
Abstract
BACKGROUND:
Work-related musculoskeletal injuries and disorders (WMSDs) are among the most frequently reported causes of lost or restricted work time in the construction industry. Ergonomics is still a relatively new theme for the construction industry. Understanding of the workers’ and managers’ knowledge and perception of ergonomic issues in construction can play a critical role to develop and implement effective ergonomic programs and policies.
OBJECTIVE:
To study the similarities and differences of the workers’ and managers’ knowledge and perceptions of ergonomics matters in the construction industry.
METHODS:
A survey questionnaire was developed and distributed to both workers and management personnel employed by sixteen different construction contractors performing various types of construction work. The final questionnaire comprised of a total of forty questions and consisted of four major sections: background, safety and ergonomic programs, injuries and illnesses, and work conditions.
RESULTS:
Eighty-eight workers and managers completed the survey questionnaire. Nearly all of their employer had a written safety program, while only one third had an ergonomics program. Ergonomics was perceived as relatively less important compared to the safety issues. Managers were more likely to think that management encourages feedback from site employees than were workers. Managers appeared to be more likely to know that their companies have an ergonomic training program or policy than were workers. Workers were more likely to consider to purchase or select the ergonomic hand tools than were managers. Workers and managers alike reported having slight regard for the potential occurrence of a work-related musculoskeletal disorder.
CONCLUSIONS:
While the construction industry has done an admirable job developing safety programs, it has done far less to develop comprehensive ergonomic programs and policies that would help provide education and guidance to its workers and managers in the industry.
Introduction
The construction industry has an unenviable history of having one of the highest work related injury rates among all industries in the United States [1]. Construction workers repetitively lift, stoop, kneel, twist, grip, stretch, reach overhead, or work in other awkward positions putting them at risk of developing musculoskeletal problems [2]. Work-related musculoskeletal disorders (WMSDs) involve the muscles, nerves, tendons, joints, cartilage and supporting structures of the upper and lower limbs, neck and lower back; they are caused, precipitated or exacerbated by sudden exertion or prolonged exposure to physical factors such as high force, repetition, awkward body posture or vibration [3]. In a 2015 report by U.S. Bureau of Labor Statistics [1], musculoskeletal disorders accounted for one-third of the total days-away-from-work cases such as sprains/strains resulting from overexertion in lifting [1]. The costs associated with musculoskeletal injuries and disorders to the construction industry are staggering. The Liberty Mutual Workplace Safety Index showed that overexertion and repetitive motions accounted for direct workers’ compensation costs of roughly 21 billion dollars. The category of overexertion which included injuries related to lifting, pushing, pulling, and holding, carrying, or throwing cost businesses over $15 billion in direct costs and accounted for nearly a quarter of the overall national burden [4].
Ergonomics, fitting the job task to the worker, is still a relatively new theme for the construction industry [5]. Ergonomics has many different meanings within the industry, and generally construction workers hold the belief that WMSDs are somewhat inevitable or acceptable as part of the job [6]. Training for ergonomic hazards in the construction industry can be complicated. Unlike other construction work related hazards, ergonomic hazards tend to be more occupation/trade specific [7]. Construction craft workers are exposed to specific ergonomic hazards. Likewise, their training to avoid WMSDs also needs to be specific. Knowledge of newly designed ergonomically correct tools and methods are not easily spread throughout the construction industry. The industry is fragmented, making it difficult to spread ideas from one geographical location to another [8]. Most ergonomic improvements that have a positive impact on workers’ health have some amount of monetary cost. For companies to maintain their desired profitability, these costs need to be recovered. Companies generally will not invest in an ergonomic improvement unless it improves productivity and increases profits, which makes it difficult for the introduction of innovative ergonomic solutions into the workplace [9]. Larger companies were more likely to address ergonomic issues through training than smaller ones believing that larger companies typically have more financial resources available to them to allocate for training [6, 9].
Management’s commitment to safety and ergonomics is invaluable to the success of these programs [10]. Managers establish priorities that determine an organization’s policies, procedures, and goals. Their commitment can manifest itself through job training programs, management participation in safety committees and consideration of safety in the job design and tasks [10]. The workers’ perceptions of management’s and co-worker’s commitment to ergonomics and safety may be equally as important to the program’s success as the commitment itself [11, 12]. Employees working for a company or supervisor that rarely or never mentions ergonomics will likely form the perception that ergonomics is unimportant and as a result place less emphasis on it [13].
The purpose of this survey study is to identify the similarities and differences of the knowledge and perceptions of ergonomic matters between workers and managers in the construction industry.
