
Abstract
BACKGROUND:
Limited literature exists investigating biomechanical changes during a Functional Capacity Evaluation (FCE).
OBJECTIVE:
To determine change in joint angle measurement between minimum load to safe maximum load in the bench to shoulder lift of the WorkHab FCE.
METHODS:
Dartfish ProSuite was used to analyse bench to shoulder lift video from 28 subjects. Measurements of joint angle at lumbar spine, thoracic spine, elbow and shoulder at four points in the ascending and descending lift phases (0/3, 1/3, 2/3, 3/3) in the minimum load and safe maximum lift were collected. Paired t-tests were used to analyse differences in joint angles between lifts.
RESULTS:
Significant differences in joint angles were identified in the thoracic spine, elbow and shoulder at maximal weight. Increased extension occurred: Thoracic spine at 3/3 ascending [2.922, 95% CI 0.8, 3.8, p = 0.004]. Increased flexion occurred: elbow ascending [1/3:6.405, 95% CI –11.8, 1.8, p = 0.008],[3/3:15.575, 95% CI 4.2, 27.0, p = 0.009]; elbow descending [0/3:18.446, 95% CI 9.5, 27.4, p = 0.000]; shoulder ascending [3/3:16.785, 95% CI 11.8, 21.8, p < 0.001]; shoulder descending [0/3:16.647, 95% CI 10.6, 22.7, p < 0.001].
CONCLUSIONS:
This study provides insight into the biomechanical changes during a bench to shoulder lift and support observations and clinical reasoning used in determining the safe maximal lift.
Introduction
Manual handling injuries are a major burden and a dominant occupational health issue [1]. Manual handling is any activity that requires the use of force exerted by a person to lift, lower, carry, push, pull, hold or restrain an object [2]. During 2012, manual handling injuries cost the US government a total of $15.1 billion and accounted for 25.3% of total workplace injuries [3]. Similarly, in the UK, one third of workplace injuries were sustained during manual handling tasks [4]. In the Australian workforce in 2013–14, 54% of workers’ compensation injuries were related to sprains and strains of joints and adjacent muscles from over-exertion [5]. Manual handling of objects caused 27% of total workplace injuries or illnesses in Australia in 2009–10 [5] and back injuries alone are estimated to cost the Australian Government approximately $140 million annually [6].
Manual handling/lifting is a complex multi-stage physiological process, which requires the activation, recruitment and use of many different muscles, ligaments, tendons and bones in all parts of the body [7]. There are also multiple external factors which affect a lift, including the size and weight of the object being lifted, the shape of the object, the base of support and the pace at which the movement is being carried out [8–10].
Manual handling/lifting tasks cause the majority of overexertion injuries, which is also one of the leading causes of back injury [11, 12]. Overexertion arises when movements are performed under load, inappropriately for the individual [13]. Risk of overexertion related injury depend on both the inherent strength of the joint tissues and the amount of external applied loads [14]. All joints, have a limit of load, before injury is likely to occur [15]. This threshold varies between different joints, different types of load and different people.
Safe lifting guidelines, based upon task based lifting (such as the Australian National Standard for Manual Tasks [16], NIOSH lifting equation [17], and the WorkCover NSW Manual Handling Risk guide [18]) have been developed with the aim of reducing or preventing injuries. These guidelines discuss both generic and more specific recommendations for different lifting tasks and lifting situations (lifting from floor, waist, shoulder or overhead) based upon the associated risks in each of these. During a bench to shoulder lift, the joints most at risk are those in the upper limb, back and neck, where most joint movement occurs and where the greatest amount of load is applied [19]. Further to this, the majority of movement and manipulation of the object is controlled by the upper limb [20], which places the upper limb at risk of injury during this lift. Workers in jobs which require repetitive shoulder movements are at risk of developing occupational shoulder disorders, such as tendonitis, particularly where there is vibration involved in the movement [21]. The shoulder, or glenohumeral joint, is the most mobile joint in the human body and as a result of this mobility, it is very susceptible to injury [22].
Functional Capacity Evaluation (FCE) can assist in the prevention of such injuries by determining a worker’s physical capabilities and assisting in appropriately matching an individual with a task [23]. An FCE is a widely used assessment tool in both prevention and occupational rehabilitation settings [23, 24]. In an occupational rehabilitation setting, an FCE identifies physiological barriers which restrict Return To Work and establishes the safe physical capability of an injured worker [25]. This allows the results of the FCE to be matched with a job corresponding demands in order to minimize risk of injury [26]. A review of ten currently available FCE assessments in the US found that rehabilitation was the most common setting in which they were used [23]. In Australia, the WorkHab FCE is the most commonly used [24, 28]. The WorkHab FCE [29] is used in many different occupational rehabilitation settings and is a useful tool to establish an individual’s ability to perform specific work related activities or job related tasks [29].
