
Abstract
BACKGROUND:
Whole body sprint-interval training (WB-SIT) represents a mode of exercise training that is both time-efficient and does not require access to an exercise facility.
OBJECTIVE:
The current study examined the feasibility of implementing a WB-SIT intervention in a workplace setting.
METHODS:
A total of 747 employees from a large office building were invited to participate with 31 individuals being enrolled in the study. Anthropometrics, aerobic fitness, core and upper body strength, and lower body mobility were assessed before and after a 12-week exercise intervention consisting of 2–4 training sessions per week. Each training session required participants to complete 8, 20-second intervals (separated by 10 seconds of rest) of whole body exercise.
RESULTS:
Proportion of participation was 4.2% while the response rate was 35% (11/31 participants completed post training testing). In responders, compliance to prescribed training was 83±17%, and significant (p < 0.05) improvements were observed for aerobic fitness, push-up performance and lower body mobility.
CONCLUSION:
These results demonstrate the efficacy of WB-SIT for improving fitness and mobility in an office setting, but highlight the difficulties in achieving high rates of participation and response in this setting.
Introduction
Despite overwhelming evidence supporting the positive health benefits associated with physical activity [1] the majority of north American adults fail to achieve physical activity levels (150 minutes of moderate to vigorous activity per week) recommended by current guidelines [2]. While the behavioural factors that determine participation in physical activity are multifaceted and complex, both limited time and lack of convenient access to exercise facilities are commonly cited barriers [3].
Sprint-interval training (SIT), a sub category of high-intensity interval training requiring short bursts of all-out effort, induces adaptations typically associated with endurance training in a fraction of the exercise time [4, 5]. While SIT may therefore provide a means of reducing the time barrier associated with an inactive lifestyle [6], most tested SIT protocols require a stationary bike. Thus, while SIT is a time-efficient alternative to endurance training, continued need for access to exercise facilities and/or equipment remains a barrier to regular participation in SIT. We have recently demonstrated the efficacy of a whole body, low volume, sprint-interval training (WB-SIT) protocol that requires no equipment for improving cardiovascular fitness and muscular endurance [7]. As this WB-SIT protocol is both time-efficient and does not require access to an exercise facility and/or equipment, it may represent a promising means of increasing physical activity and aerobic capacity in the general population.
Based on the significant amount of time most individuals spend at work, the workplace represents a potentially effective site for interventions aimed at increasing physical activity. As a result, studies utilizing workplace interventions have recently become of great interest [8–10]. Combined with evidence that work-place exercise interventions can improve physical fitness [11], the time efficiency, and convenience of WB-SIT suggests that a WB-SIT workplace intervention may be a promising means of improving physical activity and aerobic capacity. However, the feasibility of implementing a structured, supervised, WB-SIT intervention in a workplace setting is currently unclear. Further the efficacy of a WB-SIT intervention for improving physical fitness in a workplace setting has not been examined.
Therefore, the purpose of the current work was to examine the feasibility and efficacy of a WB-SIT intervention in an office environment. Specifically, the proportion of participation and response rates to a structured, supervised, 12-week WB-SIT intervention implemented in a workplace setting were examined. The impact of this intervention on aerobic capacity and upper body/core endurance were also examined.
Methods
The current study utilized a quasi-experimental pre-test/post-test design. Participants were recruited from a large Manulife office in Waterloo, Ontario. A total of 747 employees (average age, 40 years; 26% male; 74% female) were invited to participate in this study via an email blast that included a brief description of the study and inclusion/exclusion criteria. This resulted in 42 employees completing an online sign-up form. From this initial group of interested employees, 31 participants were enrolled in the study after completing the required consent and indemnity forms, and pre-study fitness screen. The experimental procedures performed in the current study were approved by the Health Sciences Human Research Ethics Board at Queen’s University and conformed to the Declaration of Helsinki. Verbal and written explanation of the experimental protocol and associated risks was provided to all participants prior to obtaining written informed consent.
Participant screening
Individuals interested in participating in this study completed an online sign-up form that included initial screening criteria. Specifically, participants were informed that participation was limited to individuals between the ages of 18 and 45 who were free of any history of cardiovascular or metabolic disease. In addition, the sign-up form required individuals to complete the Physical Activity Readiness Questionnaire Plus [12] with anyone who answered yes to any of the questions on this questionnaire being excluded. This screening was repeated in person during informed consent and prior to completion of pre-training testing.
