
Abstract
BACKGROUND:
Disability management (DM) is a systematic method to ensure job-retention and job-reintegration in competitive employment for individuals with a disability. There is evidence that ‘returning to work’ has a positive impact on the individual, the company and on the society. However, a clear overview of the efficacy and efficiency of the DM programs is scarce.
OBJECTIVE:
To systematically review the efficacy and efficiency of the disability management programs. Cochrane, PubMed, Google Scholar, and Web of Science were searched from 1994 to 2015.
METHODS:
Two reviewers independently evaluated the articles on title, abstract, and full text. The data extraction and results are documented according to the study designs.
RESULTS:
Twenty-eight articles were included in the review. These 28 articles consisted of 7 systematic reviews, 3 randomized controlled trials, 9 clinical trials, 4 mixed-method studies and 5 qualitative studies.
CONCLUSIONS:
The DM program has shown to be effective and efficient. A consensus about the DM components is still not reached. Nevertheless, some components are emphasized more than others; job accommodation, facilitation of transitional duty, communication between all stakeholders, health care provider advice, early intervention, and acceptance, goodwill and trust in the stakeholders, in the organization, and in the disability management process.
Introduction
Disability Management (DM) is defined as a systematic and constructive method associated with the bio-psycho-social model, a model originally defined by Engel in 1977 [1] and adopted by the World Health Organization (WHO) [2] to ensure job-retention and job-reintegration in competitive employment for individuals with a (temporary) disability. Individual needs, workplace conditions and legislation are taken into account during the program [3]. DM involves the compatibility of Human Resource Management (HRM) and health care providers (health care professional) [4]. It has emerged in Canada and North America in the 1940’s and consecutively introduced in different countries in Europe (Scandinavia, France, Germany, Austria, the Netherlands, Ireland, United Kingdom, Switzerland and Belgium) through conferences given by the ‘Rehabilitation Foundation of Helsinki’ [4]. In 1994 the Canadian National Institute of Disability and Research (NIDMAR) was founded and aimed expeditiously to spread and implement DM through education and research. In 2002 Russo and Innes summarized ten principles of DM (Fig. 1) according to NIDMAR obtained from different sources of Occupational Health & Safety Organizations [5]. These ten principles serve as basis to define DM according to NIDMAR. There is ample evidence that returning to work has a huge impact on the micro- (employee), meso- (company) and macro-level (society).

Principles of DM defined by Russo and Innes [5].
On the micro-level, returning to work promotes health, community integration and participation [6–8]. Additionally, there is strong evidence that work has a positive influence on quality of life (QoL), social status, occupational identity, provided that there is a good person-job fit [9]. This means a balance between challenge, flexibility and predictability and a job fitting with the values and the interests of aperson [10].
On the meso-level the company benefits by reducing costs of recruitment, selection and training, productivity loss, absenteeism, and losing qualities and skills by using DM [11]. In order to gain these advantages, the company needs an appropriate reintegration policy, which includes a quick reintegration to the workplace and a good person-organization fit is necessary. This implies a supportive and respectful environment, teamwork and transparent communication between all stakeholders involved in the reintegration process (e.g., members of the treating team, occupational physician, insurance physician, employer, employee,...) [10, 11].
On the macro-level. Firstly; DM could provide an answer to the current issues in our society; healthcare delivery is currently confronted with an emerging problem of chronic conditions which includes a growing group of patients with multi-morbidity and an increasing social gradient in health [12]. Moreover because of the increasing retirement age, immense challenges for DM arise [13]. A second issue is that some employers perceive people with a disability as less motivated to or interested in work. Therefore, motivation has been gaining more attention in the ‘return to work’ process [14]. There is however evidence that people with a disability have the same desires as other people and want to participate in society by means of having a job [10]. A third issue is that the attention to DM increases in companies because of the legislation.
The Universal Declaration of Human Rights of 1949 declares that everyone has right to work, to free choice of employment, to just and favorable conditions of work and to protection against unemployment [15] and is stull applicable in contemporary society. In 2000 a European directive reported that discrimination according to disability is prohibited. In many other countries, there is legislation that requests collaboration between individuals with work disabilities and their employers to ensure early and safe return to appropriate work (e.g. Canada’s Workplace Safety and Insurance Act, Dutch Gate Keeper Law, or New Zealand’s Injury Prevention, Rehabilitation, and Compensation Act) [16].
The described literature above shows that ‘return to work’ (return to work) has a positive impact on the person, the company and on society. However, a clear overview of the efficacy and efficiency of the DM programs is lacking. Therefore, this study aims to systematically review the efficacy and efficiency, and the successful components of the DM programs, which are intended for people with a competitive employment who have an occupationaldisability.
Search strategy
The literature review comprised a systematic search in the Cochrane library, PubMed, Google Scholar and Web of Science for articles that included information about the efficacy and efficiency of DM for people with a disability according to the method described by NIDMAR. Therefore, the PICO method was used: (P) Participant: job retention or job reintegration for people with a competitive employment who have an occupational disability; (I) Intervention: DM as described by NIDMAR; (C) Comparison: no intervention or no comparison and (O) Outcome: efficacy and/or efficiency and the successful components of DM programs. The search terms were based on different sources and took the scope of this review into account [9, 17]. If the search engine allowed it, different eligibility criteria were used. These included year published (1994–2016), language (Dutch-French-English), publication type (trials, systematic review, meta-analysis). The year 1994 was chosen as a lower limit because it is the starting year of NIDMAR. When necessary the search-string was adapted to the constraints of the databases (see Table 1 for the complete search-string and limits). Other strategies to ensure identification of all potentially relevant articles and original papers included scanning the reference lists of all initially included systematic reviews (SR), randomized controlled trials (RCT), clinical trials (CT), mixed methods studies (MM) and qualitative studies (QS), and If articles were not available in full access online, authors were contacted. The review protocol of this study is written in Dutch and is available on request.
Complete search-string and limitations in each database
Complete search-string and limitations in each database
1((disability management AND effectivity) OR (disability management AND efficiency) OR (disability management AND advantages) OR (disability management AND limitations) OR (disability management AND barriers) OR (disability management AND implementation) OR (disability case manager AND effectivity) OR (disability case manager AND efficiency) OR (disability case manager AND advantages) OR (disability case manager AND limitations) OR (disability case manager AND barriers) OR (disability case manager AND implementation) OR (vocational rehabilitation AND effectivity) OR (vocational rehabilitation AND efficiency) OR (vocational rehabilitation AND advantages) OR (vocational rehabilitation AND limitations) OR (vocational rehabilitation AND barriers) OR (vocational rehabilitation AND implementation) OR (return to work AND effectivity) OR (return to work AND efficiency) OR (return to work AND advantages) OR (return to work AND limitations) OR (return to work AND barriers) OR (return to work AND implementation) OR (absenteeism AND effectivity) OR (absenteeism AND efficiency) OR (absenteeism AND advantages) OR (absenteeism AND limitations) OR (absenteeism AND barriers) OR (absenteeism AND implementation) OR (presenteeism’ AND effectivity) OR (presenteeism’ AND efficiency) OR (presenteeism’ AND advantages) OR (presenteeism’ AND limitations) OR (presenteeism’ AND barriers) OR (presenteeism’ AND implementation) OR (job reintegration AND effectivity) OR (job reintegration AND efficiency) OR (job reintegration AND advantages) OR (job reintegration AND limitations) OR (job reintegration AND barriers) OR (job reintegration AND implementation) OR (job retention AND effectivity) OR (job retention AND efficiency) OR (job retention AND advantages) OR (job retention AND limitations) OR (job retention AND barriers) OR (job retention AND implementation) OR (work capacity AND effectivity) OR (work capacity AND efficiency) OR (work capacity AND advantages) OR (work capacity AND limitations) OR (work capacity AND barriers) OR (work capacity AND implementation) OR (work disability AND effectivity) OR (work disability AND efficiency) OR (work disability AND advantages) OR (work disability AND limitations) OR (work disability AND barriers) OR (work disability AND implementation) OR (occupational health AND effectivity) OR (occupational health AND efficiency) OR (occupational health AND advantages) OR (occupational health AND limitations) OR (occupational health AND barriers) OR (occupational health AND implementation) OR (sick leave AND effectivity) OR (sick leave AND efficiency) OR (sick leave AND advantages) OR (sick leave AND limitations) OR (sick leave AND barriers) OR (sick leave AND implementation) OR (employment status AND effectivity) OR (employment status AND efficiency) OR (employment status AND advantages) OR (employment status AND limitations) OR (employment status AND barriers) OR (employment status AND implementation) OR (work status AND effectivity) OR (work status AND efficiency) OR (work status AND advantages) OR (work status AND limitations) OR (work status AND barriers) OR (work status AND implementation) OR (occupational rehabilitation AND effectivity) OR (occupational rehabilitation AND efficiency) OR (occupational rehabilitation AND advantages) OR (occupational rehabilitation AND limitations) OR (occupational rehabilitation AND barriers) OR (occupational rehabilitation AND implementation) OR (case management AND effectivity) OR (case management AND efficiency) OR (case management AND advantages) OR (case management AND limitations) OR (case management AND barriers) OR (case management AND implementation) OR (case manager AND effectivity) OR (case manager AND efficiency) OR (case manager AND advantages) OR (case manager AND limitations) OR (case manager AND barriers) OR (case manager AND implementation)).