In the WorkHab FCE, the safe maximal lift capacity is determined by the assessor’s observation of movement and heart rate data. The assessor looks for visual clues of compensatory movements specifically relating to stance: the ideal placement of the feet and a stable base; posture: maintenance of normal lordosis throughout the lift; leverage: keep loads close to the body and in the range of centre of gravity; torque: no rotation of the shoulder relative to the pelvis, and pacing: the use of smooth and controlled movement patterns [29]. It is noted various observations have been used to determine safe maximum lift during a FCE [29–31]. Biomechanical changes have been studied in the floor to bench and bench to overhead lift [31, 32] during the WorkHab FCE, with healthy individuals. Biomechanical differences between lifting of a light load and a safe maximal load were identified. In the waist to overhead lift changes in ulnar deviation, elbow flexion, shoulder flexion, shoulder extension and lumbar extension were found and in the floor to waist changes in lumbar flexion, hip flexion, knee flexion and ankle dorsiflexion were identified. These studies support the determinations made by a clinician in assessing safe maximal lift during a WorkHab FCE with biomechanical changes confirmed with video analysis [31, 32]. There is no such study of the bench to shoulder lift of the WorkHab FCE and limited literature focusses on alteration of the biomechanics of lifting during the bench to shoulder lift of an FCE.
The aim of this study was to provide some quantification of safe maximal lifting determination to support the clinical reasoning used by WorkHab FCE assessors to identify if there are postural and biomechanical changes that assessors can evaluate during a bench to shoulder lift. The hypothesis was that significant changes will occur in joint angle measurement as external load is increased from minimum to safe maximum levels in the bench to shoulder lift. This will allow WorkHab FCE assessors to have access to additional evidence of joint changes associated with determination of a safe maximum lift in the bench to shoulder lift.
Methods
Study design
This was a within subject observational study where subjects act as their own control [33]. The repetitive lifting component of the WorkHab FCE was simulated for this experimental study, with video data of subjects completing the lifting component collected. This study used the video data to compare the joint angles of the lumbar and thoracic spine, shoulder and elbow at minimum load and safe maximum load weights during the bench to shoulder lift. The video analysis tool of Dartfish Pro-Suite (Dartfish, Lausanne, Switzerland) was used to view subjects in a sagittal plane in frames selected according to time during the bench to shoulder lift. Joint angles in these frames were then measured with the Dartfish angular measurement tool which allows calculation of angles using on screen drawing tools. Ethical approval was granted from the University Human Research Ethics Committee (H-2015-0010).
Participants
Staff and students from the Callaghan Campus of the University of Newcastle, Australia were recruited for the study. Participants were excluded if they had pre-existing musculoskeletal injuries or conditions which would impede them from completing a manual handling task. Thirty participants provided informed consent, however only data from 28 were eligible to be included in this study.
Equipment/procedures
Prior to commencing the assessment, all subjects completed a pre-screening general health questionnaire, blood pressure measurement and a three minute step test to determine heart rate recovery as per the WorkHab FCE guidelines [29]. Participants’ joints were then marked. A single researcher trained in physiotherapy joint palpation skills marked each participant to minimise variation. Markers were positioned on the right lateral aspect of the participant’s bodies to capture the sagittal motion of the shoulder, and elbow, and on the middle of the spinous processes of C7, T7, L3 and S2. Spinous processes were marked using foam balls applied with double sided tape so they could be viewed in a sagittal plane and black ink or white tape was used to mark the other landmarks. (See Fig. 1). Dartfish Pro Suite was used to view videos, capture still images, and measure distances and joint angles using the in-built software features [34] (Table 1).

Position of joint markers.
