
Abstract
BACKGROUND:
Several studies have explored the factors influencing patients’ return to work (RTW) status. However, only few studies have tried to explore the predictors for RTW in subpopulations in terms of different levels of disability, particularly in the Chinese population.
OBJECTIVE:
This study describes the trends in patient’s RTW and explores the predictors associated with RTW for patients with work-related injury in Mainland China.
METHODS:
A total of 457 patients with different types of injury were followed up for one year. Patients were stratified into three groups according to the grade of disability as follows: mild, moderate, and severe. Variables affecting RTW were then compared between the three groups, and multiple logistic regression was performed to identify the predictors for RTW.
RESULTS:
The RTW rates during the study period were significantly different among the three groups. RTW tended to increase rapidly during the early stage, but the increase plateaued during the later stage. For the mild disability group, educational level, expectation to RTW, and other types of injury (e.g., spinal cord injury, traumatic brain injury, and burn) were significant predictors for RTW. White-collar work and better employer satisfaction were positive predictors for RTW for the moderate group. Meanwhile, no significant predictor for RTW was determined for the severe disability group.
CONCLUSIONS:
RTW tended to increase rapidly during the early stage, but the increase plateaued during the later stage. The predictors for RTW also varied among the patients with different levels of disability. These predictors may help vocational rehabilitation service providers provide more accurate intervention.
Keywords
Introduction
In 1999, the annual worldwide incidence of mortality due to work-related injuries was approximately 100 million [1]. Although the rate of fatal work injuries has significantly declined over the past twenty years, particularly in developed countries [2], approximately 0.3 million deaths are still attributable to work-related injury [3] and several survivors have various types of injury [4, 5]. Many studies indicated that patients are absent from work after injuries and some could not even return to work (RTW) permanently [6, 7], which results in a large economic burden to both society and individual [8]. Furthermore, patient care and daily medical costs become a burden to the family [9].
To optimize the vocational rehabilitation program for work-related injury patients, some researchers conducted studies to explore the factors that might negatively or positively influence the patient’s RTW status. In 1987, MacKenzie et al. [10] completed a relatively early study based on 266 individuals who had severe traumatic injuries that required hospitalization. Their findings indicated that the rates of RTW varied significantly among patients with different types of injuries. For instance, patients with head or spinal cord injury (SCI) was at highest risk of non-RTW, and those with more severe injury were more likely to permanently leave work [10].
In previous studies, researchers considered the severity of injury or disability as a variable for predicting RTW and consistently showed that it is a negative predictor for RTW across different types of injury [11–15]. Many studies also explored other predictors for RTW [11, 16–20]. For example, old age, low educational level, low income, absence of strong social supports, psychological problems, and physically demanding jobs were found to be significantly associated with the low rate of RTW. However, only few studies tried to explore the predictors for RTW in sub-populations according to the severity of disability, namely, mild, moderate, and severe.
The overall RTW rate should also be determined to predict patient prognosis. Henschke et al. [21] described the rate of work capacity recovery through a Kaplan-Meier survival curve. The RTW rate significantly increased during the early stage after injury, but the increase faltered during the later stage in patients with low back pain. Steenstra et al. [22] also found similar tendency of RTW in their study, but the RTW rate was different. Nevertheless, studies on the RTW time line in patients with different severities of disability, particularly among Chinese patients with work-related injury, are limited.
In this study, we divided patients into three groups according to the grade of disability, namely, mild, moderate, and severe, based on the compensation recommendation of the Regulations of Worker’s Compensation Insurance in China. This study aimed to show the RTW tendencies and explore the factors associated with RTW in work-related injury patients with mild, moderate, and severe disability within one year after discharge in China.
