
Abstract
BACKGROUND:
Automotive workers are engaged in occupational activities like engine tune-ups, oil changes, tire rotation, wheel balancing, replacing filters etc. These activities involve prolonged sitting, awkward postures, squatting and kneeling, which are known risk factors to cause patellofemoral pain syndrome (PFPS).
OBJECTIVE:
This paper aims to investigate the effects of selected biomechanical rehabilitative exercises (BRE) on integrated electromyography (iEMG) activity of vastus medialis oblique (VMO) and vastus lateralis (VL) muscles so as to identify suitable ones to alleviate PFPS of automotive workers.
METHODS:
Eleven subjects, automotive workers having PFPS, performed four BRE: (1) short arc quad with neutral hip position (SAQN), (2) short arc quad with externally rotated hip position (SAQER), (3) medial tibial rotation (MTR), and (4) hip adduction (HA).
RESULTS:
Mean iEMG activity of VMO muscle is more than that of VL muscle during all BRE. However, one way ANOVA with repeated measures indicates that mean iEMG activity of VMO muscle is significantly higher than that of VL muscle during SAQER only. VMO/VL ratio is not significantly different across the four BRE.
CONCLUSIONS:
Results suggest a range of options for choosing appropriate BRE for treating automotive workers with PFPS. However, SAQER may directly be recommended for preferential strengthening of VMO muscle.
Keywords
Introduction
Patellofemoral pain syndrome (PFPS) is a retropatellar or peripatellar pain that affects general population. In simpler words, it is a syndrome characterized by knee pain ranging from mild to severe discomfort. PFPS is mainly caused due to the abnormal tracking of the patella within the femoral trochlea [1]. Abnormal tracking may occur owing to a delayed onset of the VMO muscle relative to VL muscle. PFPS can, therefore, be considered to be an outcome of the lateral malalignment of the patella [2]. Vastus medialis oblique (VMO) and vastus lateralis (VL) muscles work synergistically to stabilize patella during dynamic knee extension. It has been hypothesized that weakness of the VMO muscle is linked to PFPS. Therefore, many clinicians focus their treatment of PFPS on restoring the strength of VMO muscle using a number of exercise programs, which are referred to as biomechanical rehabilitative exercises (BRE) in this paper. In general, exercise programs have been used widely in healthcare and rehabilitation [3–5]. Electromyography (EMG), a widely used tool, is capable of providing information regarding muscle activity during BRE.
A number of studies have compared VMO and VL activations, as well as VMO/VL ratio across different BRE to find out those which may selectively strengthen the VMO [6–8]; however, it is debatable whether the VMO can be selectively strengthened. Many of these have reported not to achieve a significant increase in VMO activity compared to VL activity [9, 10]. Laprade et al. [6] demonstrated that both, VMO and VL, muscles are active throughout the full range of motion during open chain knee extension. Livecchi et al. [11] presented no significant difference in VMO/VL ratio across four exercises, namely, straight leg raise (SLR) and knee extension, both with lower extremity in neutral as well as externally rotated positions. However, Hanten et al. [12] reported that EMG activity of VMO muscle is significantly higher than that of VL muscle during hip adduction (HA). Medial (internal) tibial rotation (MTR) exercise is supported for selective strengthening of VMO muscle in a study [13]. Kang et al. [14] demonstrated a significant increase in VMO/VL ratio during closed-kinetic chain exercise.
Short arc quad (SAQ) exercises with neutral and externally rotated hip position, MTR and HA have not been comprehensively evaluated with respect to their effects on the VMO and VL activities on occupational workers. However, six BRE, including those selected in this paper, have been compared, on general population not having PFPS to explore those which may selectively activate VMO [15].
Automotive workers are engaged in occupational activities like engine tune-ups, oil changes, tire rotation, wheel balancing, replacing filters etc. These activities involve prolonged sitting, awkward postures, squatting and kneeling, which are known risk factors to cause PFPS. The prevalence of PFPS among automotive workers has not been reported earlier. As such a preliminary survey is carried out in the present study on 38 automotive workers from 12 car-repair units in nearby region for the purpose. Workers complaining knee pain, having a minimum work-experience of four years, and having not undergone any major surgery are included in this study. The prevalence of PFPS is found as 28.94% . PFPS has also been identified as one of the main reasons of absenteeism of automotive workers in car-repair units resulting in loss time. Timely treatment of PFPS would not only be beneficial to automotive workers but also to the owners/managers of car-repair units. The incidence of PFPS in the general population has been reported as one in four individuals [16].