2The search in Google Scholar was done in two times because of limited space:. First search string: (disability management OR disability case manager OR vocational rehabilitation OR return to work OR absenteeism OR presenteeism OR job reintegration OR job retention OR work capacity OR work disability OR occupational health OR sick leave). Second search string: (employment status OR work status OR occupational rehabilitation OR case management OR case manager). 3(disability management OR disability case manager OR vocational rehabilitation OR return to work OR absenteeism OR presenteeism OR job reintegration OR job retention OR work capacity OR work disability OR occupational health OR sick leave) Refined by: [excluding] WEB OF SCIENCE CATEGORIES: (CHEMISTRY ANALYTICAL OR CLINICAL NEUROLOGY OR EDUCATION SPECIAL OR OTORHINOLARYNGOLOGY OR BIOPHYSICS OR BIOTECHNOLOGY APPLIED MICROBIOLOGY OR CHEMISTRY MEDICINAL OR CRITICAL CARE MEDICINE OR GERONTOLOGY OR PHARMACOLOGY PHARMACY OR DENTISTRY ORAL SURGERY MEDICINE OR ENVIRONMENTAL SCIENCES OR TOXICOLOGY OR CHEMISTRY MULTIDISCIPLINARY OR OPERATIONS RESEARCH MANAGEMENT SCIENCE OR SPORT SCIENCES OR NUTRITION DIETETICS OR LINGUISTICS OR CHEMISTRY PHYSICAL OR BIOCHEMICAL RESEARCH METHODS OR PEDIATRICS OR OBSTETRICS GYNECOLOGY OR OPHTHALMOLOGY OR EMERGENCY MEDICINE OR BIOCHEMISTRY MOLECULAR BIOLOGY OR VETERINARY SCIENCES OR SURGERY OR ENGINEERING BIOMEDICAL OR WATER RESOURCES OR NANOSCIENCE NANOTECHNOLOGY OR RADIOLOGY NUCLEAR MEDICINE MEDICAL IMAGING OR ECOLOGY OR ENGINEERING ENVIRONMENTAL OR ENERGY FUELS OR ANTHROPOLOGY OR TROPICAL MEDICINE OR ENGINEERING CHEMICAL OR MICROBIOLOGY OR PARASITOLOGY OR FOOD SCIENCE TECHNOLOGY OR ZOOLOGY OR GERIATRICS GERONTOLOGY OR ENGINEERING CIVIL OR PLANT SCIENCES OR CELL BIOLOGY OR ENGINEERING INDUSTRIAL OR GEOSCIENCES MULTIDISCIPLINARY OR ANESTHESIOLOGY OR EDUCATION EDUCATIONAL RESEARCH OR ENDOCRINOLOGY METABOLISM) AND [excluding] DOCUMENT TYPES: (BOOK CHAPTER) AND [excluding] RESEARCH AREAS: (ENDOCRINOLOGY METABOLISM OR PUBLIC ADMINISTRATION OR EDUCATION EDUCATIONAL RESEARCH OR COMPUTER SCIENCE OR MINING MINERAL PROCESSING OR MATHEMATICAL METHODS IN SOCIAL SCIENCES OR GEOGRAPHY OR MATHEMATICAL COMPUTATIONAL BIOLOGY OR FISHERIES OR GEOCHEMISTRY GEOPHYSICS OR DEVELOPMENTAL BIOLOGY OR CRIMINOLOGY PENOLOGY OR SPECTROSCOPY OR ENVIRONMENTAL SCIENCES ECOLOGY OR ENTOMOLOGY OR MATHEMATICS OR CELL BIOLOGY OR INTEGRATIVE COMPLEMENTARY MEDICINE OR REPRODUCTIVE BIOLOGY OR CHEMISTRY OR PHILOSOPHY OR HISTORY OR MARINE FRESHWATER BIOLOGY OR OCEANOGRAPHY OR HISTORY PHILOSOPHY OF SCIENCE OR FORESTRY OR TRANSPLANTATION OR NUCLEAR SCIENCE TECHNOLOGY OR INFORMATION SCIENCE LIBRARY SCIENCE OR MEDICAL LABORATORY TECHNOLOGY OR LITERATURE OR ARCHAEOLOGY OR TELECOMMUNICATIONS OR RELIGION OR MUSIC OR SCIENCE TECHNOLOGY OTHER TOPICS OR POLYMER SCIENCE OR METEOROLOGY ATMOSPHERIC SCIENCES OR LIFE SCIENCES BIOMEDICINE OTHER TOPICS OR ASTRONOMY ASTROPHYSICS OR ELECTROCHEMISTRY OR VIROLOGY OR URBAN STUDIES OR GENETICS HEREDITY OR TRANSPORTATION OR ENGINEERING OR THERMODYNAMICS OR ZOOLOGY OR AGRICULTURE OR MINERALOGY OR MYCOLOGY OR MATERIALS SCIENCE OR METALLURGY METALLURGICAL ENGINEERING OR GEOLOGY OR MEDICAL INFORMATICS OR ARTS HUMANITIES OTHER TOPICS) AND [excluding] Book Series Titles: (PROGRESS IN BRAIN RESEARCH OR INTERNATIONAL REVIEW OF NEUROBIOLOGY OR ANNUAL REVIEW OF POLITICAL SCIENCE).
Two researchers (the first two authors) independently evaluated the eligibility of the articles. To do so, articles were first selected based on the title and in a second step based on the content of the abstract. At both stages, articles considered eligible (Fig. 2) by one or both of the researchers were included in the next stage. Duplicates were removed after screening the abstracts.

Eligibility criteria for inclusion.
