
Abstract
BACKGROUND:
Health care workers are known to be at high risk for occupational musculoskeletal disorders and injuries. Many different intervention strategies have been implemented in order to reduce the risk of injury to health care workers, however not many have been proven to be effective. A continuing care establishment in Ottawa, Canada, implemented a multidimensional kinesiology intervention program for injured employees.
OBJECTIVE:
To evaluate the effectiveness of the kinesiology intervention program on reducing subsequent rates for the nursing personnel and analyze the impact of age, position (RN, RPN, PCA) and sex on subsequent injuries.
METHODS:
The number of recorded work related musculoskeletal disorders (WRMSD) for each patient care worker was counted from 2007–2011. The control group included injured employees that were not referred to the kinesiologists, or who chose not to participate in the program. The intervention group included injured employees that were referred to the kinesiology service and followed their treatment program.
RESULTS:
The intervention group showed a statistically significant reduction of subsequent acute cases when compared to the control group. Nevertheless there was no significant impact regarding age, position or sex on subsequent acute cases.
CONCLUSION:
The kinesiology intervention program within the health care facility was effective at reducing subsequent WRMSD rates within the nursing personnel.
Introduction
Health care workers are at extremely high risk for all types of work related musculoskeletal disorders (WRMSDs) [1]. Between 2011 and 2016 health care workers (Nurse supervisors and registered nurses + Assisting Occupations in Support of Health Services) consistently had the highest number of lost time claims in Ontario, averaging 1170/year, accounting for 12.8% (in 2016) of all claims under the “Bodily reaction and exertion” category (i.e. WRMSD). Sprain and strains were highest among all injuries in this category, making up an average 92% of all these claims over the six years [2]. These groups include all registered nurses (RNs), registered practical nurses (RPNs) and personal care aides (PCAs) [3]. Nursing staff and personal care workers have the highest rate of workers’ compensation claims within the healthcare industry and are consistently among the top ten of non-fatal, work–related injury groups in the USA also [4]. Patient care is highly complex and it includes an assortment of variables that place nurses at high risk for injury. According to the 2016 Occupational Health and Safety: A guide for ONA members published by the Ontario Nursing Association (ONA), in Ontario Canada, the three categories of RN, RPN and PCA filed for a total 11,321 lost work days in 2012 [5] with 4059 total claims that year compared to 3999 claims in 2016 [2]. These proportions indicate that, in Ontario, WRMSD still make up over a quarter of all claims by this group. Many patient care workers believe that musculoskeletal pain is part of their job, not fully understanding the harm being done [6]. WRMSDs can have a significant negative impact on an individual’s capacity to be productive at work while also hindering the person’s quality of life causing discomfort, fatigue and pain [6].
While the prevalence of occupational injuries in the healthcare industry clearly demonstrates a significant problem, prevention efforts have been made. A common approach is to categorize three main modes of prevention concerned with the reduction of WRMSD risk factors [7]. As per accepted public health definitions, primary prevention is when the injury is simply not allowed to occur [8]. Secondary prevention is when the injury is rapidly identified and treated accordingly. Tertiary prevention is when an environmental modification is put in place following a work injury to allow the injured to work and to prevent recurrences [9]. Mechanical patient handling and transfer devices have been a major focus of efforts for prevention [10]. For example, in Ontario between 2004-2005, more than $89 million was invested in extensive ergonomic interventions including new patient lifts, ceiling lifts, electric beds and safety alarms. These ergonomic interventions are commonly accompanied by organizational policies such as “no unsafe lift” policies, which prohibit all forms of unsafe manual lifting of any patient by staff. In Ontario, the Long Term Care Homes Act specifies that “Every licensee of a long-term care home shall ensure that staff use safe transferring and positioning devices or techniques when assisting residents.” [11]. The Centre of Research Expertise for the Prevention of Musculoskeletal Disorders (CRE- MSD) website displays a comprehensive list of such policies from countries around the world. While these types of interventions function at all three levels of prevention, the ideal is that they would prevent any injury from occurring in the first place (primary prevention). Likewise for other common interventions which can be implemented, including education programs and physical conditioning or exercise [12].