Material and methods
Survey instrument
Prior to developing the study’s survey questionnaire, the authors reviewed multiple resources that included peer-reviewed articles and journals, magazines, existing ergonomic related surveys, and websites in order to obtain an understanding of the ergonomic issues that face the construction industry. The review of multiple sources guided the authors to develop this study’s questionnaire sections (4 parts), particularly based on a previous model by Choi [7, 14]. Next, a pilot survey questionnaire was developed and consisted of four major sections consisting of: (1) background information about participants (n = 10 items); (2) safety and ergonomic programs (n = 20 items); (3) work-related injuries (n = 6 items); and (4) work conditions (n = 5 items). The first “background” section consisted of questions concerning the survey participant’s work title, job function, and length of employment, race, gender and union affiliation. This section also asked a number of questions concerning the participant’s employer including their current employer’s total employment, its duration in business, and the type of safety training it or the participant’s union affiliation offered. The next section, “safety and ergonomic programs”, focused on the participant’s employer’s safety and ergonomic program. The section questioned whether their employer had written ergonomic and safety programs, the length in which the programs were in place, and if and what type of ergonomic training was offered. By asking these questions the survey’s data could be analyzed to determine the size and type of construction companies that had ergonomic programs. An ideal ergonomic program would address hazards specific to the company’s particular work tasks. An ergonomic process should utilize the principles of a safety and health program to address work-related musculoskeletal hazards, as an ongoing function incorporated into the daily operations rather than as an individual project [15]. The section also inquired about the content of their employer’s ergonomic program and policies. Did the company have a manual lifting weight limit? What types of PPE’s were available? There were also questions concerning the participant’s perception of the employer’s management commitment to safety as well as to ergonomics. The third section, “Injury and Illness”, listed six types of work related injuries and illness that commonly occur in the construction industry [14, 16] and asked to the participants to choose the injury or illness that they felt occurred the most frequently while completing their specific job task or function. The section also asked the participants to rank a predetermined list of seven body parts in which the participants felt were most commonly injured with (1) one being the “most frequent” and (7) the “least frequent”. The final section titled, “Workplace Conditions”, focused on the conditions the survey participants’ encountered while at work with their current employer. The section had questions concerning the type of work surfaces the participants were exposed to, the type of tools the participants used to complete their tasks, the types of ergonomic hazards they were exposed to while at work, as well as a number of specific questions concerning daily manual lifting expose including the amount of time spent manually lifting, the distance the object needed to be carried, and the actual weight of the object they were required to lift.
Procedures for gathering data
The questionnaire was pilot tested to ten construction workers and managers that were working on an industrial construction project located in the Southern U.S. The participants in the pilot study included three carpenters, two managers, two electricians, one concrete finisher, one laborer, and one equipment operator. The participants were asked to provide comments on the content, the delivery method and the comprehensibility of the survey. The participants in the pilot study reported that they felt the survey questions were understandable and also felt delivering the survey in person would enable the participants to ask questions if they needed a question clarified. Ultimately, the feedback resulted in minor grammatical modifications to the survey questionnaire. The final survey questionnaire was then distributed to workers and managers working at the same industrial construction project in which the pilot survey was tested. The survey questionnaires were administrated from July 2015 through December 2016.
The industrial project was constructed on a 10 acre footprint located within an existing chemical facility. The facility housed a number of chemical plants, each utilizing byproducts or products of other plants within the facility. The project was considered a green field construction project, meaning that there were no existing structures or utilities present on the 10-acre site. The facility housed a conglomeration of chemicals plants. The 10 acres were within the facility but not within an existing plant. The 10 acres were accessed through the facility’s walking paths and roadways, outside the perimeter of existing plants within the facility. The project contractors completed a wide range of work. The contractors completed tree removal and grubbing, mass grading and excavation. They erected structural steel and placed pre-cast concrete wall panels. They installed underground utilities, auger cast concrete pilings, concrete foundations and flooring, flare stacks, cold storage units, tanks and vessels, mechanical, electrical, fire protection systems, and asphalt roads. The two-year project had a peak employment of 385 personnel. The project employed skilled and unskilled craft, project and construction managers, with an onsite support staff that included engineering, scheduling, project controls, documentation, procurement, receiving, estimating, health and safety, and environmental employees. Upon final completion and commissioning, the four story chemical plant will produce a herbicide product for the commercial and residential agricultural industry.
Data analysis
The survey participants were not asked to provide their name nor their employer’s name to ensure confidentiality. The responses of the workers (tasked to perform physical construction activities) and management personnel (assigned supervisory responsibilities of a general foreman or higher) categories were tallied and compared to one another. Statistical analysis for descriptive statistics and Pearson’s chi-square tests of the data were conducted using SAS® (Statistical Analysis Software) 9.3 Software. SAS® is an analytics software suite developed by SAS Institute Inc., Cary, NC, USA.
Results
Of the one hundred three surveys that were distributed, 88 completed the survey. The results of the survey were broken down per the survey format of Background, Safety and Ergonomic Program, Injury and Illness, and Work Conditions. The results of the survey are as follows.
Background
Table 1 lists the surveyed characteristics of the participants’ reported background. The majority of the respondents were male (98%). About three-fourths of the workers were white, followed by African Americans (17%), Latinos (6%), and others (3%). They ranged in age from 18 to 69 with a median age of 39. The range of the participants’ current company employment length was 0 to 27 years, with a median of 1 year and 8 months. Seven participants reported that they were union members while forty-six participants were not. Sixty of the eighty-eight participants were workers while twenty-eight were managers. The job titles/functions of the workers were: carpenter (12), iron worker/rigger (11), rodbuster/rebar install (8), equipment operator (7), helper (6), electrician (4), sheet metal (2), painter (2), mechanical (2), engineer (1), truck driver (1), sales (1), mason (1), scaffold builder (1), and civil (1). The job titles/functions of the managers were: supervisor (8), foremen (7), safety (5), superintendent (3), project manager (3), and manager (2). The survey participants were employed by sixteen different contractors: a general contractor, two electrical contractors, an auger piling contractor, a block masonry contractor, a roofing contractor, a mechanical contractor, an HVAC contractor, a fireproofing contractor, a painting contractor, a scaffold erection contractor, an insulation contractor, a floor coating contractor, a rebar installation contractor, an industrial floor contractor, and an engineering/design/construction management. The size of the participant’s employers ranged from 17 to 44,000 employees. Eighty-one percent (71 of 88) reported that they had some types of safety training offered by the company or union. Most frequent type of safety training was OSHA training (49), followed by fall protection (22), confined space (11), basic safety training (8), and manual lifting/ergonomics (8).
