
Abstract
BACKGROUND:
Infection as a consequence of splash sharps and needlestick injuries (SSNIs) is a hazard faced by healthcare workers. Little is known about the impact this has on quality of life particularly in countries where the risk of infection is high.
OBJECTIVE:
This study aims to describe the impact SSNIs have on the quality of life of healthcare workers in Kenya, where blood borne illness prevalence is high.
METHODS:
A hospital-wide survey of a facility in Nairobi was conducted. Data was collected online from at risk healthcare workers using Burckhardt and Anderson’s Quality of Life Scale (QOLS) and a 10-item symptoms questionnaire.
RESULTS:
Of the 416 participants, 192 (46.2%) had experienced SSNIs. Their mean QOLS scores were considerably lower than that predicted for a healthy population. The relationship between symptoms and QOLS scores showed a strong positive correlation (Pearson’s r = 0.753). Tests of association between QOLS scores and SSNI type, anti-retroviral (ARV) drug use, educational level and staff cadre revealed significant association (p < 0.05). However, on key demographic variables, the association was non-dependent, indicating that the impact was felt similarly by many staff.
CONCLUSIONS:
SSNIs clearly impact on healthcare workers quality of life. Hospital management should ensure measures are taken to reduce SSNIs and provide appropriate personal protection equipment. For staff experiencing an SSNI, psychological wellbeing should be assessed and appropriate expert help provided.
Introduction
Healthcare workers (HCWs) are at risk of occupational exposure to sharps, splashes and needlestick injuries (SSNIs) because of the nature of their work. Prüss-Üstün, Rapiti and Hutin [1], estimated that in the year 2000, there were about 16,000 Hepatitis C Virus, 66,000 Hepatitis B Virus and 1000 HIV infections globally. Out of these, 39% of Hepatitis C, 37% of Hepatitis B, and 4.4% of Human Immuno-Deficiency Virus/Acquired Immuno-Deficiency Syndrome (HIV/AIDS) infections were attributed to occupational exposures amongst HCWs. From 1985–2013, 58 confirmed and 150 possible cases of occupationally acquired HIV infection among HCWs were reported to the Centers for Disease Control and Prevention in the United States (USA) [2]. Similarly, the Health Protection Agency in the United Kingdom (UK), between 1984 and 2005, reported that in total, there had been 5 documented occupational HIV seroconversions and 14 possible seroconversions [3].
Studies suggest HCWs are aware of these risks and the negative impact on their quality of life (QOL) [4–7]. Unfortunately, for Kenya and the Sub-Saharan region where blood-borne pathogens (BBPs) such as HIV/AIDS [8], are endemic, the impact of SSNIs on the QOL of HCWs has not been sufficiently studied. It is noteworthy that, previous studies [4–7] of this kind have been conducted in western countries, but these have limited value and lack generalizability [9] when comparing their findings to a Kenyan context.
As a result, the main aim of this research was to conduct a cross-sectional descriptive quantitative study, to assess the impact of SSNIs on the QOL of HCWs in a Kenyan University Hospital. This work is relevant to occupational health practitioners, counselling psychologists, infection control practitioners and healthcare managers charged with improving workplace safety and employee health. The results may indicate how a more holistic and sensitive occupational health response to HCWs sustaining SSNIs could help address both their immediate and more long-term concerns. Across Sub-Saharan Africa, research into important employee health and safety issues like this, are crucially lacking.
Literature review
Epidemiology of SSNI and HCW risk
SSNIs are a prevalent occupational hazard amongst HCWs [1, 10]. A recent cross-sectional study in Kenya examined 1,665 cases of SSNI’s over four years from 2011–2014 and suggested incidence was increasing [11]. Ugandan research [12] (Uganda shares a border with Kenya), found an SSNI prevalence rate of 46% amongst HCWs. However, underreporting of these accidents means this may not be an accurate picture. Makhoka [13], estimated a non-reporting rate of about 40% in the hospital involved in this study. Studies elsewhere in the world show that 35% to 62% of SSNIs are not reported [14–17]. This is important to HCWs in this study because they are at greater risk because of the high prevalence of BBPs in the general population in sub-Saharan African countries.
Globally, the United Nations Programme on HIV/AIDS (UNAIDS) in 2015 stated that 36.7 million people were living with HIV, 19 million, roughly 52% of those living with HIV were in eastern and southern Africa [8]. Locally, the Kenya Aids Indicator Survey of 2012 [18] showed that the HIV prevalence rate stood at 5.6% amongst adults between 15–64 years (approximately 1,192,000 people). By comparison, there were only 98,400 people living with HIV in the UK in 2012 [19].
Besides, the HIV burden, the African continent also has high numbers of people infected with chronic hepatitis B, C and A, which puts the health of HCWs at further risk [20]. In a recent systematic and pooled data review from 1965 to 2013; Schweitzer, Horn, Krause et al. [21] estimated global hepatitis B surface antigen (HBsAg) seroprevalence for chronic hepatitis infection and reported that it was highly endemic in the WHO African Region (total 8.83%, CI 8.82–8.83). Kenya has a rate of 5.16% (CI 4.86–5.48) compared to developed countries like the USA where the rate was only 0.27% (CI 0.24–0.30).
At even greater risk, are HCWs who sustain SSNIs from source patients who are already infected with BBPs. The recent cross-sectional study in Kenya [11] revealed that out of 851 cases where source patient HIV status was known, 39.4% proved HIV positive and although only 45 (5%) of source patients status was known for Hepatitis B, 15 affected workers (36.6%) proved positive for the antigen representing infection. It additionally indicated that other risks to Kenyan HCWs included low Hepatitis B vaccination coverage, a lack of testing for antibody titres, ineffective management of post exposure prophylaxis (PEP) services, inadequate staff knowledge of risk and a lack of psychological support in the event of exposure [11].