Baseline and post-intervention measures
Following screening, participants completed a battery of physiological, strength, movement, and anthropometric measures with all tests being repeated in identical fashion both before (pre; completed 1 week prior to the start of training) and after (post; 48–72 hours after final training session) completion of a 12-week exercise intervention. Following measurement of height and weight, aerobic fitness was assessed using the Canadian Society for Exercise Physiology (CSEP) modified Canadian Aerobic Fitness Test (mCAFT) [13]. Upper body strength was assessed using the CSEP push-up protocol. If participants performed modified push-ups these were counted as 0.8 instead of 1.0 for a regular push-up. Core endurance was accessed by having participants hold a V-sit, back extension and right and left side plank positions for as long as possible [14]. In addition, participants were asked to complete two standardized movements, the deep squat and hurdle step [15, 16] to screen for active lower body mobility. These movements were assigned a score of 0–3 (based on explicit criteria), where a score of three indicated that the movement was completed successfully without compensation.
Exercise training intervention
Training was performed 2–4 times per week for a period of 12 weeks. All training sessions were supervised and were completed at the workplace between 3 and 5 in the afternoon. Each training session began with a standard warm-up lasting approximately 3 minutes and was followed by a similar cool-down period. Training session required participants to complete a single set of WB-SIT consisting of a total of eight 20-second intervals separated by 10-second rest periods for a total training time of 4 minutes. Thus, each training session, including warm-up, intervals and cool down required approximately 10 minutes. The intervention progressed from 2 training sessions in week 1, to 3 training sessions in week 2 and 3, to 4 training sessions for the rest of the intervention. All intervals required participants to perform whole body exercises (including but not limited to, burpee push-ups, mountain climber push-ups, jumping jacks) as fast as possible. In a further attempt to provide progression, avoid participant boredom and maintain motivation, different exercises were utilized throughout the training intervention (See S1 Table for a description of all exercises completed). Attendance at all prescribed training sessions was recorded and ratings of perceived exertion (RPE; 10-point scale with anchors of “No exertion at all” [1] to “Maximal exertion” [10]) were recorded following the completion of each training session.
Statistical analysis
Results are expressed as means±standard deviation (SD). Level of significance was set at p < 0.05 for all statistics. Non-paired t-tests were used to examine differences in baseline characteristics between participants who were lost to follow-up and those that completed the intervention (responders). Differences between pre- and post-training values for those participants completing the intervention were compared using a paired t-test, where ordinal scores from the movement screen were compared using non-parametric repeated samples Wilcoxon signed rank test.
Results
Of the 41 employees that competed the on-line sign-up sheet, 31 were enrolled in the study and completed pre-testing. Of these 31 participants, 11 completed post-testing (Fig. 1A). Enrolment of 31 participants out of a possible 747 employees represents a proportion of participation of 4.2%, while 11 of the 31 participants completing the intervention represents a response rate of 35%. The number of participants completing at least 1 training session per week and more than 60% of training sessions per week are presented in Fig. 1B and 1C, respectively. In the responders, the average number of training sessions completed was 33±6.7 out of a total of 40 possible training sessions representing an average compliance of 83±17%.