Methods
Study design
We retrospectively reviewed the medical records of all patients with work-related injury who were admitted to Shanghai Yangzhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), which is the biggest rehabilitation hospital in Eastern China, from January 2012 to December 2014. In the recent 5 years, this hospital received the majority of patients with work-related injury who required rehabilitation services in Shanghai. Patients were included in the study if they met the following criteria: (1) work-related injury recognized by the Shanghai Municipal Human Resources and Social Security Bureau (MHRSSB); (2) first admission to the hospital; (3) 1-year follow-up record after discharge; and (4) had record-related disability grading. Patients were excluded according to the following criteria: (1) the planned rehabilitation service was not completed and (2) death. This study was approved by the Departmental Research Committee of Rehabilitation Science Department of the Hong Kong Polytechnic University (Reference Number: HSEARS20160104001) and the Research Committee of Shanghai Yangzhi Rehabilitation Hospital (Reference Number: YZ2016-097).
Data collection
When patients with work-related injury are admitted to the hospital, the doctors submit a plan of rehabilitation program for each patient to the Shanghai MHRSSB. Thus, any expenses spent in the hospital will be paid by the government. After discharge, the patients’ companies are required to submit an application for disability severity grading to the Shanghai MHRSSB, and social workers will follow-up each patient for one year through structural telephonic interviews and record patients’ work status and grade of disability electronically. In general, each patient can complete the grading process of disability in one year after discharge.
After eligible patients were included in the study, two researchers collected data on potential predictive variables and follow-up results from the electronic files. All predictive variables were patients’ status and condition on discharges. The two researchers extracted all important information and inputted them into an Excel form. Any disagreements between the two researchers were resolved through discussion. All patient information was deemed confidential, and only the related researchers had access to the data.
Predictive variables
The following are the potential predictive variables for RTW: (1) age (years); (2) sex (male/female); (3) registered address (local/non-local resident); (4) marital status (single/married); (5) educational level (primary school or below/junior high school/senior high school/college or above); (6) types of injuries (upper limb/lower limb/trunk/others); (7) nature of work (blue collar/white collar); (8) employer satisfaction (satisfied/fair/dissatisfied); (9) monthly salary; and (10) expectation to RTW (no/yes).
Many other workers in Shanghai are from other cities. Therefore, the variable registered address (local/non-local resident) was included. Because only few patients reported that they were divorced or widowed, we classified their marital status as single to avoid violating assumption of logistic regression, which is that the numbers among categories should not be significantly different. We classified the types of injury as upper limb injury, lower limb injury, and trunk injury, and regarded SCI, traumatic brain injury (TBI), and large burn injury as “others” because of the small number of cases of these injuries.
In terms of job, patients whose works frequently involve repetitive tasks with long period and heavy load were defined as blue-collar workers, while those whose works involve more paper work and less laborious tasks, i.e., clerical and managerial jobs, were defined as white-collar workers. Except for the nature of work, the patients’ monthly salary was also included. Patients were asked a few questions before discharge, including their employer satisfaction with respect to the management of work-related injuries. Employer satisfaction was defined as the patient’s overall feelings about their employers, regardless of the reasons causing satisfaction or dissatisfaction. Patients rated their overall level of employer satisfaction using a three-point Likert scale. In this scale, “one” and “three” represent “dissatisfied” and “satisfied,” respectively, while “two” is the midpoint and means fair. The second question is whether they have an overall expectation to RTW in the following one year based on their own current context, regardless of whether it is the previous job or a new job. The options were “Yes” or “No”.