Background characteristics
Background characteristics
The “Safety and Ergonomics Programs” section of the survey contained questions concerning the participants’ knowledge of their employers’ safety and ergonomic programs. Table 2 presents the survey results. The participants were asked if they knew if their employer had a written safety program; 95% responded yes, while only 37% stated that their employer had an ergonomics program. Of the respondents stating that their company did not have an ergonomics program; none replied that they knew if their employer had a plan to develop one. Only about one-third of the participants reported that their company or union-provided ergonomic training and that they had received ergonomic training specific to the task they perform. The participants were asked if they knew how to perform an ergonomic assessment, only 27% reported that they did. And about 23% of respondents stated that an ergonomic evaluation had been completed on the task they perform. Approximately half of the participants stated that there was a stretching or flex exercise policy at work and they stretched prior to work. Fifty-three percent considered purchasing/selecting ergonomic handle of power tools. Roughly two-thirds stated that they had a manual lifting training program and that they had a weight limit on single person manual lifting. Most of the limits were 36–50 pounds but 14% reported above 50 (55–100) pounds. Only 21% stated that they have work practices or personal protective equipment (PPE) for vibrations. A construction worker’s perception of their management’s concern for their workplace safety is vital to the success of an organization’s ergonomic programs and safety programs. When asked how many dedicated full time safety professionals were employed by the participants’ company, 64% (56 of 88) were unsure or did not enter an amount. While 45% responded that the company had a safety team/committee, only 4% stated that their employer had an ergonomic team/committee.
Safety and ergonomics programs
Safety and ergonomics programs
The survey asked the participants to rank their perception of their company’s safety and ergonomics issues on a scale of 1–5 with “1” labeled as “not important” and “5” labeled as “extremely important”. The following questions were answered by the participants:
Does management express concern if safety procedures are not adhered to? Does management encourage feedback from site employees? How is “Safety” perceived in your company in terms of importance? How is “Ergonomics” perceived in your company in terms of importance?
Figure 1 shows the participants’ responses. The average scores and their standard deviations (SD) for those questions were 4.83 (SD = 0.47), 4.69 (SD = 0.63), 4.96 (SD = 0.24), and 4.10 (SD = 1.11), respectively. The respondents overwhelmingly perceived that their employers were concerned for their workplace safety. However, the participants’ perception of company’s ergonomic well-being was ranked much lower than their perception ranking of company’s safety concerns. Only 50% (34 of 68) thought it was extremely important (“5”) to their employer. It clearly shows that ergonomics is perceived relatively less important compared to the safety issues (management express concern; management encourage feedback; “Safety” perception).
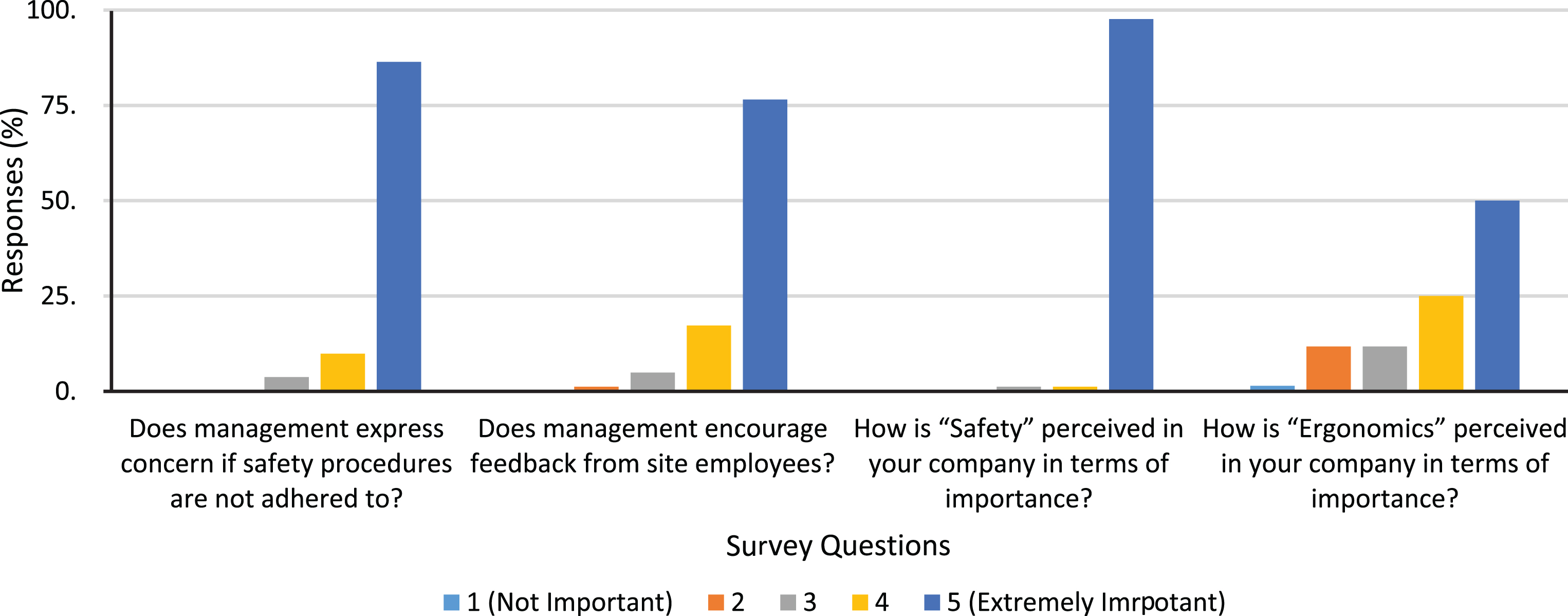
Participants’ perception of safety and ergonomics programs.