The merging of all these factors not only creates a risky situation but is a cause of worry for HCWs who sustain SSNI’s. There are also additional PEP treatment side-effects that affected HCWs may have to bear. All these issues may impact on and influence how HCWs appraise their general well-being and life quality following exposure.
Quality of life (QOL) concept and SSNIs
The World Health Organization (WHO) described QOL as “…an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” [22 p.1] It encompasses one’s state of physical health, psychological state, level of independence, social relationships, personal beliefs and is affected by the environment one interacts with [22]. QOL is a multidimensional concept that includes the subjective evaluation of both the positive and negative aspects of one’s life [23]. QOL is an important measure for clinical outcomes which has been applied to many chronic conditions to understand the impact of disease on people’s lives overall and looks beyond their symptoms [24].
While reports on how cancers, diabetes and other chronic conditions, impact on patients QOL, little is known about SSNIs and their impact on QOL. A few studies have explored this but their results are mainly limited to physical and psychological symptoms and not overall QOL as conceptualized by WHO [22]. For example, Zhang and Yu [25] in their Chinese study showed that 15.2% of their participants experienced emotional distress such as anxiety, worry, frustration, panic; post-SSNI, while bigger numbers, (57.6%), feared being infected from the exposure. Similarly, Gershon et al. [4] found that 85% of HCWs who were started on PEP treatment had adverse side-effects which mostly included nausea, stomach ache, fatigue, headache and diarrhea. They also found that the psychological symptoms suffered included, 53% of respondents feeling anxiety, 18% experiencing insomnia, 13% depression, and 10% experiencing a loss of appetite, another 10% affected with sleepiness, and another 10% are frequently crying. Other studies have also associated mental health problems such as depression and post-traumatic disease syndrome (PTDS) with SSNIs [7, 27]. Stigmatization and social isolation in relation to occupational exposures to BBPs through SSNIs have also been reported [5, 28–30]. Other difficulties involving both sexual and relational problems have also been highlighted as consequences of SSNIs exposure [4, 31].
QOL measurement is often considered only a health-related outcome [32]. Clinical Outcomes Models and Health-Related Quality of Life (HRQOL) are examples of some measures that have been applied in quality of life studies, but they have limitations and weaknesses since they focus mainly on health, function or symptoms related factors in what they assess and so do not comprehensively address QOL [32–35]. Gill and Feinstein [36] contend that QOL measurement can only be achieved by incorporating the person’s view of what is uniquely important to them, with regard to both their health status and their wider lives. According to the developers, Burckhardt and Anderson’s [33] Quality of Life Scale (QOLS) tool does this and has proved to be appropriate in measuring the phenomenon of QOL. It has cross-cultural applicability and is capable of measuring quality of life conceptually distinct from health status or other causal QOL indicators [33]. The Burckhardt and Anderson 16-items self-reported QOLS was originally developed by Flanagan [37] but was later refined by Burckhardt and Anderson to its current form [33].
The importance of undertaking QOL studies is that they can inform healthcare service development and efforts to seek care outcome improvement. For example, DiSipio, Hayes, et al. [38] found out that the health-related quality of life (HRQOL) of younger breast cancer survivors (<50 years of age) at 6 months was lower at a mean of 80.2 compared to that of older women (>50 years) with a mean of 87.1. Having discovered that younger women’s physical and emotional wellbeing was impaired they suggested a targeted intervention to improve younger women’s’ views of their wellbeing. Other researchers have also studied different patient groups including those with sickle cell disease and fibromyalgia [38, 39] to understand how these diseases impact on people’s QOL and what developments in their care could lead to improvement.
Aims, objectives and hypothesis of the study
The main aim of this study was to investigate the impact of SSNIs on the quality of life of HCWs in a non-publicly funded teaching hospital in Nairobi, Kenya. It was hypothesized that the impact on QOL on HCWs following an incident of SSNI is independent of the variables; age, sex, professional cadre, experience, marital status and level of education. The specific objectives of this study were: To describe the level of impact on QOLS scores of HCWs who reported experiencing an SSNI in the last 5 years. To assess the relationship between selected symptoms associated with an SSNI and the QOLS scores of HCWs. To test, if any, the relationships that exist between QOLS scores of the HCWs and the variables of; type of SSNI experienced, antiretroviral (ARVs) use, age, sex, profession, experience, marital status, and level of education.
Methodology
The design was a cross-sectional survey involving 1,005 employees in the hospital who were assessed to be at risk of SSNIs and infection by BBPs. The total number of hospital employees was 1,508. The 1,005 surveyed included doctors, clinical nurses, unit assistants, Central Sterilization and Supply Department (CSSD) Technicians, laboratory, radiology and pathology employees, dental unit employees, house-keeping stewards and laundry employees. The remaining 503 employees who worked in offices and other non-clinical areas were not at risk of occupational exposure to SSNIs and were therefore excluded.
Once ethical approval was given by the Hospital, and initial piloting of the data collection tools was completed, an email containing a SurveyMonkey web link was circulated to all at-risk employees. The web link contained a standard participant information sheet and the finalized questionnaire. Data collection was anonymous and implied consent was considered granted if the person went on to complete the questionnaire. This ensured confidentiality and reduced the risk of coercion in data collection. In areas such as CSSD, housekeeping and laundry where staff had limited access to work computers; floor meetings were held for clarification purposes and to answer any concerns from potential participants. Printed questionnaires in sealed envelopes were later distributed to the employee members who consented to participate in the study from these departments. These were returned anonymously to the researcher.