A newer approach for occupational WRMSD prevention in the health care industry has been to combine two or more single factor interventions, resulting in a multidisciplinary intervention [13–16]. Many studies have analyzed two and three factor interventions, addressing education and training for body mechanics and use of mechanical equipment, ergonomic interventions or exercise programs [13, 17–23]. All studies have had varying results, although it has been determined that multifactor interventions are far more effective than single factor interventions [12, 24–26]. However, there is still no set standard for what should be included in a highly successful multidisciplinary WRMSD prevention program. Furthermore, there is relatively little research regarding the influence that a multidimensional individualized intervention may yield, wherein a specialized program is developed regarding individual needs, and personalized attention is granted after the occurrence of a WRMSD. This is possible in cases where physical activity or rehabilitation programs can be tailored to an individual’s capacity, job requirements and the ergonomic equipment and policies available in their workplace. This can be further adapted to either injury prevention, recovery or recurrence. The objective of this work was to evaluate the effectiveness of such an individualized intervention.
More specifically, the aim of the study was to evaluate the effectiveness of the kinesiology intervention (both rehabilitation and subsequent preventative exercise) program on reducing WRMSD rates among Registered Practical Nurses (RPN) and Registered Nurses (RN) and Personal Care Assistant (PCA). WRMSD injury cases included work related sprains and strains, whether they be muscular or articular, which resulted in time away from work. We hypothesized that RPNs would have more new or recurring WRMSDs than any other work position and that advanced age would be a factor in subsequent cases. If an an individualized approach to injury prevention in fact reduces the prevalence of either new or recurring WRMSDs in the nursing profession, then perhaps the kinesiology program might serve as a role model for other long term care facilities and hospitals.
Methods
Background
The study was based on secondary data provided by four facilities which provide complex continuing care and care of the elderly including rehabilitation, palliative care, long-term care and family medicine. More than 950 health care workers (RNs, RPNs and PCAs) work for the organization which provides 743 beds. The Occupational Health and Safety Services Office (OHSS) within the institution have a specifically designed program that grants injured employees’ access to individualized care and physical education and training from a team of doctors, nurses, physiotherapists and kinesiologists. The doctors, nurses and physiotherapists are involved with acute care of the injured workers and managing their cases and claims. Once the injury has been assessed and treated if necessary, the employees are then transitioned into the kinesiology intervention program eventually facilitating the return to work.
Study design
All patient handling personnel (RNs, RPNs and PCAs) employed at the Continuing Care centre, who sustained a WRMSD from 2007–2011 were included in the study population.
The control group consisted of WRMSD cases that were not referred to the kinesiologist, or who chose not to participate in the program even though they were referred. The intervention group consisted of injured employees that were referred to the kinesiology service and followed their treatment program. Adherence to the program was solely determined by a positive WSIB discharge report or clinical notes from the kinesiologists stating the employee had met the goals of the program. After being divided into groups, the number of subsequent cases sustained after the initial incidence for each individual was noted. If an individual was referred to and compliant with the kinesiology program during any time from 2007–2011, any WRMSD that occurred prior to the implementation of the program was not counted. The effectiveness of the program was determined by the number of subsequent WRMSD cases suffered in each of the two different groups of employees.
Participants
There were 163 members of the nursing personnel that met the inclusion criteria. Descriptive data of the participants is presented in Table 1 along with individual characteristics for the control and intervention group. The kinesiology program was offered to and completed by 59 participants, and not completed by 104 participants, the mean age was 48.7 for the intervention group and 50.4 for the control group.
Description of the study population and control and intervention groups
Description of the study population and control and intervention groups
Primary interventions
Equipment intervention: In 2005, the Continuing Care centre installed approximately 527 ceiling lifts throughout the hospitals.
No-lift policy: Continuing Care is a no-lift organization. The formally written policy “Lifts, Transfers, and Repositioning” was implemented in 1990 and states: “staff shall not lift patients manually, but must use an electrical /mechanical lift, except in extraordinary circumstances (e.g., cardiac arrest, fire, other life threatening circumstance, or when a mobile or ceiling lift is medically contraindicated)”.
Education: In addition, this policy also states that newly employed staff involved in patient handling must complete hands-on education sessions on Safe Patient Handling during initial orientation. All staff involved in patient handling must also attend pertinent, ongoing education offered within the facilities.