Finally, the first (ML) and the second author (SD) selected all eligible articles by scanning the full texts on content, using the ten principles of DM defined by Russo and Innes [5] (Fig. 1) and on the method. Four possible categories for selection on content were developed: (1) “clearly not DM”, (2) “no clear intervention described”, (3) “yes, clearly DM” and (4) “some components of DM are described”.If reviewers did not agree whether the article belonged in the category “yes, clearly DM”, consensus was reached through discussion. Other categories were all downgraded to “clearly not DM”. Only SR, RCT, QS, MM and CT which scored “yes, clearly DM” were included in the review. The test for homogeneity between both reviewers has been done by kappa statistical test.
The quality appraisal was done by using the appropriate checklists depending on the design of the article: PRISMA (Systematic Reviews), CONSORT (Randomized Controlled Trials), TREND (Non-Randomized Trails), CASP (Qualitative research), STROBE (observational studies) and NIH (before after studies with no control group). Articles were scored good, moderate and poor according to the guidelines of the different checklists. If no guidelines were present, the following rationale was used: if all items which prevailed were good (e.g. sample size, population, outcome measures, allocation...) the quality was considered good. Articles were scored as moderate if one or two of the items were fulfilled or poorly described. Articles were scored as poor if more than two of the items were not fulfilled or poorly described.
Data extraction and analysis
A data extraction tool was developed, based on existing forms [11, 18–23]. The tool included country, study design, objectives, sample characteristics, inclusion period and follow-up period, primary and secondary outcomes, statistical analysis and summary measures, intervention, components of DM based on Russo and Innes [5] and the conclusion. Through different levels the tool was refined to capture all important elements of the study concerning DM. One reviewer (ML) extracted the data. A second reviewer (SD) reconsidered the results and made readjustments where necessary. If there was any disagreement in this stage, consensus was reached through discussion between the two reviewers (ML and SD). The fourth and the fifth reviewers (LB and DVdV) were consulted if the disagreements persisted. They also examined and approved the final results.
Results
Search strategy and selection process
After selecting the eligible titles, 908 abstracts were screened and 27 duplicates were removed. A total of 255 full texts were retrieved, of which 10 full texts could not be screened, as they were not available, even after contacting the authors. At the content level 39 full texts were retained. Kappa statistical test for all four categories (“clearly not DM”, “no clear intervention described”, “yes, clearly DM”, and “some components of DM are described”) was 0.75, and for the two categories (“yes clearly DM” or one of the other categories downgraded to “clearly not DM”) 0.87. Of these full texts 17 were dropped due to the method used (9 were theoretical papers, 8 were grey literature). By screening the reference lists of the 22 remaining full texts, 6 new articles were added. In the end, 28 articles were included, of which 7 SR’s, 3 RCT’s, 9 CT’s, 4 MM’s and 5 QS’s. (See Fig. 3).
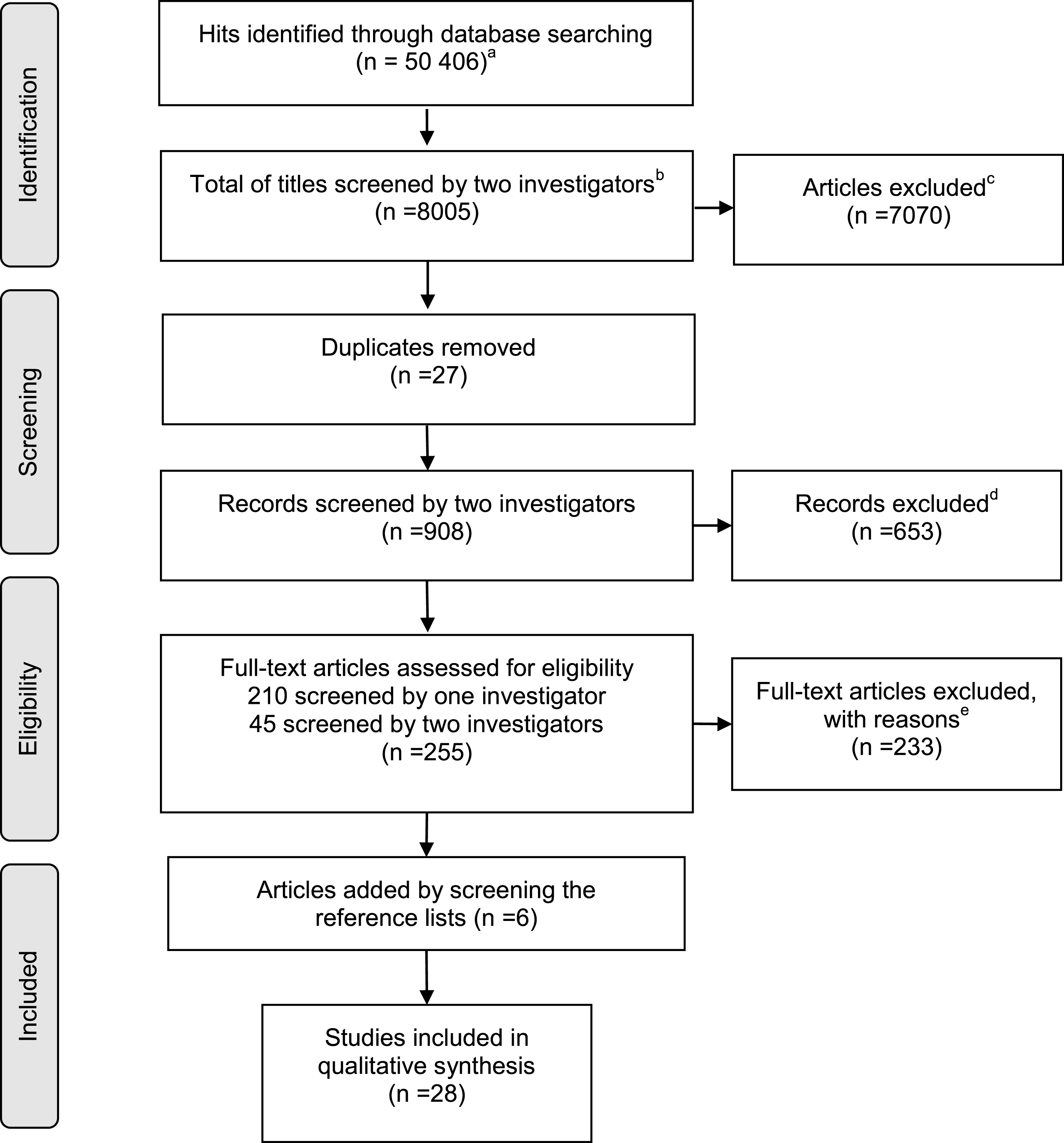
Flowchart of search and selection strategy. aOne article was obtained extra through searching in function of articles for the introduction. bOnly the first 2000 of Google Scholar total (n = 44 400) were screened. Other databases were PubMed (n = 1804), Cochrane (n = 105) and Web of Science (n = 4096). cWhen articles were screened on the basis of title, they are included when the raters have the idea the article is original research about Disability Management. When in doubt the article was selected. dReasons for exclusion: on the basis of the abstract, the raters decided the article was not original research (n = 30) or the study was not containing information about Disability Management (n = 616) or the study did not have an abstract (n = 8). eIn depth reading of the full text of the articles revealed that the article was not containing any or too few components of Disability Management (n = 205) or the method of the article was below level 4 of evidence (n = 17) or the article was not retrieved after searching the internet and contacting the authors (n = 10).
Nine articles have a good quality [12, 42], thirteen have a moderate quality [18, 44] and five have a low quality [20, 43]. None of the articles were excluded based on the quality check.
Data extraction and analysis
The data extraction of the included articles is illustrated in Table 2 (SR’s), Table 3 (RCT’s), Table 4 (CT’s & MM’s), Table 5 (QS’ss), except for one article which only studied the reliability and the validity of a questionnaire used in this area. All results, both significant and not significant, were analyzed and included. Below a summary is given of the conclusions of the different studies.