Data collection tools
Data collection was carried out between May to July 2013 using Burckhardt and Anderson’s [33] 16-items self-reported Quality of Life Scale (QOLS) and a 10- item self-reported symptoms questionnaire which also explored the demographic variables considered useful for analysis. The 16-QOLS items cover six broad domains; material and physical well-being, relationships with other people, social, community and civic duties, personal development and fulfilment, recreation and finally independence. Each of the 16-QOLS questions has a 7 point Likert scale where; 1 is described as ‘terrible experiencing of life’ and 7 is ‘delighted’. The total maximum possible score for QOLS is 112 points and the lowest is 16 [33]. The higher the scores, the better the person’s QOL, lower scores predict poorer QOL [33]. It is estimated that a score of 90, represents the expected average score for a general population [33]. QOLS has a high reliability and internal consistency with a Cronbach’s α between 0.88 to 0.92 noted in different studies [40, 41] making the QOLS both a valid and reliable tool for studies of this type, hence its selection for use here.
The symptoms questionnaire explored whether lack of appetite, tiredness, nausea and vomiting, difficulty sleeping, anxiety and worrying, reduced the desire for sexual intimacy, nervousness and despairing about the future, feeling depressed and lastly diarrhea were experienced post-SSNI and during PEP treatment. The symptoms questions and responses were also presented as Likert scales from 1 to 6; with score 1; being ‘symptoms experienced all the time, more than once a day’. A score of 6 meant ‘no symptoms were experienced at all’. The lower the scores the worse the impact of experienced symptoms would be and vice versa.
The questionnaire also included one open-ended question to collect some views from the respondents on their SSNIs experience.
Data analysis
Data was imported from SurveyMonkey to an excel sheet, cleaned and automatically coded via SurveyMonkey software. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 15.0 [42] with the help of a statistician. A Cronbach’s α reliability test was conducted for 26 items, 10 in the symptoms scale and 16 in the QOLS to ascertain to what degree the indicators that made up the measurement scales were consistent with each other. The results yielded a Cronbach’s α of 0.982 which compared favorably to previous studies using QOLS [40, 41].
A Shapiro-Wilk test was also performed to determine the distribution of the data in order to choose appropriate statistical analysis methods [43]. The results showed that p < 0.05 meaning the data was of non-normal distribution and the appropriate test methods were therefore non-parametric [9]. Tests such as Pearson’s Chi-square (X2) for test of association and Pearson’s rho (r) tests for correlations and Pearson’s coefficient of determination (r2) were thus considered the most appropriate means of analysis. The relationship between symptoms and QOLS are presented using a Scatter Plot diagram (See Fig. 3).
Results
Socio-demographic characteristics of participants
After data cleaning, 416 completed responses were received from the 1005 eligible participants giving a response rate of 41.4%. This was similar to the response rate of 46% achieved in a similar hospital-wide study of SSNI’s in Uganda [12]. Of the 416; 55.3% were females and 44.7% male. The age bracket 25–34 years was the most populous which is reflective of wider Kenyan demographics [11]. Many of the respondents (25.7%) had at least a diploma level of education. Nurses, more than any other cadre of staff were the most likely to respond (25.4% of the total). Amongst the participants; 46.2% (n = 192) answered: “Yes”; while 53.8% (n = 224) responded “No” to having had experience of SSNIs in the previous five years (Table 1).
Socio-demographic characteristics of study participants
Socio-demographic characteristics of study participants
Of the 192, “yes” responders (Table 2), the majority were within the age bracket 35–44 years (39.1%), followed by those aged between 25–34 years (37.5%). Males (50.5%) were affected, more than females (49.5%) and doctors (26%) had more experiences of SSNIs than any other employees’ type, similar to findings by Makhoka [13] and Zafar et al. [43]. The “yes” responders also suffered more needlestick injuries (46.4%) than any other type of SSNI which is also consistent with previous studies [13, 45]. The devices most involved are syringe needles for intramuscular and subcutaneous injection (34.2%) and the major activity resulting in most needlestick injury was giving injections (30.9%) [11].
Socio-demographics by reported SSNIs event experience
Across all employees, 43 (22.4%) suffered exposure through handling contaminated linen and waste. This exposure rate was high compared to that found in Gershon et al.’s [4] USA study in which only 10% of SSNI incidents were via contact exposure. Although this study and Gershon et al.’s [4] had different sample sizes, the higher percentage of employees exposed as a result of unsafe handling of waste/linen particularly, could be explained either as a sign of greater willingness to report incidents, or poorer compliance to appropriate PPE use.
Generally, the majority of SSNIs, 88 (45.8%) occurred four to five years ago; 58 (30.2%) happened two to three years ago with only 46 (24%) within the past year. This is indicative perhaps of a reducing incidence as a result of efforts by the hospital to improve safety within the workplace. This is in contrast to a national study which showed increasing cases of SSNIs [11]. The married (65.1%) and those with diploma qualification (26.6%) sustained more SSNIs perhaps due to solely to their greater presence within the workforce. Those that had worked >5 years (64.1%) within the organization had more SSNIs which may just be a consequence of the fact that they have been at risk longer than those that have been in healthcare for a shorter time. When comparing the frequency of SSNIs, 66.1% stated it had happened to them only once and 33.9% said more frequently than this. In 46.9% of SSNIs, Antiretroviral Viral (ARVs) for PEP had been administered. This compared to only 10.1% in the national study [11]. This is perhaps indicative of ease of access to PEP services in the study hospital compared to accessibility in other local healthcare providers.