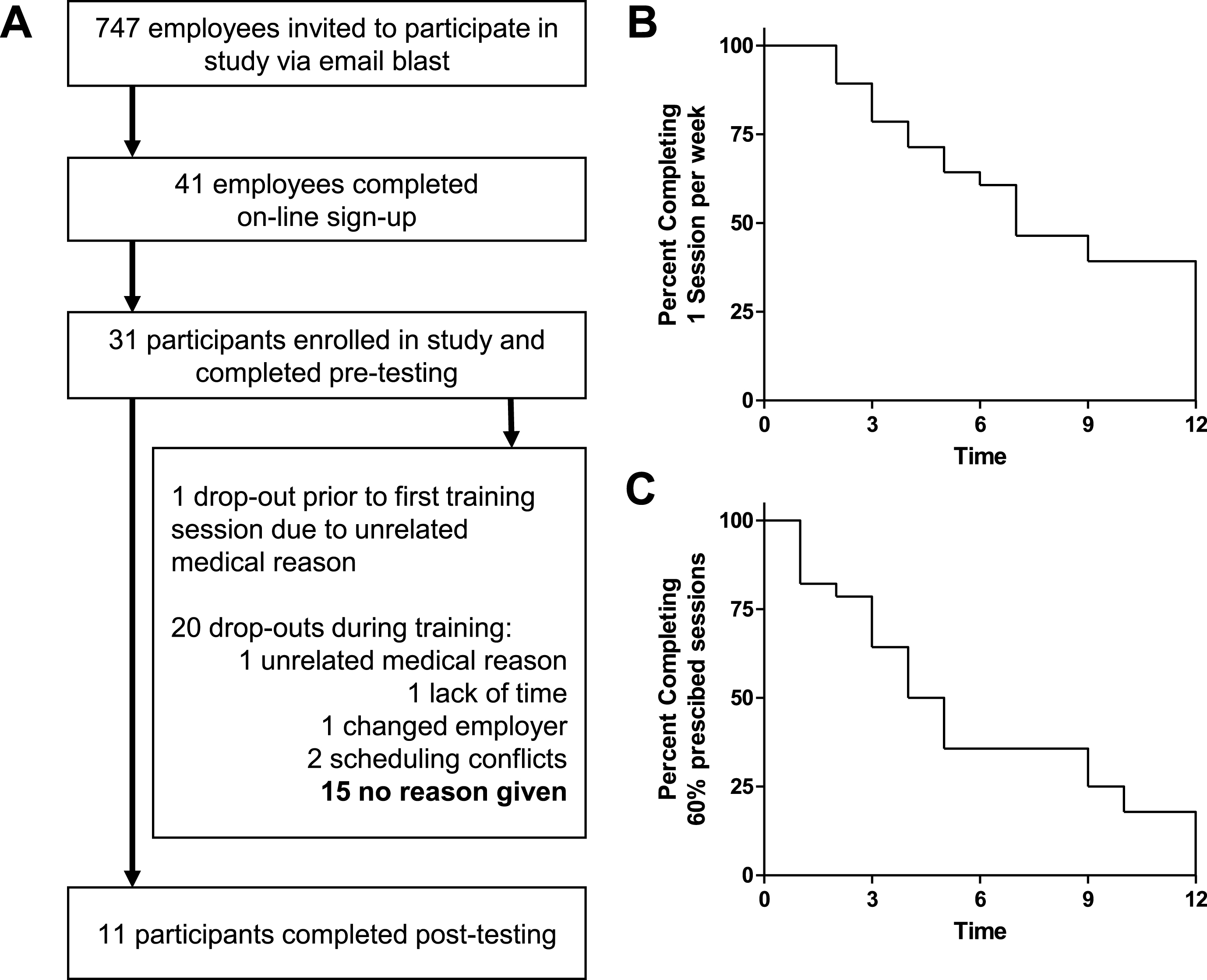
Employee response and participation during a 12 week WB-SIT intervention. Flow of participants throughout the intervention is presented (A) along with survival plots presenting the number of participants completing at least 1 exercise session per week (B) or at least 60% of scheduled exercise sessions per week (C).
Physical characteristics for participants lost to follow-up and responders are presented in Table 1. There were no differences in the physical characteristics of individuals who were lost to follow-up and the responders. In the responders, there were significant (p < 0.05) improvements in aerobic fitness score (+7%) and push-ups performed (+50%), while no change was observed for any measures of core endurance (Table 1). In addition, lower body mobility was improved significantly (p < 0.05) based on score improvements in the deep squat (+17%), hurdle step – left (+27%), and hurdle step – right (+30%) (Table 1). RPE scores and total number of participants per session over the duration of the intervention are presented in Table 2.
Physical characteristics for all participants
Values are Mean±SD. Max reps, maximum number of repetitions. *p < 0.05.
Rate of perceived exertion (RPE) and total number of participants per session over the duration of the intervention
Values are Mean±SD.
The current study was designed to examine both the feasibility and efficacy of a structured, supervised, WB-SIT intervention implemented in a workplace setting. While there were significant improvements in aerobic fitness and upper body strength in those participants completing the intervention, we observed a low proportion of participation (∼4%) and rate of response (35%). Thus, the current study does support the efficacy of WB-SIT for improving aerobic fitness in a workplace setting, but also highlights several issues that need to be addressed to improve participation and response rates in future interventions.