Overview of the selected systematic reviews
Overview of the selected systematic reviews
1In case of SR inclusion period of studies and suggested FU period. 2Components of DM: (1) Early intervention; (2) Engagement of all stakeholders involved in the process; (3) Primary goal is jobretention or jobreintegration conform to the individual needs and demands of the job; (4) Recognition of the workplace to be most effective place for reintegration. (5) Retain the dignity of the employees and ensure an active participation during the reintegration process; (6) Consultation and communication between all stakeholders in all stages of the process; (7) Return to work on the highest level possible, with attention to the following hierarchy: Same tasks/same job, same employer; Modified tasks/similar job, same employer; Alternative tasks/new job, same employer; Same tasks/same job, other employer; Modified tasks/similar job, other employer; Alternative tasks/new job, other employer; (8) Assignment of meaningful tasks to the concerned employee; (9) Consideration to graduate the return to work in terms of tasks or time; (10) Individual reintegration associated to workplace-based occupational health and safety programs. The CRTWC monitors and stimulates the clarification of the situation, the cooperation and reciprocity between all stakeholders, according to the legislation on reintegration, to accomplish an early integration of the employee. 3Measures of general health, condition-specific functional status, symptom severity, and pain levels. 4Planned intervention program, typically offered in a limited number of workplaces, by the same team of providers, often as part of a research study. Their evaluation was typically planned prior to implementation of the program. 5Strategies were approaches to improve RTW outcomes, which did not necessarily occur as part of a planned intervention program. These were typically examined in observational studies. Their evaluation was often initiated after implementation.
6Health care, manufacturing and warehousing, mining and oil and gas extraction, multi-sector, and utilities. 7Partial interventions: consideration of only the monetary value of outcomes/consequences rather than consideration of both intervention costs and outcomes. Complete interventions: consideration of both costs and outcomes/consequences.
8A period of absence from the first day of sick leave to full RTW in previous or equal work for at least 4 weeks without dropping out. 9A period of absence from work because of sickness both preceded and followed by a period of at least one day at work. 10Total days of sick leave during the FU period (resulting from one or more periods of absence). 11The number of days until a recurrence; or the frequency and duration of recurrent episodes of sick leave. 12Functional status, QOL, general health, symptoms, pain. 13Inability to work due to an acquired physical injury, MHD or other illness resulting in functional work limitations and SA. 14RTW at any time or any kind of PT or FT work. 15Periods of SA followed by RTW. 16Defined cumulatively as the duration of all days lost from work beginning with the date of injury. 17How an employee’s health affects work role functioning and work ability. 18The number of days until recurrence or duration of recurrent episodes of SA. 19Cochrane Handbook for systematic reviews of interventions.
Overview of the selected Randomised Controlled Trials
20In case of Randomized controlled trial period of inclusion of patients and/or year of conduction. 21Components of DM: (1) Early intervention; (2) Engagement of all stakeholders involved in the process; (3) Primary goal is jobretention or jobreintegration conform to the individual needs and demands of the job; (4) Recognition of the workplace to be most effective place for reintegration. (5) Retain the dignity of the employees and ensure an active participation during the reintegration process; (6) Consultation and communication between all stakeholders in all stages of the process; (7) Return to work on the highest level possible, with attention to the following hierarchy: Same tasks/same job, same employer; Modified tasks/similar job, same employer; Alternative tasks/new job, same employer; Same tasks/same job, other employer; Modified tasks/similar job, other employer; Alternative tasks/new job, other employer; (8) Assignment of meaningful tasks to the concerned employee; (9) Consideration to graduate the return to work in terms of tasks or time; (10) Individual reintegration associated to workplace-based occupational health and safety programs. The CRTWC monitors and stimulates the clarification of the situation, the cooperation and reciprocity between all stakeholders, according to the legislation on reintegration, to accomplish an early integration of the employee. 22The interview focused on the person’s social and occupational situation, education, ongoing or previous rehabilitation experiences, professional career, their current employer, working hours, travel time to and from work as well as traveling arrangement to and from work, work habits, work postures, and physical work load, ergonomic equipment at work, and psychosocial work characteristics. Functional capacity, work demands, work capacity and work duties that a person could perform despite their current MSDs, as well as how their health impacted on their life in general were also discussed. 23The training schedule included information on type of training and work tasks adapted to the employee’s capacity, time allotted for each training session, weeks of training, and a schedule for the successive increase in workload. The ergonomist instructed the participant once or, when necessary, more times directly at work. 24This means 6.8 USD benefits for every 1 USD in costs.
25Design a back pain management program based on evidence, available to a population of workers, compatible with provincial law, and linking clinical and occupational interventions. 26Develop and assess a new program that would directly address the possible causes of disability for every worker at the subacute or early chronic stage, and that could be implemented in the Quebec based on the Sherbrooke model experience. 27Visit to the OP, where he could recommend investigation or treatment, or could try to set up light duties to help the worker to return to regular work. And implementation of a participatory ergonomics intervention (i.e. a work-site evaluation that included union and employer representatives) conducted by an ergonomist from work. The recommendations were submitted to the employer, and the implementation remained his/hers responsibility. 28Visit to a medical specialist to exclude a serious or very specific disease. And prescription for a back school for the 4 following weeks. 29FRT is described as fitness development and work conditioning with a cognitive-behavioral approach, carried out by a multidisciplinary team at the back pain clinic, with the aim to develop the worker’s global functional capacities. 30TRW is a progressive return to the worker’s regular work, alternating days on the job with progressively increased tasks and days in the clinical setting. 31Identify the precise causes of disability (physical, psychosocial, occupational and administrative) in each worker’s case. Work disability diagnosis interview (WoDDI) including a medical questionnaire and physical examination for back pain, work history, work demands, job difficulty, life habits, family and social history, perception on RTW, and worker’s financial situation is administered by a GP for the medical and psychological dimension, and by an occupational therapist for its occupational part 32When the physician and the OT meet after the WoDDI they share their findings and design an intervention plan that is then recommended to the worker, the attending physician, and the WCB caseworker. The TRW is tailored to the worker’s precise needs, identified through the WoDDI, and extends to the complete return to regular work or permanently modified work. *All remaining significant values are <0.001.
33The interdisciplinary team includes a GP (with skills in musculoskeletal disorders and the rehabilitation process), an OT, a physical educator (kinesiologist), a psychologist, an ergonomist, and a team coordinator who ensures the smooth functioning of the team with respect to values, purpose, and performance. A back pain specialist is available when needed, for consultation and reassurance of the team and the worker, especially in case of symptom augmentation during the rehabilitation. The whole team reaches a consensus on graded treatment and RTW, on messages to deliver to the worker, and on communication strategy with stakeholders. The team members meet every week to review ongoing cases, have a common objective on RTW, are mutually accountable, and can put aside interpersonal and interprofessional barriers to attain greater effectiveness in their action. 34Duration of sick leave in calendar days from the first day of sick leave to full RTW in own or equal work, for at least 4 weeks without (partial or full) dropout.