When the study’s survey responses were separated into Management vs. Worker categories the comparisons suggested interesting findings. Chi-square tests of independence were performed to examine the relation between manager/worker and the survey results. The relations between these variables were significant for the following cases (see Table 3):
Different responses of managers vs workers – safety and ergonomics programs
1* (not important); 5†(extremely important).
Managers appeared to be more likely to know that their companies have a manual lifting training program than were workers, χ2 (2, N = 85) = 3.4235, p = 0.1805.
Managers were more likely to think that management encourages feedback from site employees than were workers, χ2 (3, N = 81) = 9.6843, p = 0.0214.
Workers were more likely to know that their companies have a stretching or flex exercise policy than were managers, χ2 (2, N = 86) = 5.9337, p = 0.0515.
Workers were more likely to know that their employees do stretches prior to the beginning of their shift than were managers, χ2 (2, N = 84) = 9.2215, p = 0.0099.
Workers were more likely to consider to purchase/select the ergonomic handle of power tools than were managers, χ2 (2, N = 83) = 7.1280, p = 0.0283.
Workers appeared to be more likely know that their companies have work practices or PPE for vibrations than were managers, χ2 (2, N = 86) = 4.3016, p = 0.1159.
The “Injury and Illness” section of the survey contained questions concerning the participants’ awareness and perception of workplace injuries. The participants were asked if they knew how many non-fatal injuries and illnesses had at occurred at their respective employer in the past year. They were also asked how many recordable injuries and illnesses had occurred during the same timeframe. Just 17% reported that they were aware of how many non-fatal injuries had occurred and only 13% stated that they knew the total number of recordable injuries.
The participants were asked to choose from a list of commonly occurring injuries in the construction industry that most frequently afflicted workers in the participant’s specific line of work. As shown in Fig. 2, the choices included “sprain/strain”, “back injury”, “fractures”, “burns”, “cuts”, “carpal tunnel syndrome”, or “other(s)”. The participants were allowed to choose more than one injury category from the list. Sprain/strain was chosen by 44% of the participants, back injuries 43%, cuts 42%, carpal tunnel 14%, burns 9%, and fractures 3 %. Written into other(s) were hand injuries (8%), shock (1%), and puncture (1%).
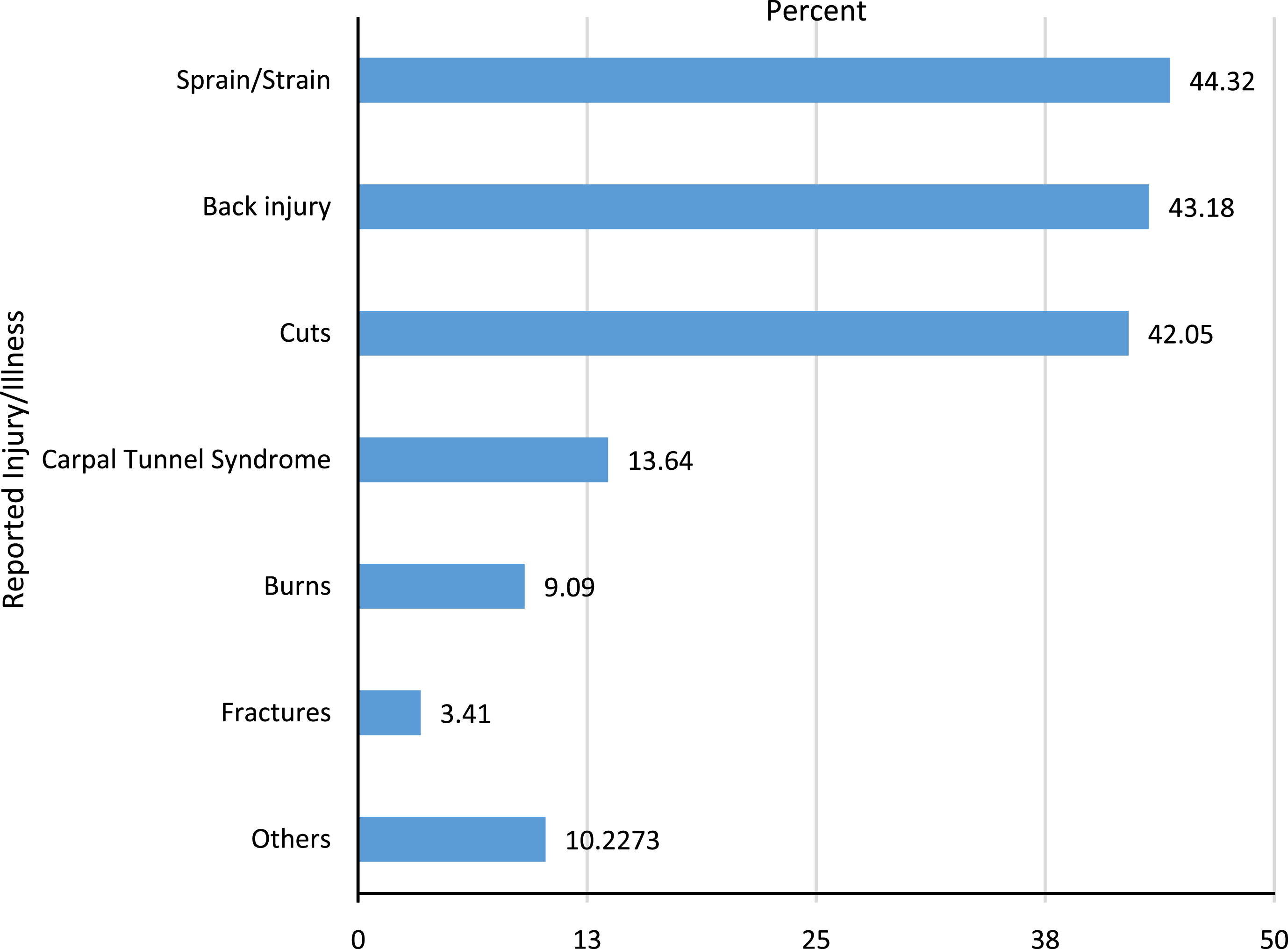
Most frequently occurring injuries/illnesses – survey results.