Follow-up outcome
After discharge, social workers followed up each patient over the telephone. Two core questions are asked during follow-up. The first one is the result of disability grading. In China, the severity of disability is identified according to the work ability identification guideline for employees with work-related injury (version 2014), which was released by the Ministry of Human Resources and Social Security of the People’s Republic of China. The guideline specifies the principles and grading standards for work disability appraisal. The grading score follows a ten-point scale, and a high score indicates mild disability. The principles of grading combine the status of organ impairment, functional limitations, medical dependence, and independence in performing activities of daily living. The Regulations of Worker’s Compensation Insurance divides patients into three groups following the grading score, namely, mild, moderate, and severe. Patients graded between seven and ten are regarded to have mild disability, indicating a strong potential to RTW. Patients with scores between five and six are regarded to have moderate disability, and employers are required to provide appropriate job positions for them after their rehabilitation. Patients with scores between one and four always have severe disability, and the Work Injury Insurance Fund offer compensation to them to cover their daily expenses. Because this grading system is a nationally used tool to evaluate the severity of disability in patients with work-related injury, the rehabilitation providers and other clinical practitioners can refer to the result of grading to classify patients into mild, moderate, and severe disability groups. In most patients, the grade of disability can be assessed within one year after discharge by experts from the Shanghai MHRSSB. Therefore, we adopted this grading system.
Another important factor is work status. We defined RTW as patients being able to consecutively work for one month after discharge. If the patients could not RTW for one month until one year after discharge, we defined them as U-RTW. If patients returned to work successfully in one year, the time since discharge to the first day they returned to work was also recorded by social workers.
Statistical analysis
All continuous variables were expressed as mean±standard diversion, while all categorical variables were expressed as number (n) and percentage (%). Kolmogorov-Smirnov test was used to check normality for each continuous variable. To compare differences in continuous and ordinal variables among the three groups, the Kruskal-Wallis test was used because all continuous variables did not have a normal distribution. Chi-square test was performed to ascertain the presence of significantly different proportions on categorical variables between the three groups. Multiple logistic regression with enter method was performed to determine significant factors related to RTW based on the overall patient population and the three groups. The level of statistical significance was set at 0.05. All statistical analyses were performed with SPSS package (IBM Corp. version 20.0 for Windows).
Descriptive analysis of patient characteristics among the mild, moderate, and severe disability groups
Descriptive analysis of patient characteristics among the mild, moderate, and severe disability groups
SD: standard deviation; RTW, return to work;
*: p < 0.05
**: p < 0.01.
Demographic data of the entire patient population
A total of 752 electronic medical records were screened. Of these, 495 cases were work-related injuries and recognized by the Shanghai MHRSSB. However, data on the grade of disability and work status was missing in 38 patients (13.0%). Finally, 457 patients comprising 337 males (73.7%) and 120 females (26.3%) were included into the statistical analysis. Among the patients, 314 were non-local residents (68.7%) and 143 were local residents (31.3%). In addition, 385 patients (84.2%) were blue collar workers, while 72 patients (15.8%) were white collar workers. The site of injury was classified into four types, namely, upper limb injuries (168 cases, 36.8%), lower limb injuries (141 cases, 30.9%), trunk injuries (43 cases, 9.4%), and others (SCI, TBI, and burn) (105 cases, 23.0%). The average age of included patients was 38.0±10.8 years. The characteristics of the included patients are shown in Table 1.
In terms of grade of disability, 289 (63.2%), 98 (21.4%), and 70 (15.3%) patients were graded between seven and ten (mild disability), five and six (moderate disability), and one and four (severe disability). However, some patients’ data on marital status (n = 38), educational level (n = 71), satisfaction with employer (n = 85), previous salary (n = 96) and expectation to RTW (n = 79) were missing. The main reason might be the staff did not input these data into the electronic hospital information system.
Comparisons of the demographic characteristics among the three groups
Analysis showed that the mild and moderate disability groups had more patients with upper and lower limb injuries, while the severe disability group had more patients with other types of injury (SCI, TBI, and burn) (p < 0.001) (Table 1). Employer satisfaction was also significantly different among the three groups (p = 0.017). Patients in the mild disability group had the highest educational level among the three groups (p = 0.004). A high proportion (64.9%) of patients in the mild disability group expected to RTW (p < 0.001). However, the remaining variables were not significantly different among the three groups.