Overview of the selected Clinical Trials (including 3 Cohort Studies, 1 Quasi-Experimental Design, 2 Before After Studies, and 2 Cross-Sectional studies)
35In case of, clinical trials period of inclusion of patients and/or year of conduction. 36Components of DM: (1) Early intervention; (2) Engagement of all stakeholders involved in the process; (3) Primary goal is jobretention or jobreintegration conform to the individual needs and demands of the job; (4) Recognition of the workplace to be most effective place for reintegration. (5) Retain the dignity of the employees and ensure an active participation during the reintegration process; (6) Consultation and communication between all stakeholders in all stages of the process; (7) Return to work on the highest level possible, with attention to the following hierarchy: Same tasks/same job, same employer; Modified tasks/similar job, same employer; Alternative tasks/new job, same employer; Same tasks/same job, other employer; Modified tasks/similar job, other employer; Alternative tasks/new job, other employer; (8) Assignment of meaningful tasks to the concerned employee; (9) Consideration to graduate the return to work in terms of tasks or time; (10) Individual reintegration associated to workplace-based occupational health and safety programs. The CRTWC monitors and stimulates the clarification of the situation, the cooperation and reciprocity between all stakeholders, according to the legislation on reintegration, to accomplish an early integration of the employee. 37The CM identified and selected cases for review from the plant hourly disability leaves listing. A CM work sheet was completed on each claim and included all available background information and pertinent data regarding the employee’s disability. Multiple information sources were accessed, including the disability information system, the national benefit center, the workers’ compensation section, and the extended disability benefits compensation office, along with employee plant medical records. Information was also received from attending physicians, specialists, consultants, and ancillary HCPs. Data were entered into a Disability Claim Tracking System. 38Work Readiness Center is a center that designs and tracks progress through transitional work programs. 39The plant DM team consisted of the CM, the job placement coordinator, the medical director, and the nursing supervisor. Other disciplines were involved on an as-needed basis and included employment, labor relations, the union, workers’ compensation, manufacturing, and the employee assistance program. 40On a weekly basis the CM presented selected cases to the DM team for review and disposition. On each new or continued case, the objective was to “bring the case to closure.” Information was compiled on job availability, transitional job assignments in the WRC, non-traditional jobs, workstation and tooling design, and accommodations needed to make available jobs more appropriate to the functional capacities of the injured or ill workers. If special accommodations were needed, the CM contacted the job placement coordinator to request a job search and analysis. When indicated, independent medical examinations were scheduled to determine the employee’s fitness for duty. 41Productivity and job retention in light of ongoing medical recovery were critical to successful RTW. The CM and job placement coordinator closely monitored the employee’s progress and performance to ensure that the employee was allowed adequate time to become acclimated to the job, that necessary job modifications and accommodations had been implemented, that required tools were satisfactory, and that the employee was functioning at his or her peak capacity in a productive job. 42No further explanation by the authors.
43This database mainly includes employees’ claims for inpatient and outpatient health services, disability and workers’ compensation benefits, wellness program participation, medical examinations and laboratory tests, use of prescription drugs, and results of Health Risk Appraisals. 44First Chicago NBD Corporation, merged in 1998 with Banc One to form Bank One Company, employs 35,000 workers. Workers are scattered among approximately 700 individual worksites that range in size from 10 to over 8000 employees. 45A specially trained occupational health nurse. 46The packet is sent through mail to the employee’s home. The packet contains detailed information about the STD Benefits Program, instructions for steps the employee is required to take to receive benefits, and a short form to be filled out by the employee’s personal HCP and returned to the medical unit within 10 calendar days of the date of mailing. 47Before such action is taken, however, clarification is sought by requesting additional written reports from the employee’s physician or by a telephone discussion between the MDC and/or the Medical Director and the employee or health care provider. If doubt persists, the employee may be referred to an appropriate specialist for an independent evaluation at the employer’s expense. 48Comprises health education, disease management, health promotion activities, individual counseling, health risk assessment, periodic medical examinations, first aid training, and immunizations. 49Comprises worksite obstetrical and gynecological consultations, preconception and prenatal education, breast-feeding program, and mammography. 50An EAP to provide consultation, counseling, referral, and FU for a broad range of personal problems such as emotional and psychiatric disorders, interpersonal conflicts, alcohol and/or drug dependency, and other addictive disorders. 51Includes: prevention and early intervention programs, review of the worker’s need for inpatient psychiatric care, CM of mental health-related STD, and establishment of a network of MH professionals to provide outpatient (ambulatory) services for the self-insured indemnity plan.
52Absent as a result of unscheduled issues or disability claims. 53An Internet-based customer satisfaction survey was designed to address 3 key areas: program communication, DMP processes, and CM activities. 54Key stakeholders are the employee, the supervisor, the employee’s physician, Shell Health Services, Human Resources, Benefits, and Legal. 55Their RTW experience, duration of work absence, workplace, HCP, insurer, as well as their physical and mental health. 56Time receiving wage replacement benefits and claim status.
57Industrial sector, occupational classification, firm size of injury workplace, based on the number of FT workers, claim type and status 30 days after injury date was extracted from the WSIB administrative database. Age, gender, marital status, children and grandchildren, level of education, annual personal income, size of the worksite and unionization status, presence of comorbidities, pregnancy status, functional status, psychophysical demands of the job, job satisfaction, job security, employment status at the time of the injury, perceived pain level, depressive risk was self-reported or assessed. ∗All remaining significant values are <0.001.
58No further explanations by the authors. 59Self reported stress without severe MHD, no drug or alcohol abuse. 60The number of weeks from index day to full return to work or transfer from public health-related benefits to labour-market-related benefits. 61The assessment must be based on updated medical, social, and vocational information, and it should take place in cooperation with the sick-listed worker, the employer, medical experts, VR institutions, and other relevant agents. 62To promote a swift RTW, the municipal social worker can initiate various VR measures and vocational services. These measures include reduced working hours with supplementary sickness benefits, financial support for workplace adaptations and aids, testing of work ability, job counseling, wage-subsidized job training, and educational measures. 63Employers are only responsible for the financing of sickness benefits for the first two weeks of a sick leave period, while sick leave exceeding 2 weeks and disability benefits are financed by public authorities. Workers can normally receive sickness benefits for up to 12 months within a period of 18 months. 64The GP is the key figure for patients and he/she is responsible for health care initiatives e.g. referral to hospital treatment or other specialized treatments. GPs are often involved early during their patient’s sick leave absence, but they are not legally required to be involved. 65E.g. on decisions concerning resumption of work, support to families, participation in meetings with the workplace. 66Directed towards activating and supporting the patients efforts to adopt a problem-solving approach to their problems. 67Consisted of advice and support to patients, e.g. concerning legal matters, e.g. with reduced work hours in an initial period.
68Days of absence (limited to absences of 4 days to 1 year’s duration, and counted in the calendar year during which the absence ended) divided by number of absences per year. 69Days of absence (limited to absences of 4 days to 1 year’s duration, and counted in the calendar year during which the absence ended) divided by person-years worked during the calendar year. 70Based on the ICD9-CM the DC was calculated based on a single underlying cause per absence, again limited to absences between 4 and 365 days duration, and counted toward the absence end year, either 2002 or 2008. Total days saved per DC were calculated by multiplying the number of absence episodes in 2008 from that DC by the difference in the mean length of absence between 2002 and 2008. 71Direct costs were based on an average hourly wage of $32 (for both staff and hourly employees), and calculated by multiplying this hourly rate by the number of absence hours for the calendar year. For these calculations only, hours of absence included those occurring in the calendar year, regardless of whether the absence began or ended in that year. 72Particularly for employees who have missed 80 hours or more, are returning with restrictions, have had surgery, or are on medication, which might impact their ability to work in a safety-sensitive position.
73More than 8 weeks, but no longer than 6 months. 74Perceived health, well-being, SE, emotional exhaustion, feelings of depression, life events. 75Job stress, stress, work ability, work centrality (how important work is in one’s life). 76Experience during the period of absence.