Joint angle measurements
The FCE was administered by a WorkHab accredited assessor [29]. The lifting task was completed in a controlled environment using WorkHab FCE protocols [35], with a standard bench height of 700 mm, and modular boxes aligned at the level of the subject’s waist (approximately navel) and shoulder (approximately acromion). All subjects wore heart rate monitors throughout the assessment. As per WorkHab FCE protocols [35], subjects completed three lifting repetitions before weight was increased. The lifted box, which has cut out handles on the side (weighing 5.5 kg) was lifted from beginning to end height and returned. This was repeated three times before additional weight was added. Initially subjects lifted the empty box as the minimum lift. After three lifts were completed, weight was increased by the WorkHab assessor as per the WorkHab protocol, amount being dependent upon the individual subject and closeness to maximum safe capacity, this was repeated until a safe maximum lift, as determined by the FCE assessor, was obtained. The three indications listed in the FCE guidelines for ceasing lifting tasks are the observation of compensatory or unsafe movements, participants reaching their maximum heart rate, or participants choosing to stop lifting [29]. Lifting style and lifting and lowering speed was self-selected by participants.
Video cameras were used to record the lifting – these were Sony Handycam Camcorders (Sony, Tokyo, Japan), which were positioned to view the rear coronal and right sagittal planes. For analysis of the bench to shoulder lift in this study, the right sagittal plane angle was utilized. Still images were collected at four points during the minimum and safe maximum lift. These points were determined by identifying the lowest vertical displacement of the box when all 4 corners of the box first lifted off the bench and ended when the box was at its highest during the lift. Both were marked with a horizontal line which were used to time the ascending and descending phases of the lift separately and then broken into thirds to attain three equal points across each lift when comparisons could be made. Joint angles were measured from still images at 0/3, 1/3, 2/3 and 3/3 of each lift. In the ascending lift, 0/3 is the lowest point and 3/3 is the highest point that the box reaches. In the descending lift, 0/3 is the highest point of the box and 3/3 is the lowest point of the box, when the lift is complete – see Fig. 2.
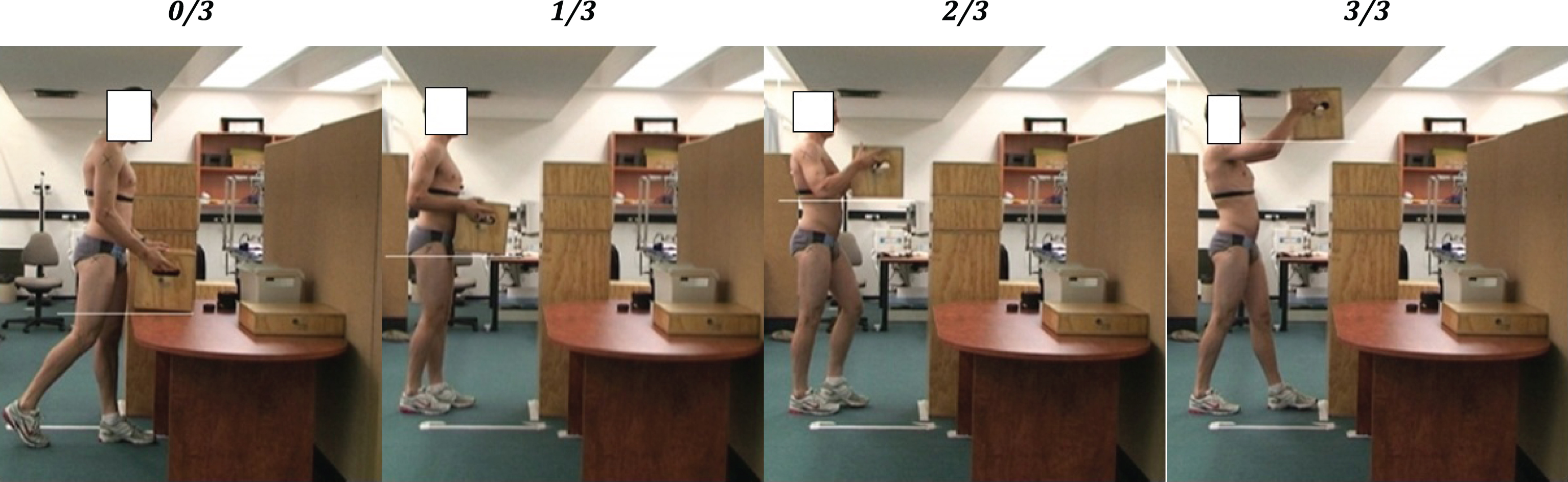
The four points in a participant’s maximum lift: 0/3, 1/3, 2/3, 3/3.