The impact of SSNIs on QOL of HCWs was assessed using both the QOLS and symptoms scale scores for the “yes” responders (n = 192). The symptoms scores were processed and described in two levels as; those who were ‘most affected’ versus those ‘least affected’ to bring greater clarity to the data. The ‘most affected’ experienced the selected symptoms frequently, from more than once daily to more than once per week and their symptom scores were lower; ranging from 1 to 3 in the 6-point scale used. It revealed that just over half (52%) of HCWs felt depressed, suffered anxiety and worrying (51.6%) and were ‘despairing about the future’ (50%). The results are summarised as in Fig. 1. Gershon et al. [4] noted that 53% of their respondents had feelings of anxiety, 18% insomnia, 13% depression, 10% a loss of appetite, 10% sleepiness, and 10% frequently cried, confirming that it is psychological symptoms that most staff experience post-SSNI.
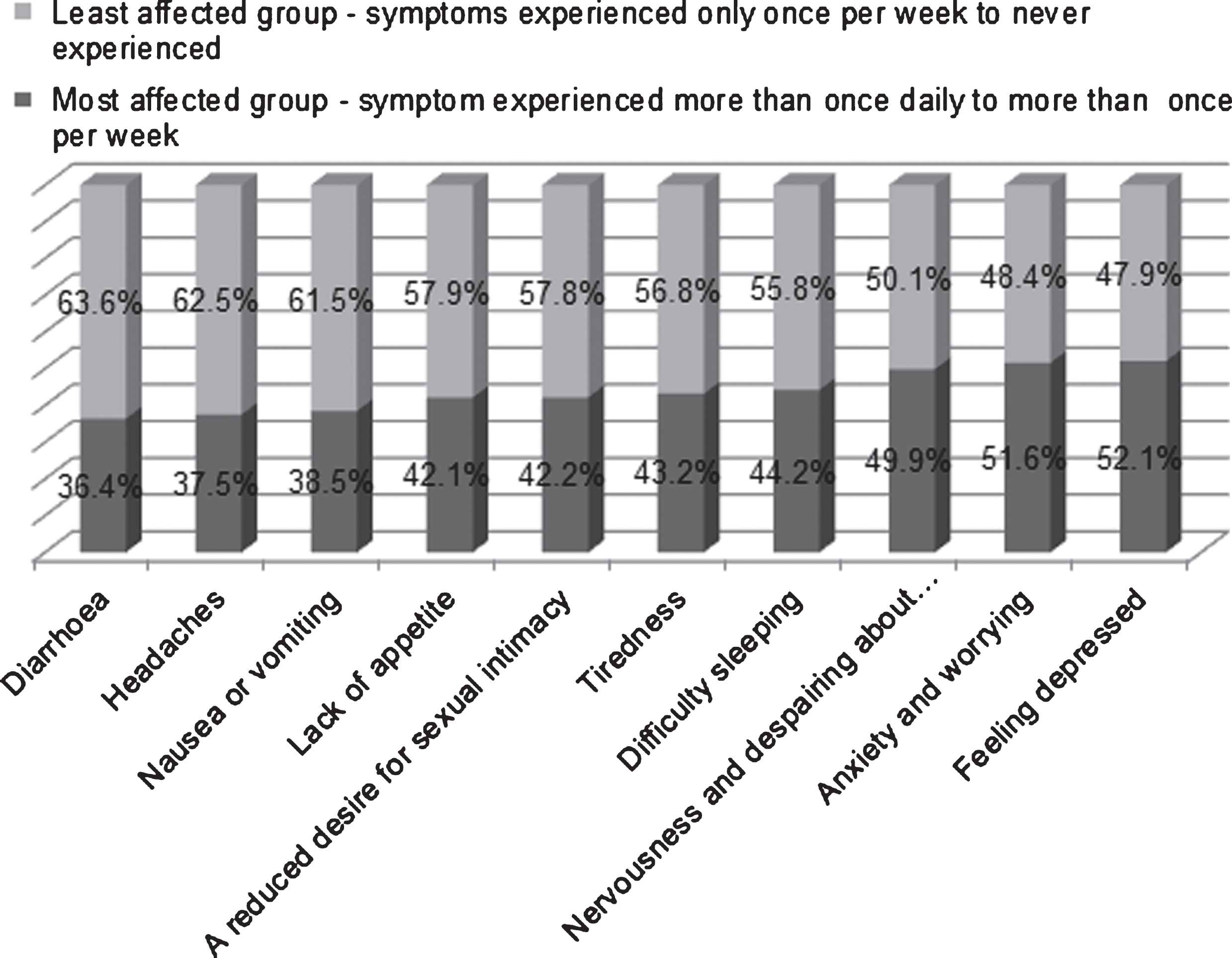
Percentage of HCWs “most affected “and “least affected” with symptoms burden following SSNIs (n = 192).
The QOLS scores were calculated as recommended by Burckhardt and Anderson for the affected 192 workers to show the impact on their QOL. The lower the scores were, the poorer the QOL and vice versa [33]. The total scores for HCWs ranged from 32 to 112 with a mean score of 79.2 (SD = 20.33). The mean score was less than the predicted 90 for a generally healthy population [33]. Noticeably, there were variations in QOLS means scores for HCWs who had different demographic variables (See Table 3). For instance, the mean scores for males were higher (81.4) compared to that of females (76.9). Similarly, the ‘married’ mean was 81.3 compared to the ‘singles’ score of 75.3, perhaps because the ‘married’ received better support (from partners) than the ‘singles’ did at the time of their SSNI incident. Notably though, it was HCWs who used ARVs who had the lowest mean score of 64.8 followed by those who had needlestick injuries, as opposed to any other type of SSNIs.