77At baseline questionnaire on socio-demographics, health, functioning, work ability, SE, social support, work conditions, and expectations. And at 3 months FU questionnaire on patients’ self-reported measures of RTW, work ability and type of interventions. 78Sociodemographic variables (age, sex, marital status, and educational level), degree of sick leave, private economic issues, expectations and SE, social support, health, functioning and work ability, and work conditions. The patient’s educational level was categorized into two groups, lower education and higher education (university degree). The degree of sick leave was categorized as full-time or part-time and worries about private economic status as “yes” or “no”. 79Expectations of RTW were measured by asking the question “In your estimation, what are the chances that you will be working in 6 months?” This question was rated on a 5-point scale, where 1 was “very good chance” and 5 was “very little chance”. SE was measured by using the SE Scale (SES). 80Social support was measured using the Orth-Gomér instrument, Availability of Social Integration Index (AVSI), dealing with social support from family and close friends. 81Health-related quality of life was measured using EuroQoL-5D (EQ-5D). Mental functioning was measured using the Shirom Melamed Burnout Questionnaire (SMBQ). Physical functioning and pain in the musculoskeletal system were measured using the Functional Rating Index (FRI). Work ability was measured using the question “current work ability compared with the lifetime best” from the Work Ability Index (WAI). 82Work conditions were measured with the Effort– Reward Imbalance scale (ERI). 83Self-reported work ability was FU using the single-item question concerning the WAI item “current work ability compared with the lifetime best”.
Overview of selected mixed-method studies
84In case of mix-method studies period of inclusion of patients and/or year of conduction. 85Components of DM: (1) Early intervention; (2) Engagement of all stakeholders involved in the process; (3) Primary goal is jobretention or jobreintegration conform to the individual needs and demands of the job; (4) Recognition of the workplace to be most effective place for reintegration. (5) Retain the dignity of the employees and ensure an active participation during the reintegration process; (6) Consultation and communication between all stakeholders in all stages of the process; (7) Return to work on the highest level possible, with attention to the following hierarchy: Same tasks/same job, same employer; Modified tasks/similar job, same employer; Alternative tasks/new job, same employer; Same tasks/same job, other employer; Modified tasks/similar job, other employer; Alternative tasks/new job, other employer; (8) Assignment of meaningful tasks to the concerned employee; (9) Consideration to graduate the return to work in terms of tasks or time; (10) Individual reintegration associated to workplace-based occupational health and safety programs. The CRTWC monitors and stimulates the clarification of the situation, the cooperation and reciprocity between all stakeholders, according to the legislation on reintegration, to accomplish an early integration of the employee.
86The assessment is performed to verify that conditions for continued benefit receipt are met and to improve or retain the sick-listed individual’s labor market attachment. The municipal CM should assess if the sick-listed employee will be able to RTW with the pre-sick leave employer, and if this is not possible, whether work resumption with a new employer is an option. The FU assessment should be based on updated medical, social, and vocational information. The assessment should take place in cooperation with the sick-listed individual and other relevant agents such as the employer, medical experts, VR institutions, unions, and labor market experts. 87This decision rests with the CM who, if an interview is required, also decides when it should take place. At the interview, the CM may advise the sick-listed person about contacting the employer, possibilities for partial work resumption, modification of job demands, job counseling, and possibilities for VR. 88E.g. test of vocational abilities, workplace based job training, courses, and long-term education. 89CM is defined as a person or a team of persons who plans, organizes, and directs the coordination of health and occupational services for the sick-listed individual. 90To have the potential for harm if practiced incompetently. 91I.e. frequency of task performance within each of the domains. *All remaining significant values are <0.001.
92At least 2 years of experience and a variety of backgrounds, including nursing, case management, ergonomics, occupational therapy, occupational medicine and human resources 93Affinity mapping is an inductive, bottom-up process performed by a team to synthesize qualitative data into conceptually related groups without using predetermined categories. 94Administration, individual personal attributes, information gathering, communication, professional credibility, evaluation, problem-solving, and conflict management 95Examples of these skills are confidentiality, ethical practices, responding in a timely manner, and demonstrating good organization and planning skills listening and communication skills, the ability to be approachable and relate well with a wide range of people, consistently focusing on important RTW issues, and effective problem-solving.
All seven SR’s were published between 2005 and 2014. Of these reviews five were published in Canada [18–22], one in the Netherlands [23] and one in Denmark [11]. Two systematic reviews were economic evaluations [18–20].
The oldest systematic review, published by Franche and colleagues included articles from 1980 until 2003 [22]. Within this papers, it is concluded that that there is strong evidence that (1) job accommodation (i.e. modify the work in terms of tasks or time), (2) communication between stakeholders involved in the process, such as the health care professionals and the employer reduce work disability duration significantly among workers with Musculoskeletal disorders [22]. Moderate evidence was found that (1) early intervention (i.e. early contact with the worker by the workplace), (2) ergonomic work site visits, and (3) presence of a ‘Return to Work Coordinator’ reduces work disability. Finally, low evidence was found that the return to work interventions may also improve the QoL of the employees [22]. Furthermore, there seems to be moderate evidence of workplace interventions reducing sickness absence among workers with Musculo skeletal disorders (nevertheless not improving health outcomes among these workers) [23], whereby specific ergonomic job accommodations [20], goodwill and trust [21] were highlighted as essential for successful return to work [20, 21]. The goodwill and trust is necessary because of the complexity of beliefs, roles, and perceptions of different stakeholders involved in the process [21]. This often leads to social and communication barriers for return to work, but intermediary players such as rehabilitation or occupational health care providers and workplace supervisors may have the potential to help overcome the barriers and facilitate theprocess [21].
Overview of the selected qualitative studies
Overview of the selected qualitative studies
96in case of qualitative research year of conduction. 97Components of DM: (1) Early intervention; (2) Engagement of all stakeholders involved in the process; (3) Primary goal is jobretention or jobreintegration conform to the individual needs and demands of the job; (4) Recognition of the workplace to be most effective place for reintegration. (5) Retain the dignity of the employees and ensure an active participation during the reintegration process; (6) Consultation and communication between all stakeholders in all stages of the process; (7) Return to work on the highest level possible, with attention to the following hierarchy: Same tasks/same job, same employer; Modified tasks/similar job, same employer; Alternative tasks/new job, same employer; Same tasks/same job, other employer; Modified tasks/similar job, other employer; Alternative tasks/new job, other employer; (8) Assignment of meaningful tasks to the concerned employee; (9) Consideration to graduate the return to work in terms of tasks or time; (10) Individual reintegration associated to workplace-based occupational health and safety programs. The CRTWC monitors and stimulates the clarification of the situation, the cooperation and reciprocity between all stakeholders, according to the legislation on reintegration, to accomplish an early integration of the employee. *All remaining significant values are <0.001.
98They might be employees within a company, work for themselves or a consultancy that provides services to a variety of different companies. They might be employed at a social insurance organisation such as a workers’ compensation board.
The importance of communication and conflict resolution as essential components for a successful return to work are confirmed in Shaw’s review [20]. Despite this evidence, the most recently conducted systematic review [11] described that there is insufficient evidence to draw conclusions on the effectiveness of DM interventions within employees with a work disability due to musculoskeletal disorders. Furthermore, this study stated that it is impossible to determine specific program components or specific sets of components that are driving effectiveness.
The above-mentioned components of Franche and colleagues [22], in addition to supernumerary replacements, are proven to have financial merits in DM interventions (moderate evidence) [18, 19]. Stronger evidence is found for financial merits of DM interventions in multi-sector initiatives (manufacturing, health care, service sector) [18, 19]. In addition, Tompa and colleagues [18, 19] reported a moderate evidence for multi-component interventions consisting of education, physiotherapy, and work/vocational rehabilitation (vocational rehabilitation), and limited evidence for behavioral therapy among workers with a work disability [18, 19].