RTW status
At one-year post discharge, 238 patients (52.1%) had returned to work successfully. In these 238 patients, the average time from discharge to RTW was 85.9±63.7 days, and the median time was 240 days. The number of patients returning to work in the mild, moderate, and severe disability group was 192 (66.4%), 40 (40.8%), and 2 (2.9%), respectively, indicating significant differences (p < 0.001) (Table 2). The tendencies of RTW in the mild, moderate, and severe disability groups are shown in Fig. 1. Through visual inspection, we found that approximately 200 days was the break point that separated significant increase in RTW in the early stage post discharge and the slow increase in the later stage post discharge.
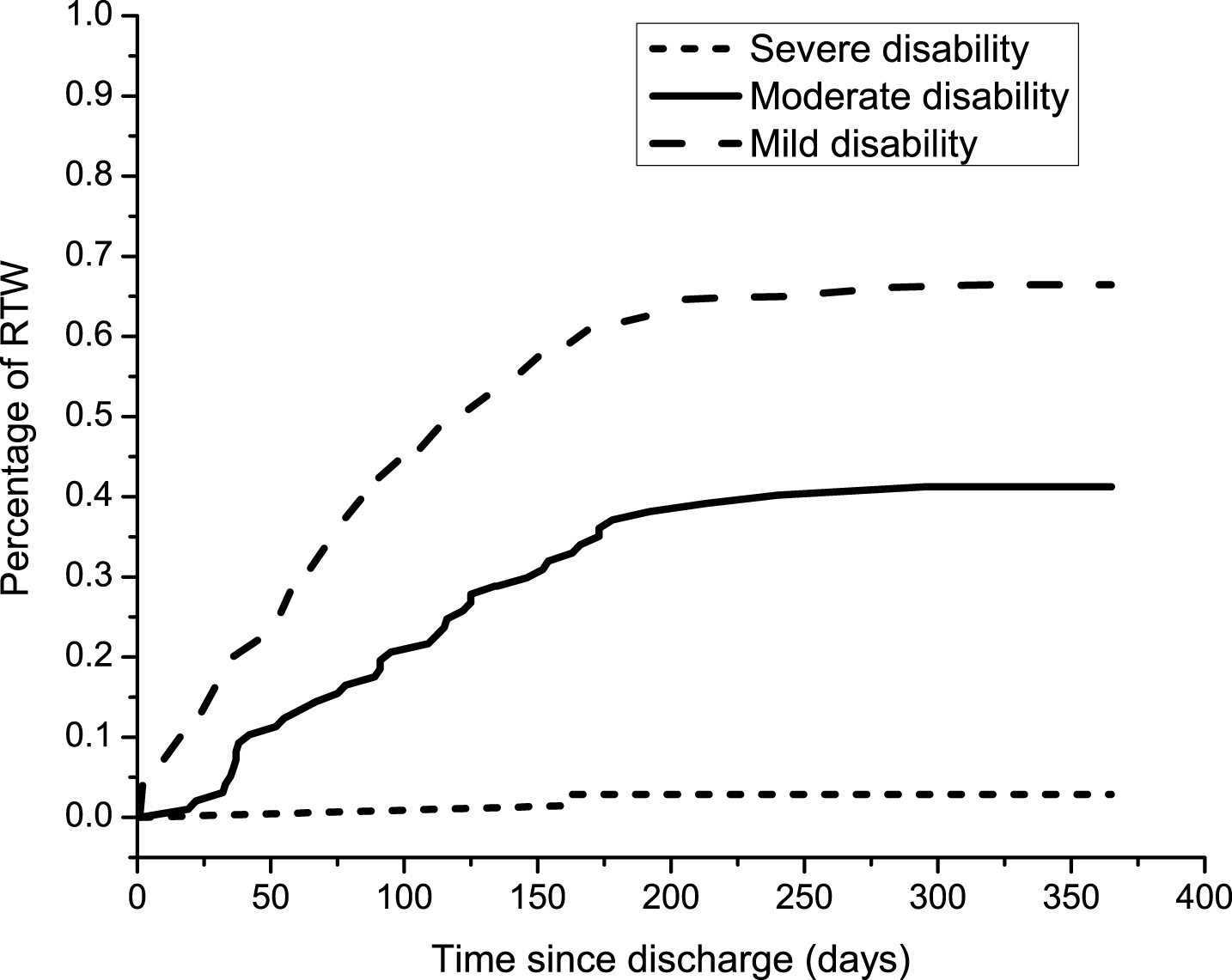
Post-discharge RTW tendency in patients with work-related injury. This figure illustrates the RTW tendency in the three groups, namely, the mild disability, moderate disability, and severe disability groups, that is represented in three different lines in the figure. In this figure, the X-axis indicates time since discharge until the end of follow-up (365 days). The Y-axis indicates the percentage of RTW. The percentage of RTW in the three groups increased until a breakpoint of approximately 200 days. After the breakpoint, the rate of RTW in the three groups plateaued until the end of follow-up.