Mean Symptoms and QOLS scores comparisons
The expected pattern of results where lower symptoms scores corresponded with lower quality of life scores was noted. However, overall these scores were lower than the QOLS scores achieved in the Norwegian general population study [40] where analysis was conducted looking only at lower scoring respondents who had disease or health problems. This unwell group from Norway’s mean score was 79.6 (SD = 13.8).
To establish if there was any relationship between symptoms and QOLS score, a scatter plot was drawn with QOLS scores on the Y- axis as the response variable and symptoms scores on the X-axis (Fig. 3). The relationship between QOLS and symptoms scores was found to have a linear positive trend, r2 = 0.567 which is a moderate and positive relationship. Furthermore, Pearson’s coefficient of correlation (r) was found to be equal to 0.753, which indicated a positive association between symptoms and QOLS scores. This confirmed that the level of symptoms experienced by HCWs was positively associated with their quality of life. The higher the symptoms scores were, indicating a lesser impact of symptoms, the higher the QOLS scores were, therefore, the better quality of life was for affected HCWs, and vice versa.
To further identify the level of QOL impact on each of the 16-QOLS items, the scores in the Likert scale ranging from “Terrible” as the lowest score (1) to highest “Delighted” (7) were calculated [33]. The initial results which are given in detail (See Fig. 2) were presented in three groups for better and clearer understanding. Those who scored from 1 to 3 in each item, were generally ‘dissatisfied’ indicating a poorer QOL. The second group comprised of those who had ‘mixed’ feelings and scored the midpoint on the Likert scale, which was 4. The last group was those who were ‘satisfied’. The ‘satisfied’ group scored from 5 to 7 and was assumed to have the better quality of life. In the 16-QOLS items, the greatest dissatisfaction expressed by HCWs (by 24.5% of respondents) was with the item ‘plans to have and rear children’ (Fig. 4). This was a unique finding for this study. Other researchers have employed this analysis yielding different results. For instance in a study involving Sickle Cell disease patients, work – related QOLS item had the lowest score because many participants were jobless because of their disability [39].
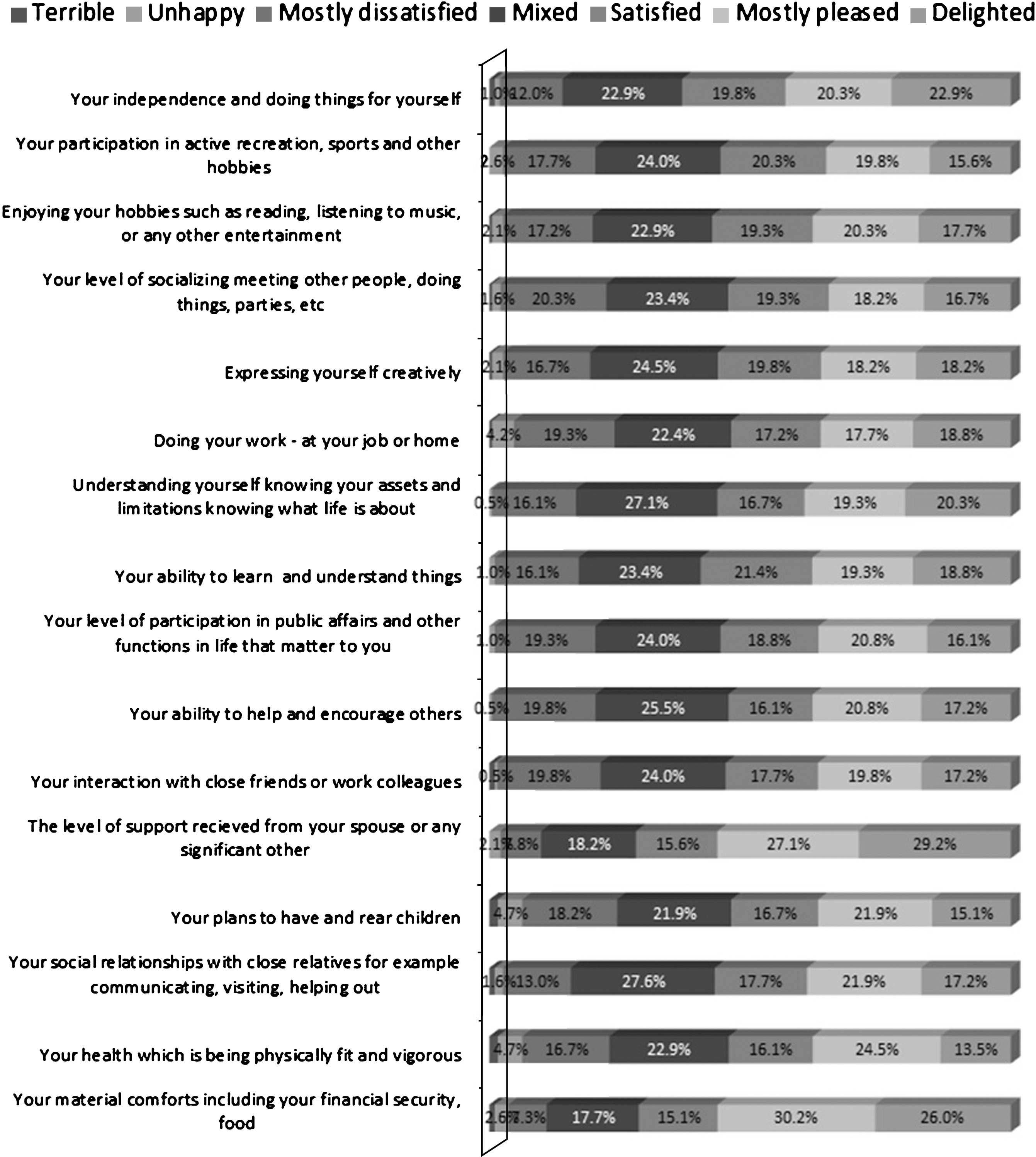
Percentage score of HCWs in each QOLS item following SSNI.
