cleaning, and waste disposal contribute to the area contamination [8, 60–65]
The effective use of cleaning methods at preparation stations is important to limit environment contamination [45, 55]. Vandenbroucke et al. proved residual contamination in a cleaned BSC after installing in a new constructed preparation room [66].
Based on our findings, an inappropriate cleaning program in our oncology setting contributed to the work environment contamination. The preparation room was cleaned at the beginning of the work shift and cleaning procedure was not carried out after preparation.
Waste disposal in preparation room and patients’ rooms were not scheduled appropriately and were usually carried out at the start of the work shift. Previous studies indicated that leakage from conventional IV equipment is another source of exposure to ANDPs. Spiking and unspiking IV containers with IV tubing could result in leakage of drugs in administration areas [27, 67]. Another study reported contamination spots of doxorubicin on gloves, clothing, and hands (after glove removal) of health care workers by using fluorescent scanning devices [35].
According to ASHP guideline, drug spill kits should be available in workstations in which chemotherapy drugs are handled and administered [19]. We also found that our health care workers were unaware of hazardous consequences of leakage and spilling, and so they didn’t report them. Constantinidis et al. revealed that health care workers usually do not report accidents and a high number of accidents could be related to the lack of training [41]. Since educated personnel experience fewer accidents, continuous training may reduce the accidents in our hospital.
In contrast to the other studies, risky behaviors were not reported in current study [42, 46].
Personal protective equipment (PPE)
Use of PPE in order to reduce occupational exposure to ANPDs is highly recommended by safe handling guidelines. PPE used for handling hazardous drugs include gowns (disposable, low permeable, closed front, tight cuffs, and single use), gloves (impermeable, powder free, labeled and tested for use with chemotherapy drugs, made of latex, nitrile, or neoprene), face and eye protection (fully enclose the eyes), and a particulate filter P2 (N95) respirator [8, 47].
Our study showed that gloves and surgical masks were regularly used for all activities except administration. Wearing of inadequate PPE for administration activity suggests that there is a wrong perception of low risk of exposure in administration among health care workers [25, 46]. Gown and face protection were not available in the ward and goggles were rarely worn by health care workers. Not wearing PPE and taking contaminated clothes to the home could increase the risk of ANPDs exposure. Inappropriate use of PPE (incomplete and incorrect use) by our personnel reconfirmed the result of other studies [25, 59]. Lack of knowledge has been reported as a barrier to using adequate protection against hazardous drugs [1, 42]. PPE unavailability and budget deficit are also important limitations in developing countries. Surgical mask and gloves worn by our personnel were not adequate for protection against ANPDs.
Acute adverse health effects experienced by the personnel
Acute adverse health effects associated with occupational exposure to ANDPs include skin irritation, sore throat, cough, dizziness, headache, eye irritation, hair loss, allergic reaction, diarrhea, nausea, vomiting, and so on [14, 68].
Our findings showed that the frequency of acute symptoms experienced by health care workers was noticeable. Central nervous system (CNS) symptoms were the most frequently reported acute adverse health effects that were in accordance with the previous studies [22, 44]. In contrast to Constantinidis et al., adverse health effects related to gastrointestinal, skin, and vision systems were reported more than respiratory problems. In addition, their findings showed less gastrointestinal reactions and more respiratory symptoms than our results [41]. Most reactions occurred in the middle of the work shift and lasted to the end or beyond of the shift. In 2003, Krstev et al. also mentioned extension of the symptoms beyond the work shift [69]. Since dermal contact and inhalation are the main causes of exposure to hazardous drugs [14, 67], wearing of suitable protection for skin and respiratory system decrease adverse health effects.
There was significant association between the number of acute symptoms and the numbers of preparations, dose and number of prepared drugs. This is in accordance with Constantinidis et al. study that indicates a correlation between the adverse effects experienced by health care workers and the number of handled drugs and the occurrence of accident [41].
Results of current study proved that working hours in different locations (preparation room, treatment room, patient rooms, and station) of the ward was associated with the number of experienced symptoms reported by health care workers. This finding demonstrates the entire of the ward were contaminated by ANPDs that could be related to improper exposure controls. Another study also showed measurable levels of surface contamination in different workstations of drugs handling [21].
One limitation of our study was restricted number of the respondents that was due to evaluation of safe-handling practices in one oncology setting at a tertiary care center. Although, all oncology health care workers responded the questions every day during the study period and an adequate number of questionnaires were filled for our purposes. Another limitation was the lack of data regarding surface contamination levels and biological monitoring of the personnel in our setting (there is no periodic test for evaluation of contamination). Biological monitoring and measurement of surface contamination should be considered when preparing a local guideline for safe handling practices in our country. The results of the current study will be used to conduct the future study in several oncology settings.
In summary, inadequate and inefficient exposure controls in our setting have led to adverse health effects in our health care workers. We recommend establishing a local safe handling guideline covering all applicable exposure controls in order to decrease occupational exposure to ANPDs.
Conflict of interest
All authors declare no conflicts of interest.