The objective of the present study is to investigate the effects of selected BRE on iEMG activity of VMO and VL muscles of automotive workers having PFPS. To increase dynamic stabilization of patella, VMO muscle should be preferentially activated over VL muscle during an exercise. An exercise producing overall strengthening of VMO and VL muscles together may not be useful for the purpose. Preferential activation of VMO muscle during an exercise is achieving significantly increased VMO/VL ratio, i.e., VMO activity being significantly higher than VL activity, which has been advocated as a treatment for PFPS. As such, four BRE are experimented in the present work to identify those which produce preferential activation of VMO muscle of automotive workers having PFPS (Figs. 1–4).

Short arc quad with neutral hip position.

Short arc quad with externally rotated hip position.

Medial (internal) tibial rotation.

Hip adduction.
A brief demonstration of EMG equipment and four BRE are given to each of 11 subjects taken in the study, and an informed consent is obtained prior to experiments. Inclusion criteria of subjects are automotive workers complaining knee pain, having a minimum work-experience of four years, and having not undergone any major surgery in last five years.
A 2.2 Kg weight is taped at the upper side of the heel during SAQ exercises. The dominant leg, as determined by handedness of the subject, is used for all subjects for electrode placement by shaving and cleaning (with spirit and towel) the designated areas to remove hair and dead skin cells. The electrodes are placed parallel to the direction of the muscle fibers on the VMO and VL following standard norms (International Society of Electrophysiology and Kinesiology [17]). According to Zipp [18], the fibers of the VMO run at approximately 55 degree angle medial to the quadriceps tendon, and the electrode is placed 20% of the distance from the medial joint line of the knee to the anterior superior iliac spine. The fibers of the VL are at 12 to 15-degree lateral to the quadriceps tendon. The electrodes are placed at the midpoint between the head of the greater trochanter and the lateral femoral epicondyle. Ground electrodes are placed on 6 to 8 cm from the inferior pole of the patella along the bony shaft of the anterior tibia [16].
Surface EMG signals are acquired using AcqKnowledge 4.1 software (Biopac Systems, Inc., USA). EMG activities are recorded using Biopac MP 150 (Biopac System, Inc., USA). Bipolar adhesive surface electrodes (Ag-AgCl) are used over the muscle bellies of the VMO and VL. Room temperature is about 36ºC. Concentric and eccentric phases of each exercise are marked distinctively. Subjects are allowed a five minute rest period in between each exercise. The EMG data are sampled at 1,000 Hz and amplified 2,000 times by the Tel-100 unit. The peak value of the iEMG data for each muscle is used for normalization.
The subject is in supine position during short arc quad exercises (SAQN and SAQER), and is instructed to maintain his dominant leg at a knee angle of 60º using bolster and ankle over the edge of the exercise table. The dominant leg is in neutral position during SAQN and in externally rotated position during SAQER. There are three verbal cues ‘lift’ at the first beat, ‘lower’ at the second beat and ‘rest’ at the third beat.
Each subject carried out five repetitions of each exercise. EMG data during middle three trials are considered for the analysis and remaining trials are excluded. In order to minimize possible interference, all EMG processes are in accordance with the standard norms. The EMG signals are band-pass filtered with cut off frequency as 20 to 500 Hz using AcqKnowledge 4.1 Software, Biopac Systems, Inc. These signals are then full-wave rectified and integrated using MATLAB Software, The Mathworks, Inc. The above process of obtaining iEMG is repeated for each muscle. An electromyography signal consists of two phases, a concentric phase and an eccentric phase. A concentric phase is characterized by a contraction in the muscle which is caused by the approximation of the muscle’s contractible units. On the contrary an eccentric phase is typified by relaxation or lengthening of muscle. Figure 5 shows concentric phase and eccentric phase of an electromyography signal of VMO and VL muscles All stages of EMG signals (raw EMG signal, EMG signal without DC offset, rectified EMG signal and integrated EMG signal) are shown for VMO muscle during SAQN (Fig. 6).