Individualized intervention after primary WRMSD
The program was introduced in 2003, where it primarily focused on work hardening and functional body mechanics training. The program has been under constant development since then, evolving into a complex multidisciplinary program including three main components for patient care workers: education for body mechanics training, job shadowing, and exercise programs to enhance functional capacities. Three qualified Kinesiologists administered the intervention program from 2007–2011. Body mechanics training is done through simulation with the kinesiologist in their office. The focus is safe work postures and correcting improper techniques which may have developed over time and certain at risk behaviors nurses tend to adopt. Job shadows (which were introduced solely in 2009) are performed on the unit, where the kinesiologists will provide advice and recommendations for safe work practices while reinforcing proper body mechanics. The exercise program is developed according to the individual’s needs. After an initial assessment, a training program is developed to address potential instabilities and muscle weaknesses or imbalances. The aim is to ensure the employee has the strength and control required to meet the physical demands of their job. Depending on the specific employee’s needs, a select few or all of the components are implemented.
Data sources
The Continuing Care centre supplied injury and demographic data for all nursing staff from January 2007 to December 2011.
Injury records
All initial data was retrieved from the Parklane data management system. This system contains all the workplace incidents that occur at the Continuing Care centre. The participants’ data was searched and retrieved using the following criteria: WRMSD cases occurring from 2007–2011, WRMSD sustained by patient care workers and injuries that qualify as an WRMSD.
OHSS database and employee files
Using the OHSS database and employee files located in the OHSS office, information regarding the participants was retrieved. These data sources contain information and notes for all employee interactions with the members of the OHSS office (doctors, nurses, physiotherapists and kinesiologists). Referral to the kinesiology program along with the employee adherence to the program was determined using these sources.
Case definition
Cases were defined as work related musculoskeletal injuries that occurred due to a “strain”, “sprain” or repetitive movement. Those occurred due to the lifting or repositioning of patients were also included. All other WRMSD (for example, slips and falls, injury due to patient violence, etc) and non-occupational disorders and injuries were excluded. Narrative information from incident reports (documented through the Parklane database), were used to define the case and determine the inclusion or exclusion. All participants were employed and working at the Continuing Care centre for the duration of the study period (2007–2011) and any employee that suffered from a chronic condition, had a long-term disability claim during the period of study, or didn’t receive any form of treatment from the OHSS staff at the time of their injury were excluded from the study. In addition, employees who had a number of recorded injuries that was more than two standard deviations away from the average population were eliminated from the study. These individuals are classified as “yellow flags” by the OHSS at the Continuing Care centre and therefore are part of a different population. In order to eliminate these potential outliers any individual that was documented in their clinical notes as being a “yellow flag” were automatically excluded.
Statistical analysis
All data was analyzed using SPSS. For confidentiality purposes before uploading data to SPSS, every employee in the study population was given an alphabetical and numerical ID (A# for the intervention group and B# for the control group). The number of subsequent injuries was determined using the data sources. Using one way ANOVA tests, independent variables such as: age, sex and position (RN, RPN, PCA) were analyzed to determine if they had an impact on the dependent variable which was the number of subsequent injuries. The intervention and control group were then compared to determine if the referral to the program significantly lowered the risk of subsequent injuries. To answer what levels of effect each independent variable demonstrated, descriptive analysis was executed containing, means with standard deviations, standard errors and 95% Confidence Interval for Mean.
Results
The hypothesis was confirmed. Referral and adherence to the program does in fact have a significant effect on reducing subsequent WRMSD rates. However, no other independent variable analyzed had an effect on future WRMSDs.
One-way ANOVAs
Descriptive analysis and one-way ANOVA results of subsequent injuries when analyzed with each independent variable indicated no significant findings for either work position F(2,160) = 1,142 p = 0.313, sex F(4,158) = 1,213 p = 0.251 or age group F(1,161) p = 0.307 having had an impact on an individual suffering subsequent cases (Table 2). However, referral and adherence to the kinesiology program was proven to have a significant impact on reducing subsequent cases F(1,162) = 6,555 p = 0.011. Individuals who were referred to the program and completed it were 51% less likely to suffer a subsequent WRMSD than individuals who were not referred or never completed the program.
Descriptive information computed after one-way ANOVA of number of subsequent WRMSD cases with each independent variable
Descriptive information computed after one-way ANOVA of number of subsequent WRMSD cases with each independent variable
*P value statistically significant at χ ≤0.05%.