Joint angles at each of the eight points in the ascending and descending lift (0/3, 1/3, 2/3, 3/3) were measured using the Dartfish angular measurement tool (Table 1). Each subject’s second lift of the three repetitions at minimum and maximum weight was chosen for analysis. The second or middle lift was chosen to allow for comparisons across all subjects up to the maximum weight. Data were entered into the statistical analysis program SPSS version 22 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.) to calculate descriptive statistics -means and 95% confidence intervals (CI), intra-class correlation coefficients (ICC), and paired t-tests, with alpha at 0.5. For reliability, measurements were independently repeated for ten subjects selected at random. Two raters selected the ascending and descending start and end points and took measurements from the still images at 0/3, 1/3, 2/3 and 3/3 of the ascending and descending lift phases as detailed above. Intra-rater and inter-rater reliability were determined from these measurements using intraclass correlation coefficients (Table 2).
Reliability of joint angle measurements
Reliability of joint angle measurements
Demographics
Twenty eight subjects participated in this study. The sample consisted of 19 females and 9 males, with an age range of 18–22 (mean age 20.9). The mean maximum weight lifted for females and males was 10.54 kg (range 8.5–13) and 16.56 (range 12–23.2) respectively.
Reliability
Both intra-rater and inter-rater reliability measures for all joint angles were considered excellent [36], with ICCs of greater than 0.75 for all measures (Table 2).
Ascending segment of lift
The mean joint angles, confidence intervals and p-values of the ascending bench to shoulder lift for all participants are shown in Table 3. Key findings in the ascending phase were significant differences between the minimum and safe maximum lift in joint angles in the thoracic spine, elbow and shoulder. These were found in the thoracic spine at the point 3/3 (p = 0.004, mean difference 2.292), where the thoracic spine was in greater extension during the maximum lift (Fig. 3); in the elbow at points 1/3 (p = 0.008, mean difference 6.405) and 3/3 (p = 0.009, mean difference 15.575) where the elbow was in greater flexion during the maximum lift (Fig. 4), and in the shoulder at point 3/3 (p = 0.000, mean difference 16.785) where the shoulder was in less extension during the maximum lift (Fig. 5). The lumbar spine presented slight joint angle differences between the minimum and maximum lifts however none of these were statistically significantly different with mean differences at all points being <1° (Fig. 6).
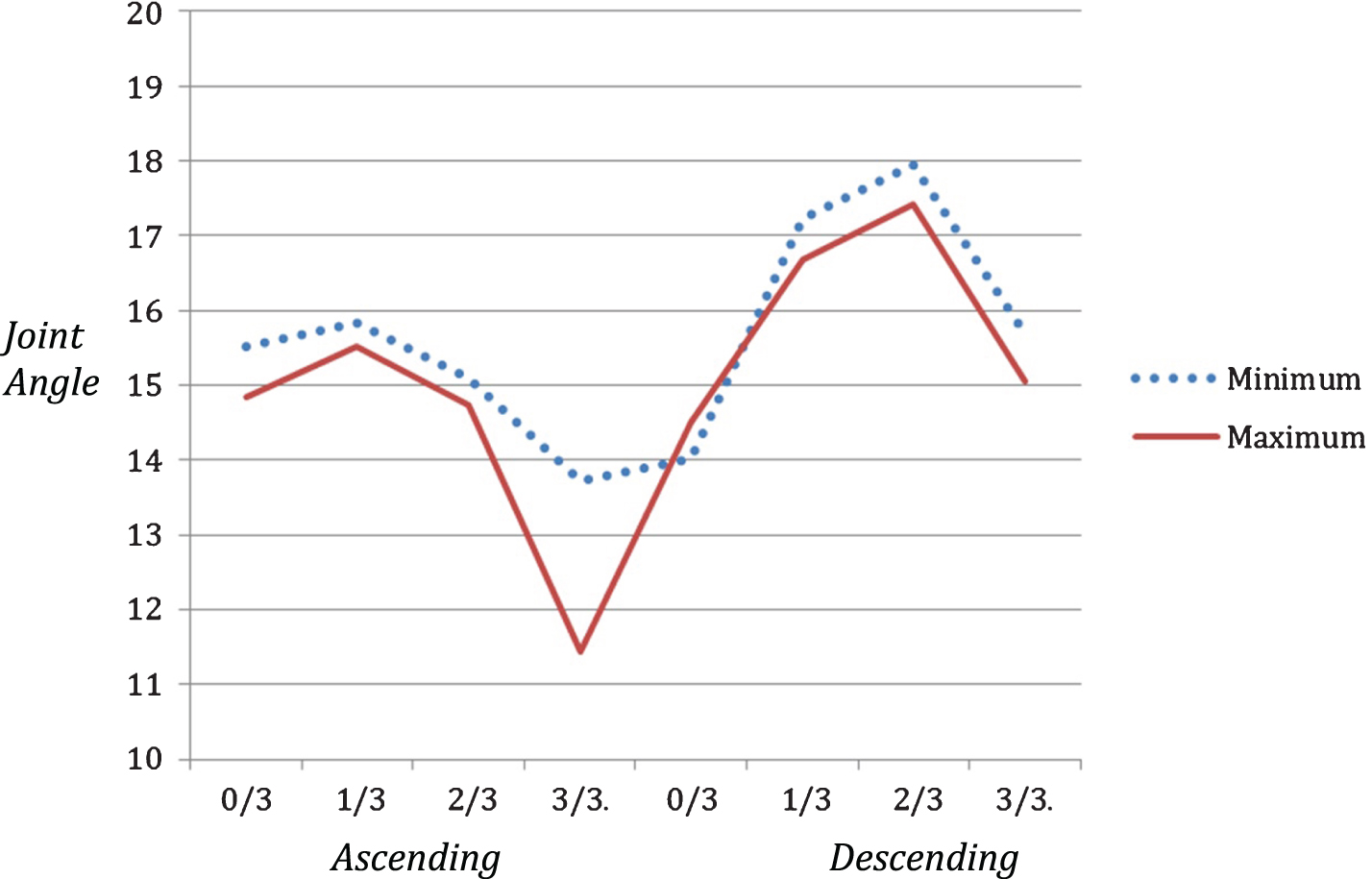
Thoracic Spine results.
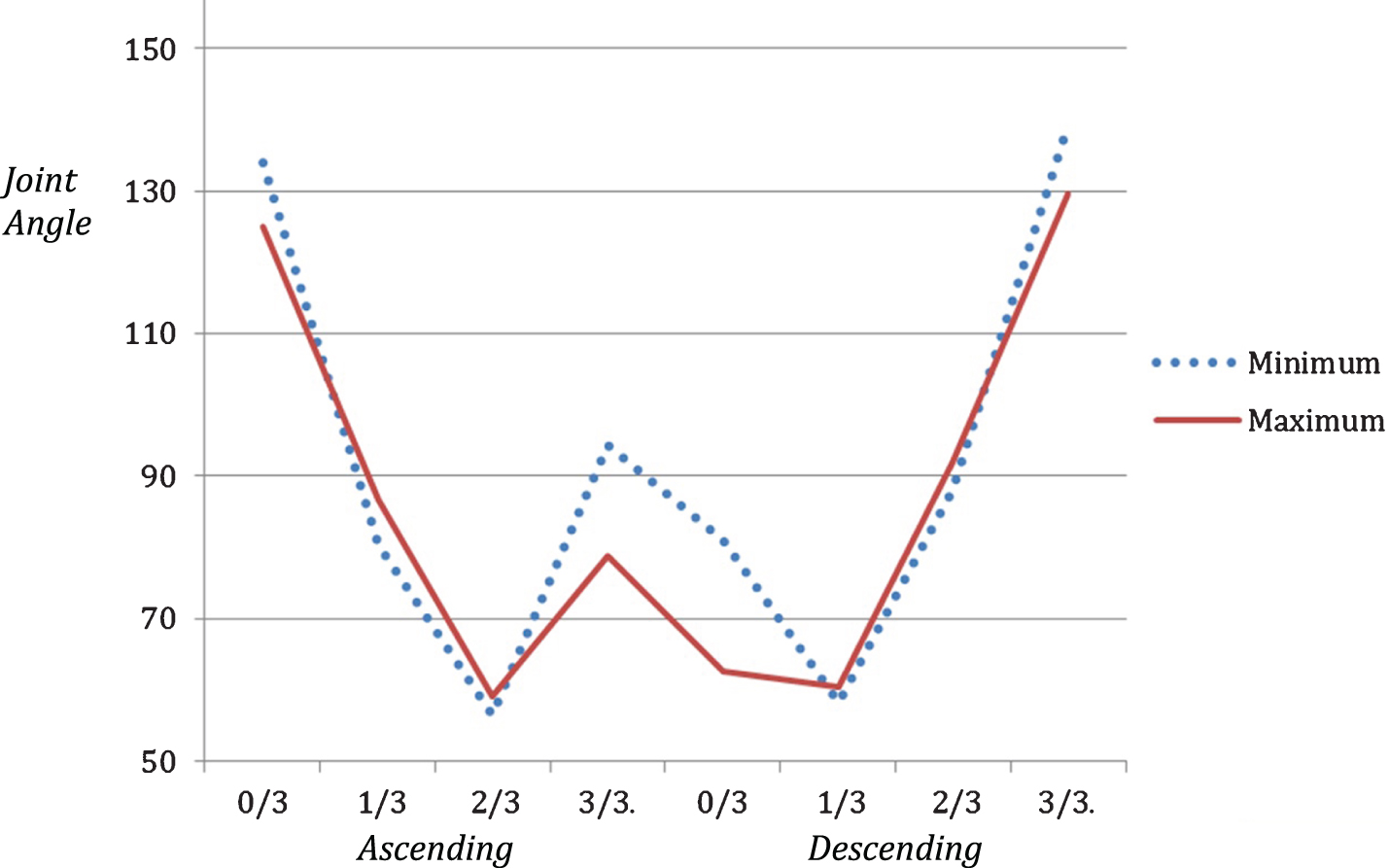
Elbow results.