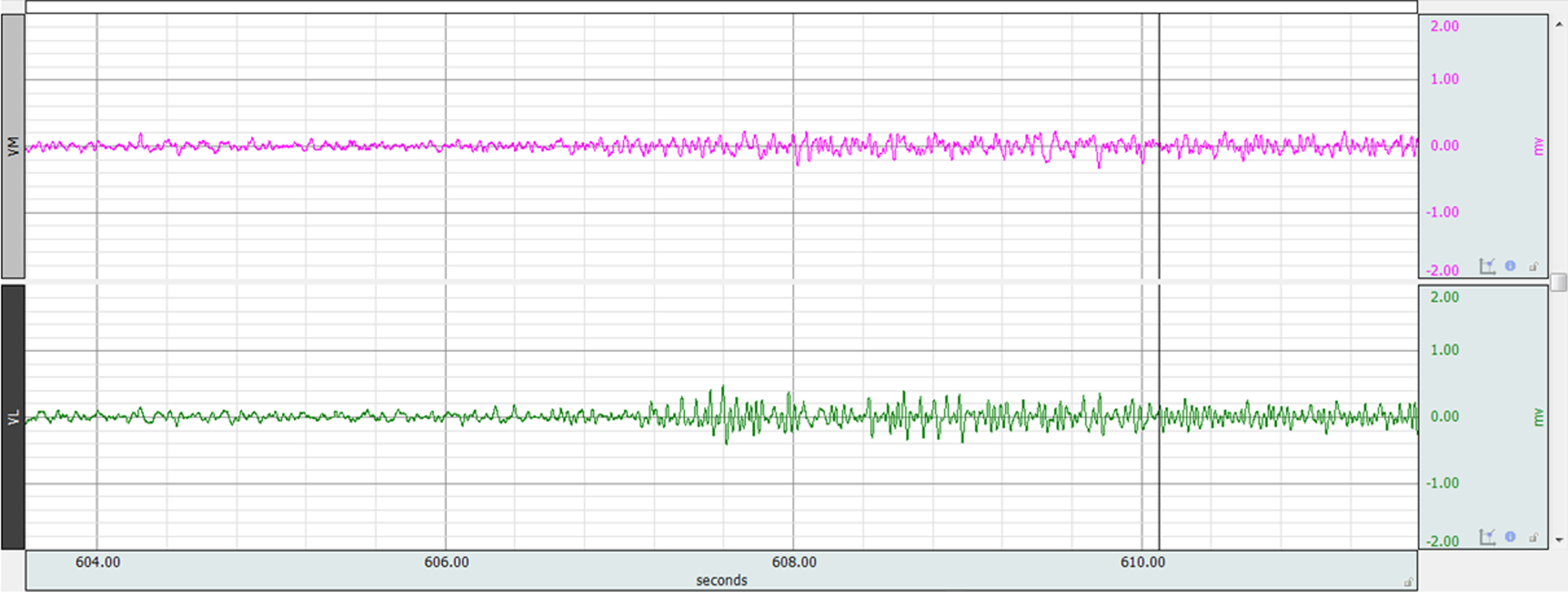
EMG activity for VMO and VL muscles.
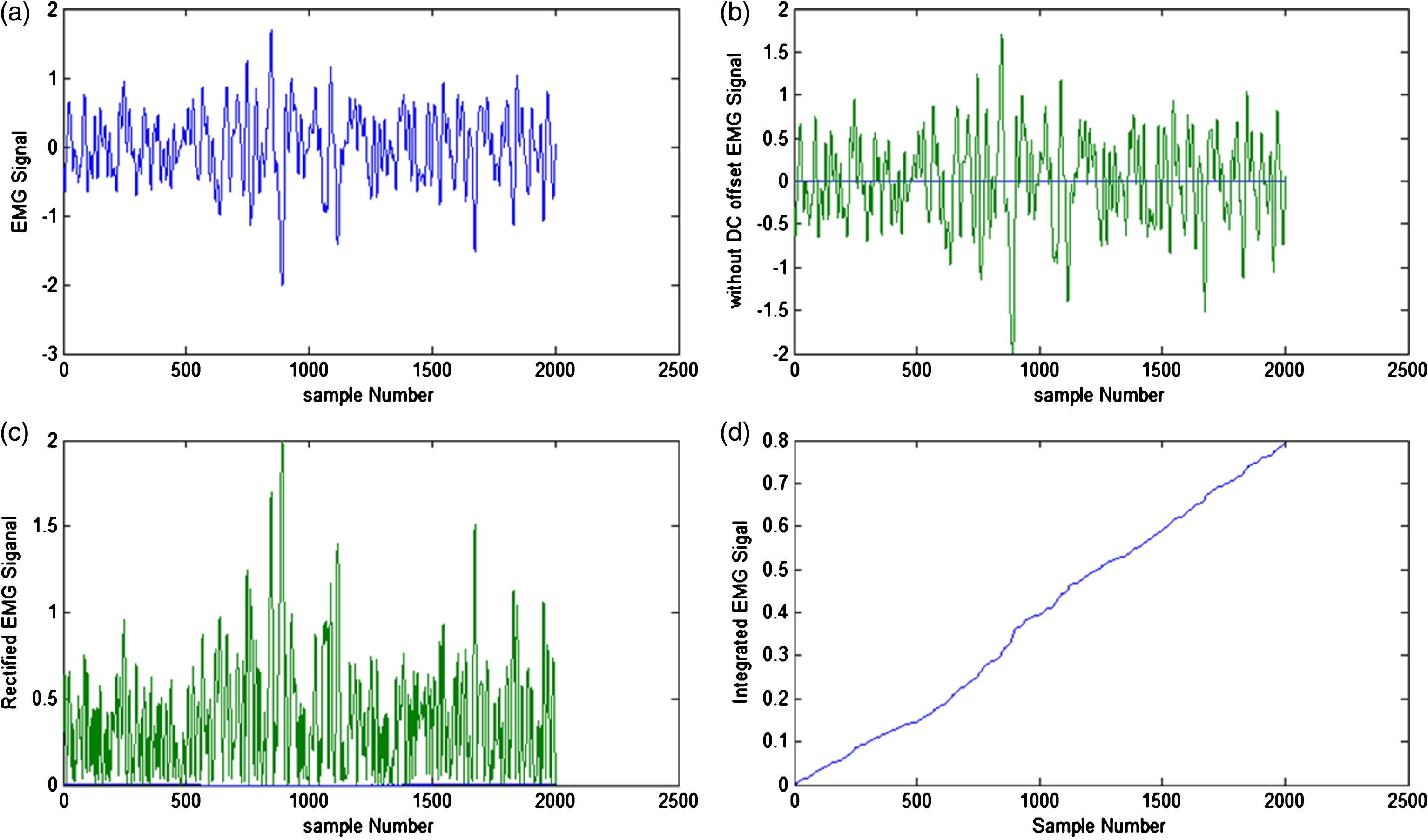
Stages of EMG Signals for VMO muscle during SAQN (a) Raw EMG signal (b) EMG signal without DC offset (c) rectified EMG signal (d) Integrated EMG signal.
iEMG differences among all exercises are tested for statistical significance using one-way analysis of variance (ANOVA) with an alpha level of 0.05 for each muscle. If significance is found using one-way ANOVA, post hoc analysis using least significant difference (LSD) test is performed to compare exercises using P < 0.05 for the level of significance. Means and standard deviations are computed for the normalized EMG readings of the VMO and the VL for all the exercises. Normalized iEMG values for the VMO and VL muscles during all four BRE are computed as percentage of maximum voluntary contraction (% MVC). MVC is defined as the maximum iEMG value recorded for a specific muscle under consideration. This procedure of normalization of iEMG value using MVC ensures that the consistency for normalization exists within each muscle. Further this procedure is based on dynamic movements of experimental tests [16].
Experiments are performed on 11 male subjects (age range: 25–58 years). Name, age in years, height in centimetres, weight in kilograms and work-experience in years of each subject are recorded. Body mass index is calculated using height and weight data for each subject (Table 1).
Demographic data
Demographic data
Normalized iEMG values for the VMO and VL muscles during all four BRE are listed as percentage of maximum voluntary contraction (% MVC) in Table 2. It is noteworthy that VMO/VL ratio is greater than one for all BRE. In other words, muscle activity of VMO is more than that of VL for all BRE. One way ANOVA with repeated measures indicates that VMO activity is significantly different from VL activity for SAQER. There is no significant difference in the VMO/VL ratio across the four BRE. The results show that SAQ and HA produce significantly higher VMO activity than MTR. Whereas for VL muscle, HA produces significantly higher iEMG activity than other three BRE.
iEMG (% MVC±SD) value of VMO and VL for all four BRE
Analysis of individual activity of VMO and VL muscles during all BRE is as follows. iEMG value of VMO muscle during HA is 81.61 (Table 2), which is the highest value across all BRE. SAQ produced significantly higher electrical discharge of VMO than MTR. HA produced significantly higher VL activity than SAQN, SAQER and MTR.