All patients (n = 340) with complete data were included in the logistic regression analysis (Table 3). The results showed that employer satisfaction and severity of disability were two significant predictors for RTW in the entire study population. In addition, the other types of injury (SCI, TBI, and burn) was also a significant predictor for RTW when upper limb injury was the reference category.
Predictors for RTW in the mild, moderate, and severe disability groups
Logistic regression analysis was performed in each group. A total of 231 patients with mild disability were included in the logistic regression model to determine the significant predictors for RTW. The results indicated that high educational level and expectation to RTW were two significantly positive factors for successful RTW in patients with mild disability (Table 4). Other types of injury had a negative influence on RTW in the mild disability group. Only 69 patients with moderate disability were included in the logistic regression model, and the results showed that white collar and better employer satisfaction were two positive factors for RTW. In the severe disability group, only two patients returned to work, and logistic regression analysis showed no factor was significantly related to RTW.
RTW status of patients in the mild, moderate, and severe disability groups
RTW status of patients in the mild, moderate, and severe disability groups
RTW: return to work;
**: p < 0.01.
Predictors for RTW in the overall study population (n = 340)
RTW, return to work; OR, odds ratio; CI, confidence interval.
Predictors for RTW in the mild, moderate, and severe disability groups
SD: standard deviation; SCI, spinal cord injury, TBI, traumatic brain injury; OR, odds ratio; CI, confidence interval;
*: p < 0.05;
**: p < 0.01.
This is the first study to show the RTW tendencies and explore different factors associated with RTW in patients with work-related injury in China. The RTW tendency graph shows that the RTW rates in the mild and moderate groups maintained a rapidly climbing tendency in the early post-discharge stage. Approximately after the 200th day since discharge, the RTW rate plateaued until the end of follow-up, indicating low possibility of RTW after the 200th day. Because different types of injury were combined in our patient sample, the RTW rate in the current study was not comparable with the results in previous studies that included only specific types of injuries [23, 24].
The period from injury to discharge was not shown in the RTW tendency graph because all patients underwent a similar process and had a comparable time from injury to discharge in the study. Even though we did not consider the time interval from injury to discharge, the average time (85.9±63.7 days) since discharge to RTW seemed to be longer in our study than that in other studies [25, 26]. One of the reasons could be the higher number of patients with severe injuries in our cohort than that in previous studies; for instance, the majority of hand injuries was caused by mechanical compression that usually results in severe hand crush injury. More severe injury usually means longer time for recovery. Furthermore, a complicated process of work capacity identification and compensation might also delay the patients’ RTW plan because several patients were not willing to RTW until they were compensated.