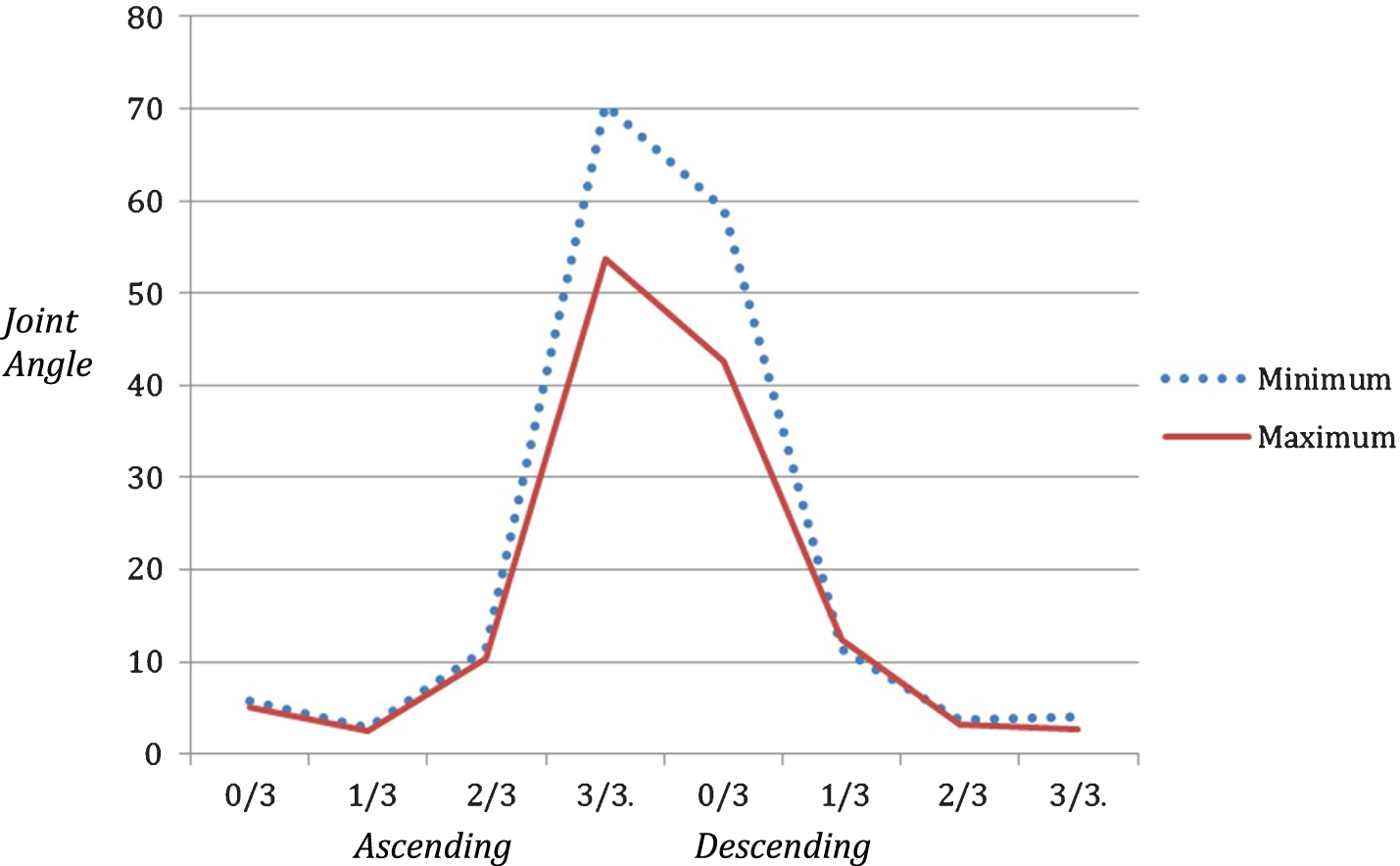
Shoulder results.