The participants were then asked their perception of the possible causes of the injury or illness in which they had chosen. They were given the choice of “overexertion,” “motion/position,” “slip/trip/fall,” “tools/machinery,” “chemicals,” or “other(s)” in which they could write the cause. Once again, the respondents were allowed to choose multiple categories. As shown in Fig. 3, “motion/position” was chosen by 44% of the participants, “slip/trip/fall” 42%, “overexertion” 34%, “tools/machinery” 24%, “chemicals” 5%, and “others” had “not wearing proper PPE,” “materials/metals,” “sheet metal,” “sharp objects,” “complacency for the most part,” “not understanding,” and “processes/complacency” written in.
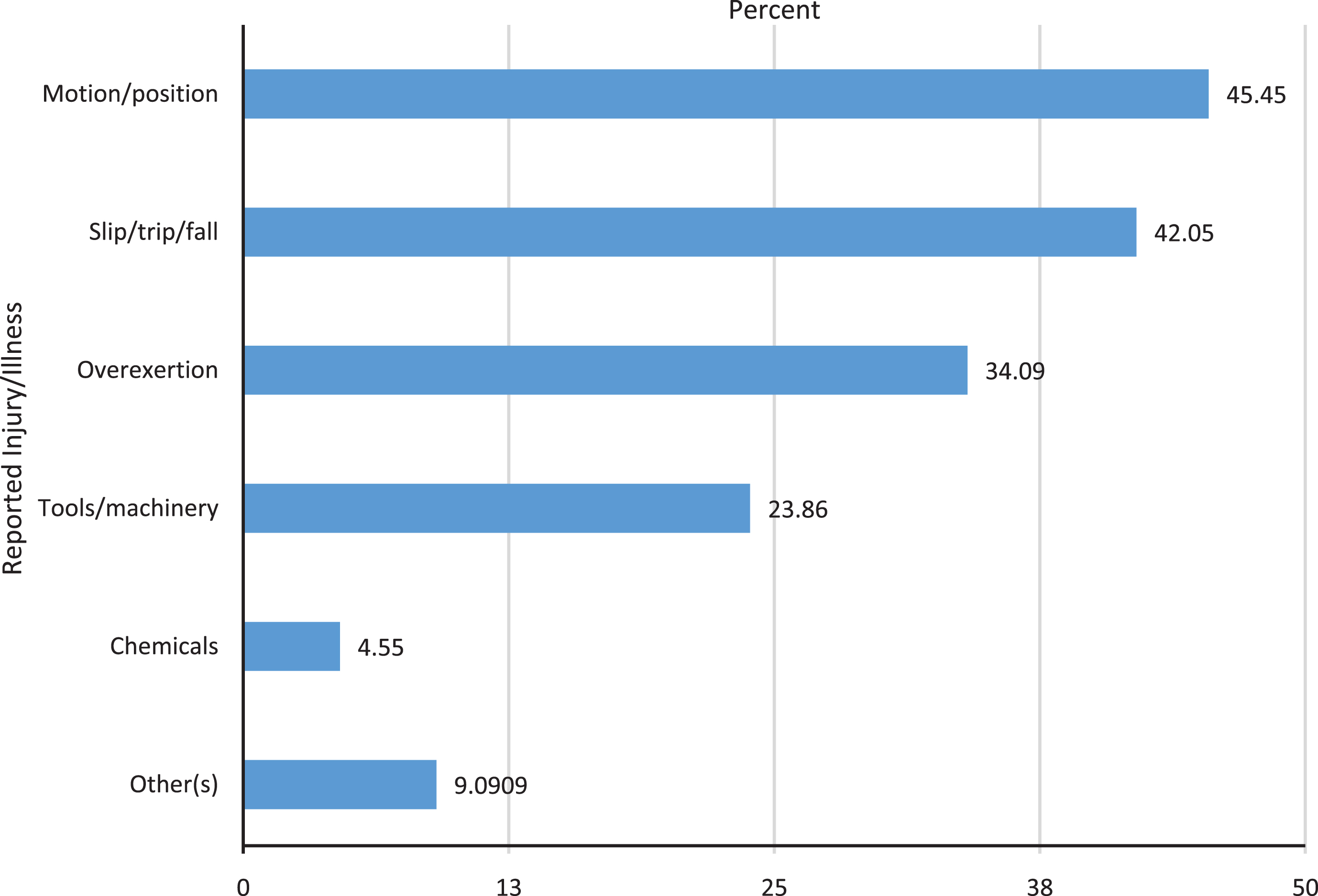
Cause of frequently occurring injuries/illnesses – survey results.