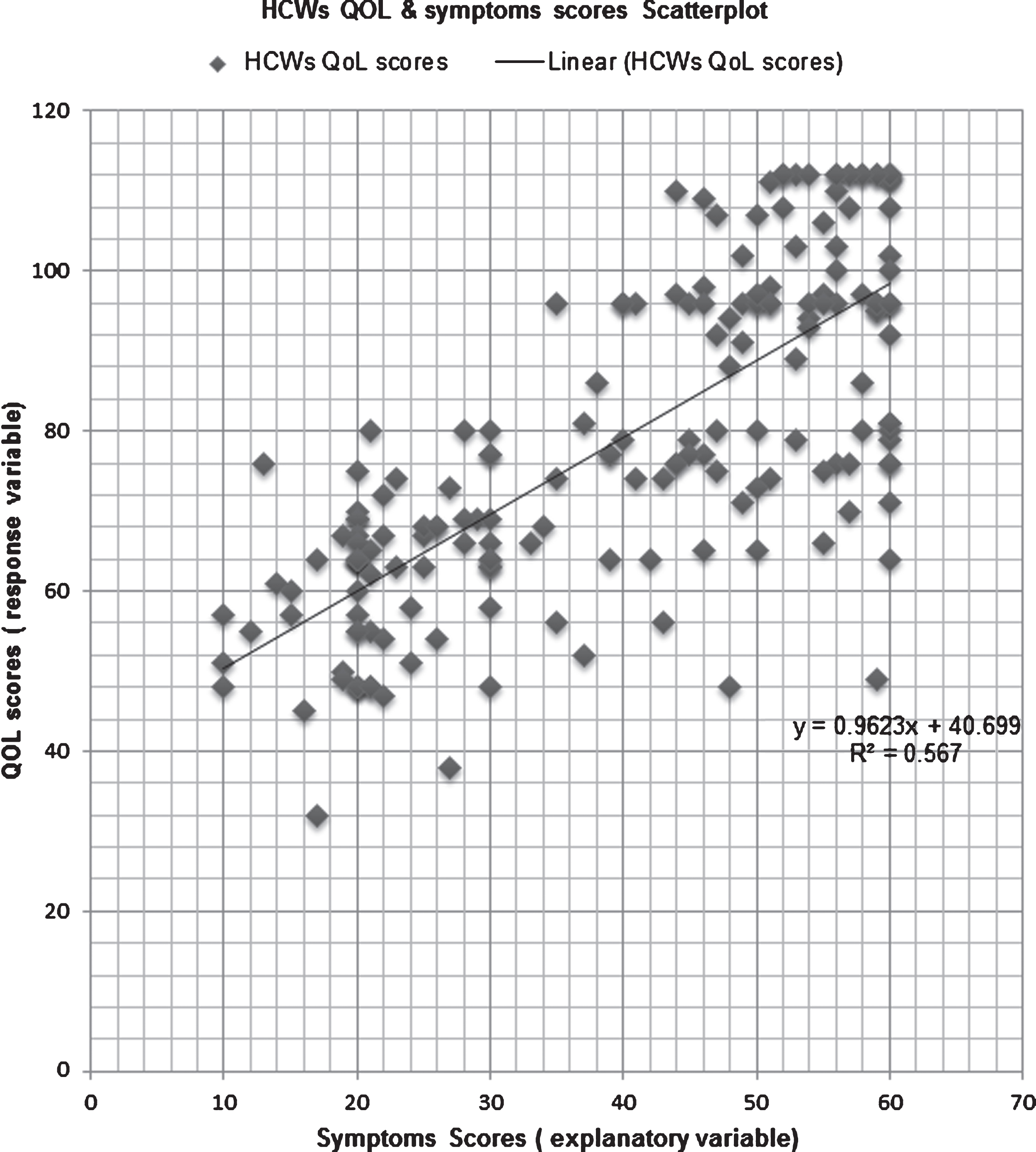
Relationship between symptoms and quality of life scores.

Percentage of HCWs responding “dissatisfied,” “mixed” or “satisfied” to the QOLS items following SSNIs.
In trying to establish if relationships existed between the independent variables of age, sex, professional cadre, experience, marital status, level of education and ARVs use and the QOLS scores of HCWs following SSNIs; results showed that SSNI type, ARV use, level of education and employee cadre generally had statistical association (p < 0.05) to QOLS scores. However, there were specific QOLS items which didn’t have any statistical significance. These are summarized in Table 4.
Testing any relationship between the independent variables and QOL scores following SSNIs
Finally, 43 HCWs responded to the open-ended question about their SSNI experiences. These were summarized into thematic areas and the majority of the comments, roughly half, were related to the impact of SSNIs on their lives. One HCW stated;
“The side-effect of medication was unbearable. Plans for vacation were put on hold as I couldn’t travel”.
Fifteen responses were associated with service delivery relating to the management of SSNIs within the study hospital. Five were about safety standards and practice issues, such as the need to enforce compliance with good practice on waste management, the use of appropriate personal protective equipment (PPEs) and easy access to first aid facilities such as an eyewash sink in cases of splashes with body fluids. Three people responded regarding other more general issues. Nonetheless, for some, the SSNI incident was seen as a learning event. For instance, one staff member learned to think more about safety practices and commented,
“We should be careful as we work in our respective places”.
The important role of the occupational health service was also recognized. For example, one respondent felt,
“The hospital has sensitized staff and (they) are aware of the procedures to follow in case of splash or a needle-prick injury.”