In the review of Shaw and colleagues [20] the preliminary competency domains (ergonomic and workplace assessment, clinical interviewing, social problem solving, workplace mediation, knowledge of business and legal aspects, and knowledge of medical conditions) and the principal activities (workplace assessment, planning for transitional duty, and facilitating communication and agreement among stakeholders) of the ‘return to work coordinator’ are indicated. Additionally, a substantial variability is found in the background and training of the ‘return to work coordinator’ and in the specific methods used for coordinating return to work. Professional backgrounds included occupational therapy, nursing, physiotherapy, vocational rehabilitation, ergonomics, case management, and psychology [20].
Three RCTs published between 2003 and 2007 were withheld, one was performed in Canada [24], on in Sweden [25] and one in the Netherlands [26].
Sickness absence and disability costs are reduced by active participation of the employee and involvement of different stakeholders (i.e. the employee, the employer and an ergonomist) for the return to work process with a proactive role for a case manager [25]. When the role of the case manager is supplemented by workplace assessment and work modifications a positive effect on return to work was detected [25, 26]. On the contrary, an exercise program based on cognitive behavioral approach had a negative effect on return to work and functional status [26]. Rehabilitation was completed to a larger degree and significantly faster for the employers using the DM program. Enhancing the benefits for employers and employees and achieving a positive benefit-cost ratio is possible by applying the case manager’s and the ergonomist’s experience and skills to individual workplaces knowledge sharing [25]. Furthermore, Anema and colleagues [26] proved that the effectiveness of these workplace interventions is not influenced by the socioeconomic system. Furthermore, Loisel and colleagues [24] illustrated the process of transfer of evidence from rehabilitation research to community practice. In the first phase the Sherbrooke model was developed, which showed a quicker return to work and improvement of QoL after 1 year follow-up, and cost-effectiveness after 6 years follow-up. In the second phase the PREVention of work handICAP (PREVICAP) program was established, with results of return to work improvement after 1 year and 3 years follow-up, but this effect decreased over the years. The PREVICAP program can be compared to a DM program and differs only slightly. In the third phase implementation of the program is discussed with the recommendation of following appropriate steps to ascertain that the program will fulfill planned objectives and community needs.
Clinical trials (mixed-method studies included)
Nine CTs, including three cohort studies [27–29], one quasi-experimental design [30], two before and after studies [31, 32], two cross-sectional studies [33, 34], and one article (excluded out of the table because of only checking the reliability and the validity of the Organizational Policies and Practices [OPP] questionnaire) [35] were published between 2000 and 2012. Moreover, the four MM’s [36–39], published between 2005 and 2010, are discussed in this paragraph. The studies were completed in the Netherlands [33], USA [27, 39], Sweden [28], Denmark [30, 36], and Canada [29, 38].
According to Rosenthal and colleagues [39] DM can be divided in two practices. The first is a predominant individual practice, which means that there is direct contact with the client and that the disability managers are case managers. The second is a predominant organizational practice, where administrative and management tasks focus on the organizational level.
Early intervention can reduce absence duration, given examples are receipt and acceptance of job accommodation offer [29, 38], job training [38], and targeted health care professional advice to the workplace on how to prevent re-injury [29]. In addition, ergonomic worksite visits [29, 34] reduce absence duration. Skisak and colleagues [32] complemented above-named components with case management, teamwork in the organization, trust in colleagues by the employee, trust in the DM process by the employee and the senior management, and acceptance of the DM program by all stakeholders. Alongside of a shorter absence duration, these components described by Skisak and colleagues [32] also improved patient satisfaction and direct disability costs. Lander and colleagues [30] found that case management and psychological stress management did not improve work capability. Adversely, psychological factors (e.g. self-efficacy, depression feelings, long term work stability, achieved coping skills, well-being, psychological improvements) improved the time to return to work [33] and work resumption [30]. Furthermore, a better health [28, 33], positive return to work expectations [28], a better work ability [28], and contextual factors [33] improved the time to return to work. By contextual factors D’Amato and colleagues [33] intended a specific climate that incorporates procedures and policies that are geared toward work resumption, both at organizational and national level, where the Dutch system is seen as the best practice. Other components that reduce absenteeism are absence tracking [27], timely return to work [27] and facilitation of transitional duty (i.e. assignment of meaningful tasks to the concerned employee) [27, 34]. This effect was measured in the first six years of the program [27]. Mobley and colleagues [31] reported that the first 72 to 100 weeks are a point of maximum beneficial effects on disability leave rate, resulting from both the administrative improvements, as well as, the rehabilitative improvements. Absence tracking, timely return to work and facilitation of transitional duty did not only had an effect on the reduction of absenteeism, but also provided a return on investment of direct costs only 2.4 : 1. This meant gaining $2.40 for every dollar spent in the program [27]. Moreover, a program incorporating the important stakeholders and communication between all stakeholders [34, 38] – especially the employee because he/she is the recipient of DM [34] – could significantly and cost-effectively reduce absenteeism among manufacturing employees. For this blue-collar work population reduction in the days of absence is less spectacular than for the white-collar work population [32]. Possible explanations are organizational and cultural differences or a higher prevalence of health risk factors among this target group [32]. Also in the study of Wendt and colleagues [27] the program worked better for hourly employees (in comparison with staff employees) in favor of the days of absence. Moreover, D’Amato and colleagues [33] found a small difference in the approach of a physical or mental health condition. Where work centrality (i.e. how important work is in someone’s life) is an important precondition for the physical condition, is support from the supervisor an important precondition for mental health conditions [33]. Burton and colleagues [34] described other components of DM can be recognized as useful: integrated management of behavioral-health-related disabilities between a clinical psychologist and Employee Assistance Program (EAP); independent medical examinations (when appropriateness of care or fraud and abuse may be an issue); charging of employees short-term disability costs to the manager’s/supervisor’s cost center; disability benefit design including limited 100% benefits; management disability reports including trend reports by work locations; work site disease management using occupational health nurses and EAP staff.
A case manager or ‘return to work coordinator’ is seen as someone with a broad range of responsibilities. These comprise developing and maintaining interpersonal relationships and communication through a complex social process, and problem-solving in a positive and effective manner that involves all key stakeholders. If these competencies are applied to improve the selection and training of ‘return to work coordinator’, improvements in return to work outcomes may result [37]. Also, the group of Burton and colleagues [34] highlights the importance of education. They stated that health care professionals, managers/supervisors, and HRM have to be educated on short term disability and available job accommodations. Additionally, Rosenthal and colleagues [39] described that the certification of DM specialists ensures that they have the educational and professional backgrounds, as well as the knowledge, to perform the requisite tasks associated with DM practice today. Through continuing education,practitioners can also keep abreast of the changes that will occur as the field continues to evolve [39].
The Case Manager Interview (CMI) and the Organizational Policies and Practices (OPP) questionnaire can be used to determine the management of the DM process in the workplace [35, 38]. The CMI motivates the sick-listed employees to resume work and adjusts for asymmetric information between the employee and the pre-sick leave employer, but not for a new employer [36]. The OPP questionnaire measures the extent to which the workplace achieves the following eight activities: safety diligence, safety training, ergonomic practices, disability case management, return to work, safety leadership, people-oriented culture, and joint health and safety climate [36].
Qualitative research
Five QSs were included published between 1999 and 2010, two in Canada [40–42], one in the USA [43], and one in Sweden [44].