The participants were also asked to rank which body parts were most frequently injured from a list. They were instructed to rank the body parts from “1” to “7” with “1” being the most frequent and “7” the least. The results of the ranking were hand/fingers (median 1, mode 1), back (median 3, mode 3), eyes (median 3.5, mode 2), foot/ankle (median 4, mode 3), knee (median 5, mode 7), shoulders (median 5, mode 7), and head/neck (median 5.5, mode 7). However, workers ranked knees (median 4, mode 1) ahead of eyes (median 5, mode 7). Very few of the respondents had experienced or elected to state that they had sustained a work-related injury or illness or had suffered bodily pain within the last 12 months. Just 2% (2 of 88) stated that they had a lost time injury within that timeframe and only 20% (18 of 88) stated they had experienced body discomfort or pain at work in the past year. The eighteen participants reporting that they had experienced bodily discomfort choose the following body parts as the source of their pain, “back” (5 times), “shoulder” (4 times), “neck” (3 times), “knees” (3 times), “legs” (3 times), “feet” (3 time), “eyes” (2 times), “wrists” (1 time), hands (1 time), ankle (1 time), all (1 time), and general soreness (1 time).
Chi-square tests of independence were performed to examine the relation between manager vs. worker. The relations between these variables were significant for the following cases (see Table 4): Workers were more likely to get back injuries in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 7.9204, p = 0.0049. Workers appeared to be more likely to get sprain/strain in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 1.2319, p = 0.2670. Workers were more likely to get injuries due to overexertion in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 9.9878, p = 0.0016. Workers appear to be more likely to get injuries due to motion/position in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 1.5714, p = 0.2100. Workers appear to be more likely to get injuries due to tools/machinery in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 2.0735, p = 0.1499. Workers appear to be more likely to get injuries due to chemicals in the participant’s specific line of work than were managers, χ2 (1, N = 88) = 1.9556, p = 0.1620.
Different responses of managers vs workers – injury and illness
The final section of the survey focused on work related conditions. The participants were given seven work surfaces in which they most commonly walked or worked on while completing their job. The participants could choose from more than one surface. The results in order were ground (75%), scaffold (44%), ladder (43%), steel beam (28%), roof (16%), and tree (0%). Written into the choice of “other(s)” were rebar (3%), crane (1%), lifts (1%), loose gravel ricks (1%), grating (1%), elevated metal decks (1%), and all (1%). The top ten commonly used tools the participants utilized to complete their tasks included: grinder (22), hammer (18), drill (15), wrenches (14), pliers (14), shovel (6), screwdriver (6), tape measure (4), knife (4), side cutters (4). This question was “fill in the blank”; participants were able to write in more than one tool. Only 43% (38 of 88) of the participants responded that they felt they were exposed to ergonomic hazards while at work. When the participants were instructed to check all applicable occupational risk factors from a list of choices, they selected (number of participant responses) awkward body postures (34%), high repetition or frequency (27%), excessive manual force (20%), extended task duration (17%), cold temperatures (17%), vibration (13%), as shown in Fig. 4. The participants could check more than one risk factor.
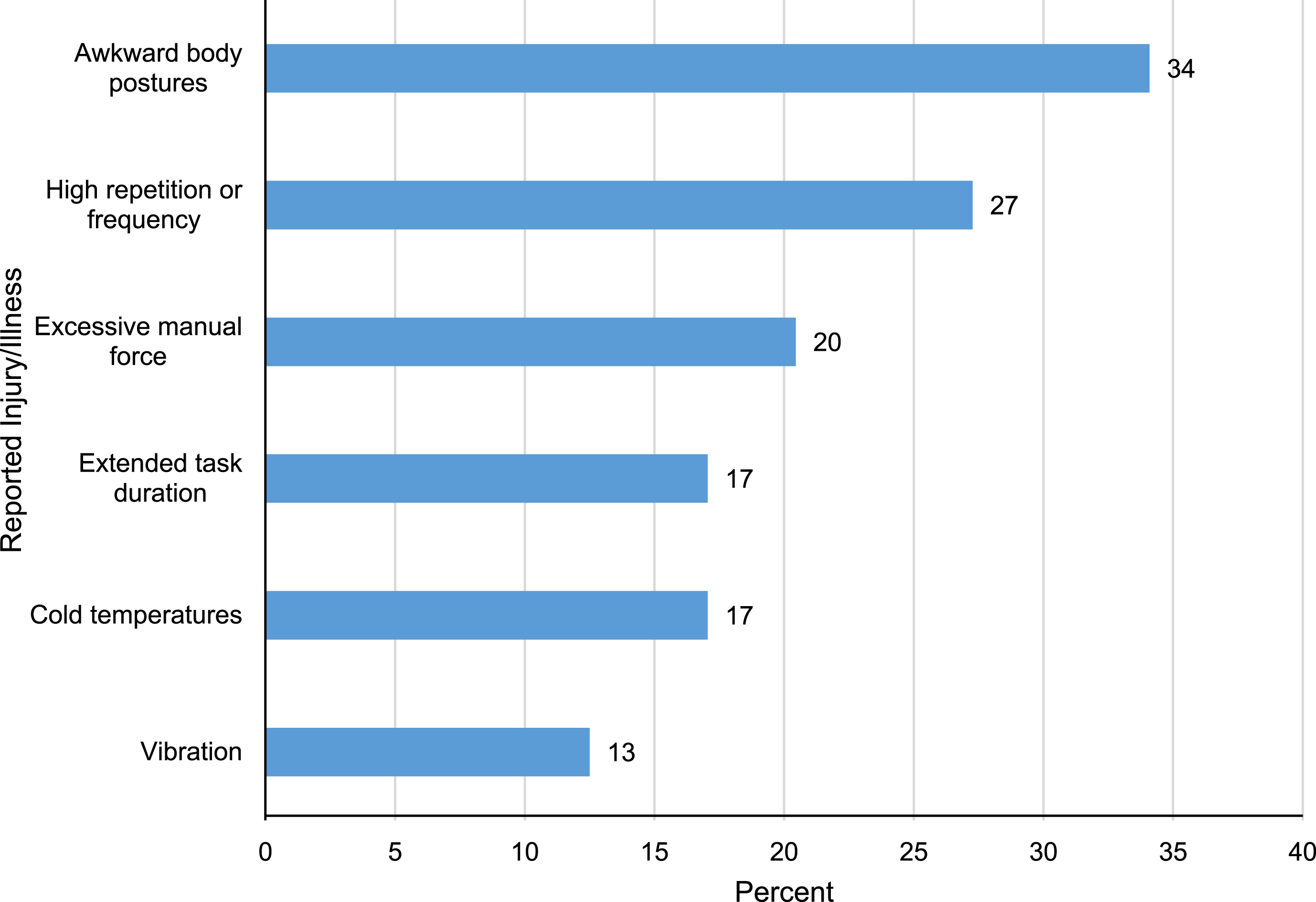
Occupational risk factors – survey results.