Improvements in aerobic fitness, strength and movement
Due to its brevity, and the lack of equipment required, WB-SIT overcomes two commonly reported barriers to physical activity, both time and access to exercise facilities and/or equipment. Further, consistent with our previous demonstration in university aged students in a lab-based study [7], WB-SIT was able to induce significant improvements in both aerobic fitness scores, upper body strength (push-up performance) and in lower body mobility. These results add to a growing body of literature that very low doses of high-intensity exercise are capable of improving aerobic fitness [4, 17], and demonstrate for the first time that these beneficial effects can be achieved when WB-SIT interventions are implemented in a work-place setting with middle-aged adults.
Proportion of participation
While the changes in fitness we observed are consistent with previous studies (see Shephard 1996, for review), the low proportion of participation and rates of response in the present study suggest that overcoming two commonly reported barriers to physical activity (access to facilities and/or exercise equipment and time) is not sufficient to entice significant employee participation in a supervised, work-place training program. Importantly, while it is known that the behavioural factors impacting participation in physical activity are complex, these data highlight the need for the development of comprehensive approaches that engage and retain participants in work-place based training interventions aimed at improving physical fitness. In the current study we observed a proportion of participation of less than 5%. While our strict exclusion criteria (18–45 years; free of any disease history; answered no to all questions on PAR-Q Plus; had to be available between 3 and 5 pm for training sessions) likely contributed to the low proportion of participation, low rates of participation are a common problem associated with work-place intervention studies, particularly those that do not provide opportunities for lifestyle counselling in addition to training [11, 18].
Response rate
In addition to observing a low proportion of participation in the current study, we also observed a low response rate. In total, only 11 of the 31 participants who completed pre-testing completed post-testing. One issue affecting the response rate was the availability of training times (exercise supervisors were present at the workplace from 3 to 5 pm only). By design, it was assumed that this window would provide ample opportunity for participation; however, non-completers noted that this window was not sufficient as work demands (i.e., meetings, etc.) and life demands (i.e., picking up children from school) affected participant’s availability within the prescribed window of time. It was interesting that select participant’s noted work demands as a limiting factor, as Manulife was very supportive in trying to facilitate participation during the prescribed 3 to 5 pm window. Work reorganization was a second issue that affected response rate; during the course of the research study Manulife was undergoing a re-organization, where some participants were required to relocate to alternative offices, such that they were no longer able to participate. Work reorganization is common in most industries and is an important external factor to consider when designing an exercise intervention in an office setting.
It is also likely that the response rates were low as the research design failed to utilize strategies like social activities that might have helped to improve response rates. For example, the use of exercise teams [19, 20], personal and team goal setting [20] and the provision of incentives for study completion [21, 22] have all been successfully utilized to improve participant retention previously. The response rate of the current study might have been improved by training some participants to act as group-leaders capable of acting as exercise supervisors and providing social support and motivation to participants, in addition to the provision of more flexible training schedules. While the reasons for the low rates of participation and response observed in the current study are not known, this study demonstrates that workplace participation in exercise programs are challenging and that workplace-related barriers need to be considered (time-availability, environment, social aspects, etc.). Thus, future interventions should be developed that implement several strategies shown to improve participation and retention rates such as the use of incentives [20, 21], lifestyle interventions [18], one-to-one counselling, exercise teams [19, 20], and personal and team goal setting [20].
Limitations
Although the current study represents an important first attempt to implement a WB–SIT intervention in a work place, our study design suffered from several limitations that should be considered in future office exercise interventions. First, our study design failed to include intervention approaches designed to engage and retain a large portion of the work-place population. This failure likely contributed to the low rate of participation observed in the current study. Second, the rate of participation and response rate in the current study were both likely adversely affected by our inability to provide flexible availability of training supervision (training only offered between 3–5 pm). Finally, the low response rate was likely also influenced by our inability to include a social aspect in our intervention. Social approaches improve participant retention [19–22] and should be utilized in future workplace interventions.
Conclusion and future directions
We have demonstrated that a supervised, WB-SIT intervention is capable of improving physical fitness in a workplace setting; however, we also observed low rates of participation and response. Together, these results provide further evidence supporting the efficacy of WB-SIT but also highlight the importance of utilizing an integrative approach in future interventions that include lifestyle interventions, social activities, incentives, and goal setting at both an individual and team level to improve participation and response rates.
Conflict of interest
None to report.