The demographic characteristics of the patients in the mild, moderate, and severe disability groups were markedly different. We found that the majority of our subjects were blue collar workers, while more patients in the mild disability group were white collar workers and had the highest educational level among the three groups. Patients in the mild disability group also had better residual work capacity; hence, they have strong confidence and high expectation to RTW. A previous study indicated that people with high educational level tended to be employed for professional or managerial work (white collar) [24]. Ozegovic et al. [27] further confirmed that socioeconomic and injury-related factors were associated with expectations for RTW in patients with work-related injury. Moreover, the expectation to RTW can reflect the patients’ psychological status because patients usually integrate various information related to their work, injuries, and personal context and decide whether they can RTW immediately [28]. Sometimes, a weak expectation to RTW may not be only due to functional capacity or physical disability, but also due to other reasons. For example, patients may have already considered quitting their jobs prior to the injuries or have a poor relationship with their employers or colleagues; thus, the injury might be an appropriate reason for quitting the job [17]. In addition, we found that educational level, types of injuries, and expectation to RTW were significant predictors for RTW in the mild disability group. As such, patient prognosis may be more precisely predicted if it is based on the predictors from a subdivided population instead of that in the whole population.
For moderate disability patients, the nature of work and employer satisfaction were significantly associated with RTW. The tasks of white-collar employees usually do not involve physically demanding tasks while that of blue collar employees are usually physically demanding. Physical capacity was more significantly reduced in patients with moderate disability patients than in those with mild disability. Furthermore, the disability in some patients with moderate injury might be permanent. In such cases, physically demanding work becomes more challenging for moderate disability patients. This is why nature of work is among the important predictors for RTW. Employer satisfaction is the patients’ psychological reflection about their employer’s management of their injuries. Patients are usually dissatisfied with their employers due to the employer’s passive attitude on the management of their injury. In our institution, patients with work injury may complain that their employers do not have an active attitude in their clinical treatment and even do not visit them at the hospital. Although the insurance law stipulates that the salary of employees with work injuries should remain the same, some employers still default the patient’s salary because of the decreased employee productivity post injuries. Therefore, policy makers should be involved. Another reason for poor employee-employer relationship is the patient’s poor communication skills. For example, patients cannot appropriately express their needs and requests to their employers. An inharmonious relationship between patients with work injury and their employers will strongly affect the patient’s decisions about RTW. By contrast, a harmonious relationship and good employer satisfaction will be advantageous when patients decide to RTW as soon as possible. To promote RTW, patient education about maintaining a good relationship with their employers may be necessary in occupational rehabilitation practice.
No significant predictors for RTW were determined in the severe disability group because only two patients returned to work successfully in the one-year post discharge. TBI and SCI were comprised the largest number of injuries in the severe disability group. The RTW rate for patients with severe brain injury in our study was lower compared with that of previous studies [29, 30]. In the severe disability group, the majority (90%) of patients were blue collar workers, and very few of them (8.9%) had educational level of college or above. These demographic features could be the barriers for RTW. However, we also have to note that the job of these two patients who returned to work were flexible and they had huge supports from their employers and families. These findings may be practical in guiding our vocation rehabilitation service. To facilitate RTW of patients with severe disability, strategies suggested by other authors can be applied, such as comprehensive work-absence management [31], assistive technology supports [32], and training for skills related to physically demanding jobs [30].
This study has some limitations. First, the number of patients included in the moderate and severe group is small; thus, future research with large sample size are needed to explore different predictors for RTW in patients with moderate and severe disability. In addition, we did consider the time period from the onset of patient’s injuries to discharge, and this may distort the tendency of RTW. Future studies should include more baseline variable into analysis to make the results more comprehensive and helpful for clinical practice.
Conclusion
Although our study has some limitations, we provided baseline information on the RTW tendency of patients with work-related injuries in China. We showed that the rate of RTW rapidly increased during the early stage post injury but plateaued during the later stage in China. Moreover, the predictors for RTW in the three groups are also different. Educational level, expectation to RTW, and other types of injury (SCI, TBI, and burn) are predictive factors for RTW in the mild disability group, while white-collar work and employer satisfaction are factors for RTW in the moderate disability group. No significant predictors for RTW were found in the in severe disability group.
Conflict of interest
None to report.