The final survey question inquired about the participants’ manual lifting task requirements during a typical work shift. The participants were asked to check off from a list of categories the total time they spent manual lifting during a typical day, the total distance traveled for each manual lift or carry, and the approximate weight of the load they were required to lift or carry. For “total time lifting/carrying”, the category of 1-2 hours was chosen the most (27%), followed by less than 1 hour (25%), 3-4 hours (16%), 5-6 hours (16%), and 7-8 hours (15%). However, managers chose the category of less than hour (42%) and 1-2 hours (33%) more than the other categories, while workers chose all the categories relatively evenly, as shown in Fig. 7. For “total distance traveled”, the categories of <10’ (38%) and 11’–30’ (35%) were overwhelmingly chosen. The 31–50 lbs. category of “approximate weight of the load” was chosen 43%, overwhelmingly the most common response. Ten percent participants choose more than 51 lbs., a weight higher than the NIOSH recommended limit of 50 lbs. Fourteen percent workers reported this high weight of load, while only 4% managers did (Fig. 5).

Different responses of managers and workers – work conditions.
This study was intended to greater understand workers’ and managers’ knowledge and perceptions on ergonomics in the construction industry. The findings of this survey reported that nearly everyone had a written safety program whereas only a third had an ergonomics program. Similarly, in a previous study by Choi et al. [14], all of the companies completing a survey stated that they had a written safety program but only approximately 40% had an ergonomic-related program (e.g., weight lifting restrictions). When this study’s survey responses were divided into management and worker categories the comparisons proved interesting. Most of the participants had knowledge of their employer’s manual lifting training program; 82% of the managers verses 62% of the workers had knowledge on NIOSH lifting guidelines (i.e., approximately 20% fewer workers knew of their employer’s manual weight lifting program than the managers). Perhaps, the workers are learning of their employer’s weight lifting limit by word of mouth rather than a formal training program. Similarly, a study “barriers to adoption of ergonomic innovations in the construction industry” by Glimskar and Lundberg [9] found that employees are willing to participate in programs that prevent severe and fatal injuries but far fewer are willing to appreciate the risks associated with ergonomic hazards.
Managers were more likely to think that management encourages feedback from site employees than were workers. Approximately 93% of the managers participated in this study reported that it is “extremely important” to receive feedback from site employees. When it comes to stretching programs, the difference is participation. More workers will typically stretch prior to work than managers, whose tasks are less physically strenuous and typically more office related. Fewer than half of those surveyed believed that they were at risk for a work related musculoskeletal injury. When the participants were broken into management and workers categories, neither the managers (50%) nor the workers (40%) strongly felt that they had an exposure to WMSDs. Given that less than a half of the participants reported that they are exposed to ergonomic hazards at work, it is no wonder that only about one fourth of the respondents reported that an ergonomic evaluation has been performed on their task. Managers are tasked with developing and implementing health and safety programs at the worksite. If they do not understand or believe a potential hazard exists, they will be far less agreeable to allocate resources to complete a hazard evaluation. Without completing an evaluation, the hazard will never be addressed and workers will continue to be harmed. Management’s support was vital to a safety program’s success. Given that management’s support is critical to a safety program’s success, the workers’ perception of their support and concern is equally as important [10]. The survey respondents’ perception of management’s concern for the safety program was compared to their concern for the ergonomic program. Nearly everyone felt that their management was concerned for the company’s safety program but only a half perceived that their management was concerned for the ergonomic program.