Integrated EMG is regarded as an appropriate tool for the evaluation of muscle function in occupational rehabilitation in spite of the fact that the exact relationship between EMG and muscle tension is argued [12]. Many studies in the recent past used integrated EMG for the evaluation of muscle function [16, 19].
To selectively strengthen VMO muscle, it is argued that EMG activity of VMO muscle should be significantly higher than that of VL muscle during a rehabilitative exercise. In the present study VMO/VL ratio is more than one (ranging from 1.03 for MTR to 1.19 for SAQER) for all four BRE, which is in tune with the fact that VMO should be preferentially strengthened to alleviate PFPS. Higher VL activity may lead to a lateral force on the patella which is considered to be the main cause of PFPS. Further, one-way ANOVA indicates that VMO activity is significantly higher than VL activity during SAQER only. In other words, VMO can be strengthened selectively during SAQER. iEMG readings of VMO and VL muscles are 70.02 and 59.37 respectively during SAQER (Table 2). Though iEMG activity of VMO muscle is notably higher than that of VL muscle during SAQN and HA, yet the difference is not statistically significant. MTR is able to increase the proportional activation of VMO slightly when compared with that of VL (Table 2). VMO/VL ratio is not statistically significant across the four BRE.
Short arc quad (SAQ) exercises, in general, produce higher VMO and VL activations than straight leg raise (SLR) exercises [16]. SLR exercises require lesser force from the VMO and VL, resulting in lower EMG activities of these muscles. Concentric and eccentric activation of the quadriceps muscles during SAQ exercises involve greater participation of the VMO and VL muscles. As such SAQ exercises may be preferred to SLR exercises to alleviate PFPS of automotive workers in the present work.
VMO and VL activations are not significantly different across SAQN and SAQER. These results are in agreement with the findings of previous investigations, which stated no significant changes in electrical discharge of the VMO and VL muscles across SAQN and SAQER [11, 20]. Stimulation of VMO muscle with respect to external rotation of hip has been an underlying hypothesis in some the earlier reported work [11, 21].
Medial tibial rotation is also experimented to alleviate PFPS of automotive workers under study as it has been recommended for the preferential strengthening of VMO muscle by some of the researchers [6, 13]. MTR with 110 degree of knee extension was recommended for selective strengthening of VMO muscle [6]. However, in the present study it was found that though VMO activity is higher than VL activity, yet the difference was not significant. As such MTR may not be supported to alleviate PFPS of automotive workers under study. This finding is in accordance with the result of a previous study [12], wherein it was shown that VMO/VL ratio is not significantly higher than one during MTR.
Hip adduction exercise is also investigated in the present work to alleviate PFPS of automotive workers, as it has been recommended for the preferential strengthening of VMO muscle by some researchers [12, 22–24]. Though in the present work iEMG activity of VMO is notably more than that of VL muscle during HA exercise, yet this difference does not turn out to be statistically significant. There are some studies which support this result i.e. VMO muscle activity is not significantly higher than VL muscle activity during HA [1, 25]. The difference in the results may be attributed to difference in method of study, e.g., (i) using different types of electrodes, i.e., surface electrodes vs. needle electrode, (ii) performing experiments with no/less resistance or with maximal-effort isometric contractions etc.
Options for strengthening the VMO muscle of automotive workers according to outcomes gleaned from the present study can be concluded as below. All four selected exercises contribute higher VMO/VL ratio. However, VMO activity is significantly higher than VL activity during SAQER only; therefore it can be recommended for preferential strengthening of VMO. Mean iEMG activity of VMO muscle is notably higher than that of VL muscle during SAQN and HA, yet the difference is not statistically significant. MTR may not be supported to alleviate PFPS of automotive workers under study. Lastly VMO/VL ratio is not statistically significant across the four BRE. Overall, the results of the present study provide a range of options for choosing appropriate BRE for treating automotive workers diagnosed with PFPS. However, a sample of automotive male-workers of local population is not a representative of whole country. Another limitation of the study is crosstalk between electrodes in surface electromyography of concerning muscles. Future research should involve a larger sample size across a wider region including both genders and a range of resistance exercises.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We sincerely acknowledge the help and support of Dr. Shellyka Ratnakar, Physiotherapist, Saran Ashram Hospital, Dayalbagh, Agra. This work is supported by UGC, New Delhi, under Grant F. No. 3-38/2012(SAP-II) dated 02/10/2012; and by DST, New Delhi, under Grant Dy. No. 100/IFD/2563/2012-2017 dated 20/07/2012.