DM has a very broad and sometimes nebulous definition that can include: (1) providing internal, direct services, (2) providing external, organizational services, (3) providing external consultation, working directly with insurance carriers [43]. Bernhard and colleagues [40] reported that the DM program is oriented to the needs of the employer and not of the employee and that certain components of the DM program can lead to a better outcome of return to work. These incorporate trust, respect, communication and labor relations experienced by a wide range of actors [42], and motivation and self-efficacy in combination with external support [44]. In the return to work process – similar to the processes of health promotion [44] – the ‘return to work coordinator’ is an essential figure [41]. This profession is recognized as the best professional background to resolve the fragmentation problems of DM functions at the service delivery level and offer employer assistance with developing integrated programs [41]. The ‘return to work coordinator’ needs specific competences to guarantee the success of return to work: individual traits/qualities, relevant knowledge base, return to work focus and attitude, organizational/administrative skills, assessment skills, communication skills, interpersonal relation skills, conflict resolution skills, problem-solving skills, and return to work facilitation skills [41]. According to Rosenthal and colleagues [43] the administrative and organizational skills often lack in practice. Gardner and colleagues [41] stated that more emphasis on mentorship and observation will be required to develop and evaluate necessary skills in this area. Another concern in the return to work process is that employers view disability primarily as a medical problem that is best addressed by medical personnel [43]. Furthermore, the goal of treating all injured and disabled people the same – as stated in the NIDMAR training framework – is a DM ideal. The implementation of this idea in practice can be difficult, because return to work-needs are established by legislative frameworks, which will distinguish between non-work-related cases and work-related cases, in favor of the last one [40].
Discussion
With this study, we aimed to report on the contemporary knowledge on the efficacy and the efficiency of the DM program from NIDMAR. The results of this systematic review show strong to moderate evidence that the DM program is effective. There is however not much evidence that the DM is cost effective.
The efficacy is shown by a quicker return to work [24, 25], improvement of QoL [22, 24], and patient satisfaction [32]. The effectiveness however, decreases over the years [20, 27], but is not influenced by the socioeconomic system [26]. The effective components incorporate job accommodation [22, 38], job training [38], facilitation of transitional duty [27, 42], ergonomic work site visits [22, 34], contact and communication between all stakeholders within the workplace [22, 42], health care professional advice [22, 29], employee involvement [34], early contact with the worker by the workplace [22], acceptance, goodwill and trust in the stakeholders, in the organization, and in the DM process [21, 32], and the presence of intermediary players such as a ‘return to work coordinator’, a case manager, a rehabilitation or occupational health care professional to overcome social and communication barriers [20, 43]. Alongside of these components and factors, education also seems to be an important element. The ‘return to work coordinator’ needs different competencies, such as: facilitate the communication between all stakeholders [20, 41], conflict resolution and problem solving skills [20, 41], knowledge of business and legal aspects and knowledge of medical conditions [20, 41], planning for transitional duty [20], return to work focus and attitude and return to work facilitation skills [41], competencies in ergonomic and workplaceassessment and in clinical interviewing [20]. According to Rosenthal and colleagues [43] the administrative and organizational skills often lack in practice. Besides there is a variability in the background and training of ‘return to work coordinator’ and in the specific methods used for coordinating return to work [20]. Therefore, Rosenthal and colleagues [39] stated that a certification of DM specialist and continuing education is necessary.
The efficiency of DM is investigated for direct costs only and can be proven by some components, such as contact between all stakeholders [18, 34], early contact with the worker by the workplace [18, 27], experience and skills of the case manager [24, 26], job accommodation [18, 34], absence tracking [27], ergonomic work site visits and facilitation of transitional duty [18, 27]. Efficiency of DM is highest in multi-sector initiatives [18,19, 18,19].
Defining the DM concept is a complex issue, it remains nebulously defined and this leaded to difficulties to overview the evidence. The search revealed a lot of literature about DM or return to work interventions, but an unambiguously analysis of the efficiency/efficacy of DM was difficult because of the literature focusing on different principles, pillars and components of the concept and this in populations with diverse disabilities. Besides it is not easy to investigate if research is specific focused on DM or on return to work in general. Therefore we decided to focus on the ten components of DM, described by Russo and Innes [5], to ensure a small amount of articles remained with an intervention as close as possible to the approach of NIDMAR. However, it remains difficult to make general conclusions on the international published literature on DM as in many studies a variety of (outcome) measures is used which all have a specific definition. This makes comparison of data difficult. Additionally, most papers in the area of DM are focused on workplace and return to work interventions for workers with musculoskeletal disorders [11, 23]. Due to lacking power in evidence, no conclusions could be drawn for mental health disorders and other health conditions [23].
DM is a broad and nebulous concept. The concept can be divided in system-oriented DM, which is directed at the administrative and managerial tasks with a focus towards the organizational level, and in service-oriented DM, which aims at a direct contact with the client [39, 43].
The above described and current literature is especially directed at DM for employees withmusculoskeletal disorders [11, 23]. Future research is needed to investigate the efficacy/efficiency of DM in mental health disorders and other health conditions (e.g. cancer, cardiovascular diseases...). Additionally, there is a lack in research towards the differences in approach for physical and mental health conditions, or for blue collar work population and white collar work population, or for non-work-related cases and work-related cases. Bernhard and colleagues [40] already proved that the DM ideal of treating all people the same with an injury of disability is not possible in practice because return to work needs are established by legislative frameworks. People with a work-related injury or disability take advantage of this. In addition, D’Amato and colleagues [33] reported a small difference in the approach of physical or mental health conditions.
Limitations of the study
To compose this article the PRISMA checklist, which is known as a qualitative appraisal for systematic reviews, was followed. The data collection captured a large number of articles by using three different languages and very broad range of years. The lower limit was chosen to be the starting year of NIDMAR, whereby all possible articles related to NIDMAR could be included. Limitations of this research is no certainty about a publication bias. If these limitations could be resolved, a clearer overview of the overriding evidence could be drawn. The review can benefit practice by using the above prescribed, evidence based components of DM. Moreover, the recommended skills of the ‘return to work coordinator’ can be applied in the training and education of this profession.
We specifically aimed to include also other studies then systematic reviews and RCT’s as the highest level of evidence. Including qualitative research for instance gave a better insight in the perceived importance of the different components of the DM program such as the importance of the return to work coordinator and showed at the same time shortcomings of the program such as the lack of consensus on the program itself. This aspect reduces the effectiveness of the Disability manager program and impedes research.
Conclusion
The overall conclusion of the review is that the DM management program has shown to be effective and efficient. However, DM still remains a broad and nebulous concept. That is why an international consensus about the method and the efficacy/efficiency of the DM components still has not been reached. Nevertheless, some components are highlighted more than others: job accommodation, facilitation of transitional duty, communication between all stakeholders, health care professional advice, early intervention, and acceptance, goodwill and trust in the stakeholders, in the organization, and in the DM process. In addition, a ‘return to work coordinator’ is an important person in DM programs, who needs an appropriate education. This review is relevant to companies and stakeholders, who already use DM or are planning to implement it.
However, the results from this systematic review do not give straightforward information of how these described components can be applied in the real world. Based on the current evidence we can conclude that a multi-stakeholder perspective is inevitable. This perspective involves a close collaboration between all stakeholders, including government, employer, healthcare professional, rehabilitation services and the person with the disability to enable his return to work. An important key issue in this process is the ability to communicate between all these different stakeholders. This means the use of a common language and the use of standardized assessment forms to get a clear view on the complexity related to the job requirements and the skills of the person. A return to work coordinator is necessary to facilitate and monitor the entire return to work process. Building capacity for sustainable multi-stakeholder collaboration, considering all components described in this review might maximize effectiveness, efficiency and productivity.
Conflict of interest
All authors declare no conflict of interest.
Authors’ contributions
All authors contributed in concept, design, data collection, analysis and interpretation; writing the article, critical revision and final approval.