Written programs are the basis for a safety or ergonomic program, the lack of written ergonomic programs appears to be mirrored by the workers’ less than favorable perception of management’s concern for ergonomics. Creating a company culture to effectively address safety and ergonomic hazards begins with management [6]. While it is clear that while the majority of construction companies have written safety programs that have strong management support; it seems that the industry’s management support of ergonomic programs is far less developed. The lack of management’s commitment revealed in the lack of written programs coupled with the workers’ perception of management’s lack of ergonomic program concern maybe contributing to the workers’ apathy towards the probability of an occurrence of a WMSD. Boatman et al. [6] study had similar results concluding that workers were skeptical as to management’s commitment to making the workplace safer and that workers tended to believe that WMSD’s were an acceptable part of the job. The participants in this study had little knowledge of ergonomics as well. Less than one third reported that they had completed some type of ergonomic training. The lack of ergonomic training being offered and completed in the construction industry as well as the imbalance of completed training between management and workers may be contributing the industry’s high frequency rate of WMSDs. It should be noted that there seemed to be a contradiction in the responses to the questions concerning specific ergonomic training and programs compared to those responses to the generalized question of, “have you completed ergonomic training”.
When asked if there were manual lifting programs at work, approximately two-third stated their employer had a manual lifting training program or a manual lifting weight limit. It’s possible that the respondents who completed the specific training did not realize that the training fell under the umbrella of ergonomic training. Still, even if ergonomic training is being under-reported or misunderstood for what it is, with most of the participants believing that they are not exposed to work-related ergonomic hazards additional training seems to be warranted. The participants in this study performed work within sixteen different types of craft trades or tasks. Interestedly, of the twelve carpenters who participated in the study; whose trade has a higher rate of injury and illness than the national average, none reported that ergonomic training had been made available to them. The participants that did report that ergonomic training had been offered to them were concentrated in the iron worker trade and management. Considering a typical iron worker’s job duties, the training that was offered to them almost certainly was construction related while the management participants may have been offered ergonomic training related to office and administrative functions. Individual companies could do more for their employees. Most construction contractors do not provide trade-specific or site-specific ergonomic interventions [7]. Contractors could evaluate their own worksites for ergonomic hazards and then provide project specific training for their employees. Companies could also institute engineering controls, change work processes, and provide their workers with ergonomically correct tools that reduce muscle strain and fatigue. Companies could also institute pre-shift stretching programs that help loosen workers muscles before they start work; they could also encourage workers to take frequent, short breaks to stretch their backs and muscles throughout their workday [5].
As with company health and safety programs, ergonomic programs must have the commitment of upper management to provide not only the financial funding but also the organizational support to make it a success [17]. Money and time must be allocated to provide worker and manager training, complete ergonomic task evaluations, improve work methods, and the proper personal protective equipment. Top management must be apprised of the potential economic costs to their companies and the physical disabilities caused to their workers by ergonomic injuries such as work-related musculoskeletal disorders.
There are some limitations in this study. The survey did not pose questions to ascertain the participants’ level of understanding of construction ergonomics which may have resulted in the surveyed respondents’ misrepresenting their company’s ergonomic programs and policies existence as well as their management’s commitment to these programs. For example, it is possible that some participant’s companies had programs that addressed manual lifting or use of tools that mitigated repetitive motion that certain respondents did not recognize as ergonomic programs. This possible lack of ergonomics understanding, which may have led to workers and managers’ inability to recognize ergonomic programs accurately, invokes the possibility of further investigation. Have construction workers and managers been trained in certain ergonomic programs and misunderstood them to be safety programs? Or, is it possible that the workers and managers’ underdeveloped understanding of ergonomics reflects the construction industry’s lack of quality or absence of ergonomic awareness, programs, and training? While the survey’s participants’ level of ergonomic understanding was not fully addressed, the results of the study do seem to indicate that the construction industry’s workers and managers’ perception and awareness of their company’s ergonomic programs and their company’s leadership commitment to those programs are not in alignment with their perception and awareness of their company’s safety programs.
Conclusions
This study was conducted to survey the similarities and differences of the knowledge and perception of ergonomics between the construction workers and management personnel. Ergonomics was perceived relatively less important compared to the safety issues. Members of neither group were particularly concerned with the potential of a work-related musculoskeletal disability. Both groups had little knowledge concerning ergonomic hazard assessment methods and few reported that they were aware if an ergonomic assessment had been completed for their specific job task. Additionally, a majority of each group reported that they had not been offered nor completed training in ergonomics. The manager’s reports of having substantially less awareness of their company’s stretching program could be the result of the sedentary nature of their job duties while workers, feeling the bodily effects of the daily physical grind required to complete their job tasks, could be more inclined to follow their company policy by performing stretching and warm-up exercises each day. Management personnel’s considerably greater awareness of their employer’s manual lifting program could be based in the workers’ understanding of what constitutes a manual lifting program. It is well documented that management commitment was vital to the success of ergonomic programs. The industry’s top managers and leaders require knowledge that is obtained through training and experience to develop an appreciation for ergonomic risks; only then will they provide the financial and organizational support to address the problem of WMSDs. Upper management must be made aware of the ergonomic issues confronting their industry. Their support and encouragement can provide the basis for industry wide improvements. While the construction industry has done an admirable job developing written safety programs and policies, it is necessary for comprehensive/written ergonomic programs and policies that can aid the effective education and guidance to its workers and managers.
Conflict of interest
None to report.