The main objective of this study was to assess the impact of SSNIs on HCWs QOL. Specifically, it explored the extent of this impact as measured by both reported symptoms and Burckhart and Anderson’s QOLS [33]. It also tested the relationship between selected symptoms associated with being affected by SSNI’s and their treatment and QOLS scores. Finally, it examined the relationship, if any between the QOLS scores of the HCWs involved and the following variables; type of SSNI experienced, antiretroviral (ARVs) use, age, sex, profession, experience, marital status, and level of education.
The results revealed that of the HCWs who had experienced SSNIs (n = 192), the majority (46.4%) were sustained by needlestick injury involving devices such as injection needles or cannulae. This high prevalence is consistent with findings in other literature [13]. Needlesticks carry the highest risk of transmission of BBPS to HCWs [2]. The US Center for Disease Control estimated that the occupational risk of transmission of Hepatitis B Virus (HBV) amongst HCWs was 22–31%, Hepatitis C virus was 0–7% and Human Immuno Deficiency Virus 0.09–0.3%. But, the risk of transmission of HIV alone was higher (0.3%) in percutaneous injuries compared to 0.1% for splashes to the mucous membrane and <0.1% in non-intact skin [46]. HCWs seem to be aware of this risk and it does impact on their QOL as reflected in the findings of this report. One study conducted in an Israeli hospital, Tabak, Shiaabana and ShaSha [6] established that there is a correlation between perceived severity of diseases contractible from needlestick injuries and the level of reporting compliance. They found that those who reported their injuries perceived their threat of contracting a disease more highly than non-compliers. It is likely that risk perception heightens the psychological manifestation of stress symptoms. This is also demonstrated within the findings of this study.
Some variables around type of SSNI incident had an impact on QOLS scores. For example, the experience of a needlestick injury compared to any other type of SSNI produced a mean score of 69.3 in the QOLS; while the use of Antiretroviral (ARV) for post-exposure prophylaxis produced a much lower mean score of 64.8 (Table 3). Low QOLS scores were usually a result of ARV drug side effects such as diarrhea, headache, loss of appetite, lethargy and tiredness reported by many HCWs. It can be inferred that the physical and psychosocial symptoms some experienced curtailed significant life events such as travelling, sports participation and even plans to have children. Each of these affected events had an impact on how HCWs subsequently assessed their QOL. Comments from the open-ended question help illustrate this, for example one person stated that:
“The side-effect of medication was unbearable. Plans for vacation were put on hold as I couldn’t travel”.
Fayers, Hand, Bjordal and Groenvold [47] argued that the presence of causal indicators such as treatment side-effects or symptoms can cause a change in quality of life evaluation. This view is supported by Smith, Avis, and Assmann [48].
As mentioned within the results a positive relationship between symptoms and QOLS was found confirmed by the scatter plot diagram (Fig. 3). However the Pearson’s coefficient of determination suggested that r2 = 0.567; meaning that 56.7% of the QOLS scores are likely to be related to the symptoms scores. However, that means that the remaining 43.3% relate to other issues within the QOLS items or perhaps outside them. It is worth noting that there may be other confounding factors that may have an impact on the QOL of HCWs which may be unrelated to SSNIs, such as workplace discrimination or verbal abuse [49, 50].
As well as the general impact of an SSNI on QOLS, how each of the 16-QOLS items was affected was also analyzed. This had been done by previous researchers looking into some chronic diseases which produced different outcomes [39, 51]. In this study, “plans to have and rear children” was the most affected QOLS item (24.5%; Mean 4.73, SD = 1.544) (See Fig. 4). The reasons for this are not fully understood. Anecdotal and personal accounts of HCWs who have experienced SSNIs suggest that their mental, psychological and emotional state has an impact on their sexual relationships [52]. The symptoms results may support this as 42.2% of HCWs actually expressed reduced desire for sexual intimacy. Gershon et al.’s study [4] also casts some light on this. They quote one respondent stating:
“I was afraid to have sex with my spouse, but he did not understand my concerns, and we are separated now. I feel it’s because of the problems we had when I got exposed.”
Another individual within the same study commented:
“I refused to have sex for four months... It was hard on my wife, as we wanted to start a family.”
The concerns regarding engaging in sex during this period may be complex ranging from fear of infection and transmission, dislike of the requirement to use condoms to protect partners against potential transmission of BBPs, psychological stress and tiredness a result of stress or ARV use. Tackling this issue therefore, requires sensitive professional counselling and psychological support when it arises. This may require meeting both parties. Gershon et al. [4] found out that the partners of the victims can be equally traumatized by the event. This gives further credibility to the requirement to consider QOL as a whole, dependent on the subjective experience of the individual in specific circumstances and this needs consideration when creating a person focussed response for any HCWs who sustain SNNIs. Such programs need to be sensitively designed to ensure the needs of HCWs are addressed beyond just administration of PEP ARVs.
Some, QOLS items such as “level of support received” were less affected. Only 9.9% of HCWs found this dissatisfying compared to 24.5% in the worst affected item (See Fig. 4). Perhaps the reduced effect is explainable by the fact that most participants were married (65.1%), and appeared to have received a high level of support from their partners which may have helped to ameliorate the situation. The “financial and material” item in the QOLS was also one less affected amongst participating HCWs Only 10.9% expressed dissatisfaction. A possible reason for this is because labor laws in Kenya protect workers against any financial loss caused by workplace injury; therefore, as much as they were experiencing other problems, most could meet their financial obligations.