Lumbar Spine results.
Ascending lift results
In the descending segments of the bench to shoulder lift, three significant differences in joint angles between the minimum and safe maximum lift were observed (Table 4). These were found in the elbow at point 0/3 (p = 0.000, mean difference 18.446) and 3/3 (p = 0.035, mean difference 9.632) (Fig. 4), and in the shoulder at point 0/3 (p = 0.000, mean difference 16.647) (Fig. 5), where the joints were in greater flexion during the maximum lift. The lumbar and thoracic spine measurements produced slight joint angle differences between the minimum and maximum lifts however these had no statistical significance as mean differences at all points were <1.5°.
Descending lift results
Descending lift results
This analysis of healthy individuals completing a bench to shoulder lift during the manual handling component of the WorkHab FCE found there are significant differences in joint angles of the thoracic spine, elbow and shoulder when comparing the minimum and safe maximum lifts in both ascending and descending directions. This shows when load is placed on the body, it will compensate through biomechanical adjustment.
Elbow/shoulder
In the elbow joint, a significant difference at 1/3 of the ascending lift was identified where subject’s elbow joints were in less flexion during the maximum lift, shortly after the box is lifted from the bench. Research by Andersson and McLester shows that a 4 kg weight held at a distance of 50 centimeters from the body requires the same amount of muscle force as a 20 kg load kept close to the body, and that lifting a load at an arm’s length away causes a 10 times increase in the amount of force exerted on the spine [37, 38]. The safe maximum load (heavy) lifted during this study, caused the subject to keep the load low and close to the body for longer, prior to raising it to a higher surface. Significant differences were observed in the elbow (3/3 ascending, 0/3 descending) and in the shoulder (3/3 ascending, 0/3 descending). At these points the elbow and shoulder joints were in significantly greater flexion during the maximum lift. These are the highest points of both the ascending and descending lift, and occur shortly before the box is placed at shoulder height and shortly after the box is picked up from shoulder height respectively.
These results concur with a number of safe lifting guidelines that suggest the safest and most efficient way of moving a load is to keep it close to the body [39–42]. Heavy loads kept further away from the body require greater muscular force to lift [43]. By keeping loads close to the body, weight distribution becomes more even and large muscle groups are recruited [44]. This relates to FCE aims and highlights that through the use of correct manual handling techniques, muscle exertion and risk of injury can be significantly reduced. It also demonstrates that healthy people, without injury are naturally using safe lifting without prompting.
Lumbar
There was no significant difference in lumbar spine extension during the ascending or descending segment in the maximum lift when compared to the minimum lift, seen in Fig. 6. When lifting from a low to high surface (ascending), the force exerted on the lumbar spine is greater compared to beginning a lift at a high surface, as a result of an increased trunk angle putting strain on the posterior aspects of the spine [45]. In 2013, Rodriguez-Soto et al. investigated the effect of load on the lumbar spine and found that greater load increases superior lumbar spine lordosis (extension) [46]. Research shows that ligaments and muscles of the lumbar spine are strained when the lumbar spine is not in neutral lordosis [14]. Therefore, increased stability of the lumbar spine and neutral lordosis maintenance is required as load increases [47] in order to decrease risk of injury [48]. In the current study there was minimal change observed in lumbar extension which may have been the result of the specific style of lift conducted (bench to shoulder, as opposed to being from the floor).