Finally, statistical evaluation revealed that SSNI type, ARV use, level of education/training and employee cadre generally had an association (p < 0.05) to QOLS scores as summarized in Table 4. In as much as some variables had a strong association, there were no clear correlations found. This may be because of the global nature of QOLS; which is influenced by a number of factors beyond health status [26, 51] which may be difficult to unravel. It is probable that the significant association of level of education and QOLS scores may be linked to job tasks and the employees’ professional backgrounds. SSNIs, ‘at risk’ populations are likely to be from certain professional cadres based on both their education level and the skills they possess. Doctors, nurses and students have been identified as at more risk than other professional groupings [25, 52]. When you consider the riskiest SSNIs, needlestick injuries, they are primarily associated with tasks like injections or suturing principally carried out by this same staff grouping [29, 53–55]. This is important because proper employment procedures that look into training backgrounds, and the knowledge and skills of this staff group are crucial to workplace safety. Although work experience had only significant associations in 6 out of 16-QOLs items (p-value<0.05), it had very strong positive correlations to most QOLS items (15 out of 16). Perhaps, these strong correlations can be attributed to the fact that more experienced employees may have a better understanding of their injury and what needs to be done. They may also be more aware of the level of risk involved and the possible impact of side-effects that accompany ARV use.
Sex, age, marital status and work experience in relation to quality of life after SSNI, did not yield statistical significance (p > 0.05). This indicates that the impact of SSNIs on QOLS may be independent of these variables implying that the perception of risk, the experience of adverse effects of ARVs and the impact on QOL of HCWs may be similar for all. This to an extent confirms one of the hypotheses of the study, that SSNI victims experience an impact on their QOL that is not related to any clear demographic variables.
Limitations of the study
This study would have been aided hugely had a QOLS study been completed that examined the Kenyan general population. This study relied on the reference point mean score of 90 for a healthy population based on Anderson and Burckhardt’s initial view of the QOLS [32] but that may not be appropriate to a Kenyan context. According to Wahl et al. [40], comprehending and comparing any QOL indicators or measures in a study is helped if there is a wider general population reference comparison score. The ability to compare the QOLS scores of affected hospital staff with their peers outside the hospital would have helped to assist in showing just how much of an impact an SSNI was having on staff. Data collection by self-completion introduced a risk that respondents would either under-rate or over-rate their scores, although work by Bliven, Kaufman and Spertus [56] suggests that electronic collection of QOL data was just as reliable as any other method and was the preference for 45 (82%) out of the 55 people who participated this way in their study. The issue of the effect of other wider confounding variables that may influence QOLS scores was more problematic, particularly since the QOLS scores for HCWs who were not exposed to SSNIs were not collected.
It is important to note that the study hospital is a private facility with several safety and quality improvement initiatives in place, including employee health programs that can be accessed easily by HCWs who sustain SSNIs. This is atypical in Kenya, where the international standards adopted by this hospital may not be representative of other Kenyan health care facilities. As a result, further studies which involve local public healthcare facilities may have provided data that better reflects the wider national picture.
Conclusion
This study demonstrates that HCWs in a university hospital in Kenya are aware of the risks posed by SSNIs and when it does occur this awareness influences negatively how they appraise their state of wellbeing and quality of life. The impact is global and multifaceted and includes emotional, psychological, social, relational and physical symptoms, especially when the additional impact of the side effects of ARV medication used during PEP are considered.
A clear relationship between the symptoms that HCWs experience and their QOL was established. Low scores on the symptoms scale, recorded by the HCW’s who experienced symptoms most often, resulted in poor QOLS scores, implying that there was a positive and strong link between exposure and treatment for SSNIs and perceived QOL thereafter. Looking more closely at the QOLS scores and the independent variables measured, four areas; SSNI type, ARV use, educational level/training and staff cadre yielded significant associations with QOLS scores. Some QOLS items were less affected.
The variations in statistical significance of the associations and correlations of QOLS scores with different demographical variables reflect the manner in which QOL was evaluated by HCWs and is based on their perceived risk and the impact this has on their physical, psychological and social wellbeing. It is important to understand how these personal perceptions can be addressed in the care of HCWs who sustain SSNIs. The findings are also useful as an illustration of the usefulness of QOL measures as a means of determining how meaningful staff health can be improved and re-designed.
These findings are also relevant to a range of practitioners from Occupational Health and Safety, Healthcare Managers and researchers working locally in the region.
Recommendations
From the results of this study, it has been suggested that hospital management should ensure that PPEs are provided and appropriately used by staff especially in areas like laundry services, where splash accidents were more prevalent that one might expect. Given that needlestick injuries were also more prevalent than any other type of SSNI, consideration should be given to the introduction of engineering controls i.e. safety needles that reduce the hazards and risks related to injection administration accompanied by further education, measures encouraged by Van der Molen et al. [54]. Where possible, the need for injections can also be reduced by encouraging the wider prescribing of oral medications.
Although the hospital already has counselling services, it emerged from some responses that these were not consistently provided by knowledgeable and experienced persons. It was also noted that sometimes there are missed opportunities to refer people who sustained SSNIs for psychological counselling. This could be addressed by the employment of additional psychologists to ensure services are provided in a more reliable and professional manner. Currently, the profile of this issue is being raised across the hospital through departmental safety and infection prevention talks. There have also been improvements in access for employees to assisted post-SSNI programs. Alerts to the occupational health and safety department via telephone or emails when SSNIs occur have been implemented, to ensure PEP and support services can respond at the earliest opportunity (within 1 hour of accidental exposure). The service will also make use of the information in this study to deal differently, more holistically and more empathetically to everyone who suffers an SSNI exposure.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We wish to thank the management of Aga Khan University Hospital, Nairobi (Kenya) for allowing us to undertake this study and all the support received from colleagues and the participating staff there. Many thanks to Francis Maina, the Hospital’s Statistician, for assisting with the statistical analysis of the data.