Thoracic
Results from the current study indicate that the thoracic spine was in significantly greater extension (decreased kyphosis) at the highest point of the maximum ascending lift as opposed to the minimum ascending lift at the same point. As shown in Figs. 3–6, when the shoulder is in greater flexion and the elbow is in less flexion (the load is further away from the body), the thoracic spine is in greater extension suggesting that the muscles of the thoracic spine are under significantly more pressure. This is a result of the longer level at the shoulder joint being unable to produce the torque required. The thoracic spine shifts into extension, as a compensatory strategy, to allow the shoulder to stay at reduced range, and thus produce more force. This shift causes sheer, which can lead to injury [14]. The thoracic spine was also observed to be in slightly greater extension at point 0/3 (Fig. 3) of the maximum descending lift (mean difference 0.493), which is the highest point of the descending lift. It is interesting to note that significant differences in thoracic extension were noted during the ascending lift and at the highest point of the descending lift. This maybe related to the interactions between the lumbar and thoracic spine during a lift and the pattern of movement overall [49] and as the trunk compensates to keep postural stability [50]. Other than at these stages of the lift the thoracic spine was in less extension during the maximum lift, in both the ascending and descending components, as can be seen in Fig. 3.
Compared to the cervical and lumbar spine, the thoracic spine is considered to have a restricted range of motion in flexion and extension, caused by its spinous processes and attachment to the rib cage [51, 52], therefore significant joint angle change under load present a serious risk of injury [51]. The most common types of thoracic spine injuries occur in axial loading and are muscular irritation and costovertebral joint dysfunction [53, 54]. Ning, Zhou, Dai, and Jaridi studied trunk biomechanics and manual handling with sudden loading and found a higher load increased compression forces in the lumbar region of the spine and reduced the magnitude of trunk flexion [55]. This supports the findings in the current study, where the thoracic spine was at most risk when the lift is at its highest point as also noted by others [39, 42]. Keeping loads at lower heights when lifting is good practice and maybe a protective strategy, as recommended in safe lifting guidelines [41].
Clinical implications
The significant extension of the thoracic spine observed in this study is an important finding during a bench to shoulder lift, as the thoracic region of the spine has been linked to changes in movement patterns that impact upon spinal loading [49, 50], and is at risk of injury as lift mass increases [51]. There was no significant change in lumbar posture. The assessor observed biomechanical cues and ceased the assessment when a significant change in lifting posture and technique was observed [23, 56]. This research gives therapists more understanding of the expected change in joint angles in the minimum and safe maximum lifts during the bench to shoulder lift in an FCE. It also provides support and adds to the current literature regarding the biomechanical and joint angle change, which occurs as a result of load. This substantiates the clinical reasoning used, alongside biomechanical cues, by the assessor in determining the safe maximal lift during an FCE [24, 57]. The findings of this study, with changes in the thoracic, elbow and shoulder joints assists to validate the clinical reasoning and clinical judgements used by the assessor in determining a safe maximal lift during the bench to shoulder lift of the WorkHab FCE. As all FCE assessments include manual handling, the results of this study could be applied to other assessment tools and Functional Capacity Evaluations which utilize a bench to shoulder lift.
Limitations
This study used a small sample of healthy university students with no presenting biomechanical issues and an age range of 18–22, which is not indicative of the working population on which the FCEs would generally be carried out. The video data used for this study assumes symmetry with only the right sagittal view being used for data collection. Additional cameras on the left sagittal plane would have allowed a more thorough analysis of the joints particularly as rotation in the trunk obscured the foam markers from view in some images. This study used joint angle to investigate biomechanics however analysis of muscle force or muscle activity level would have provided greater depth to this analysis. It is also assumed that safe maximum lift was achieved for each participant.
Future research
Future research should investigate the manual handling component of the WorkHab FCE in workers prior to starting a job or returning to work after injury to better reflect the population usually assessed with FCEs. Research and assessment of biomechanics, posture and joint angles during dynamic lifting, rather than from static images, would also provide useful information to support clinicians in their determination of a safe maximal lift during an FCE. The addition of participant interviews to determine if they felt that they had reached their maximum effort would be advantageous. Biomechanical changes when objects of different dimensions are moved, with particular relevance to dynamic workplace lifting and it’s potential to cause injury should also be investigated.
Conclusion
This study showed that significant biomechanical differences occur in the elbow, shoulder and thoracic spine when lifting a light load compared to safe maximal load between bench and shoulder height as defined by the WorkHab FCE [29] The most significant differences were found with increased flexion in the elbow and shoulder in both the ascending and descending lift and the shoulder in the safe maximal lift. Additionally, the thoracic spine was in greater extension when a heavier load was being lifted, particularly at higher points. This study adds to the literature on the effect of load on lifting and be a useful reference point for clinicians administering the WorkHab or other FCEs.
Conflict of interest
None to report.