Overall, the effect of the Kinesiology program was determined using the combination of data from 2007–2011. Figure 1 demonstrates the yearly breakdown of referrals to the program and injury rates. Rates of WRMSDs in the study population peaked in 2008 at 41 injuries and by 2011 dropped to 30. Figure 2 demonstrates the percentage of referral to the kinesiology program, which increased over the years, starting at a low of 28% in 2008 and attaining 47% of individuals being referred and adhering to the program in 2011.
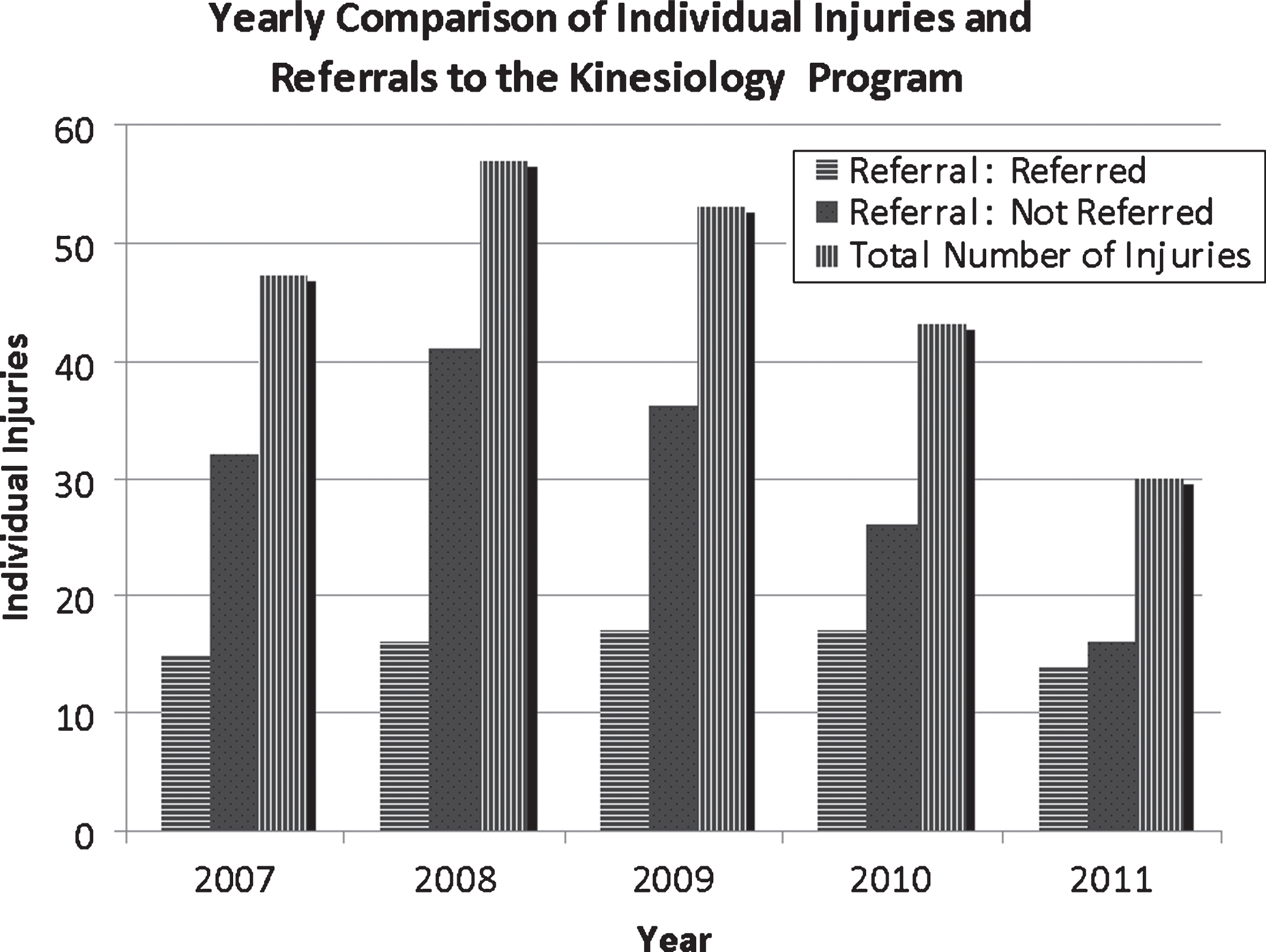
The number of WRMSD for both the experimental (referred) and control (not referred) groups. Those who participated had fewer WRMSD cases.
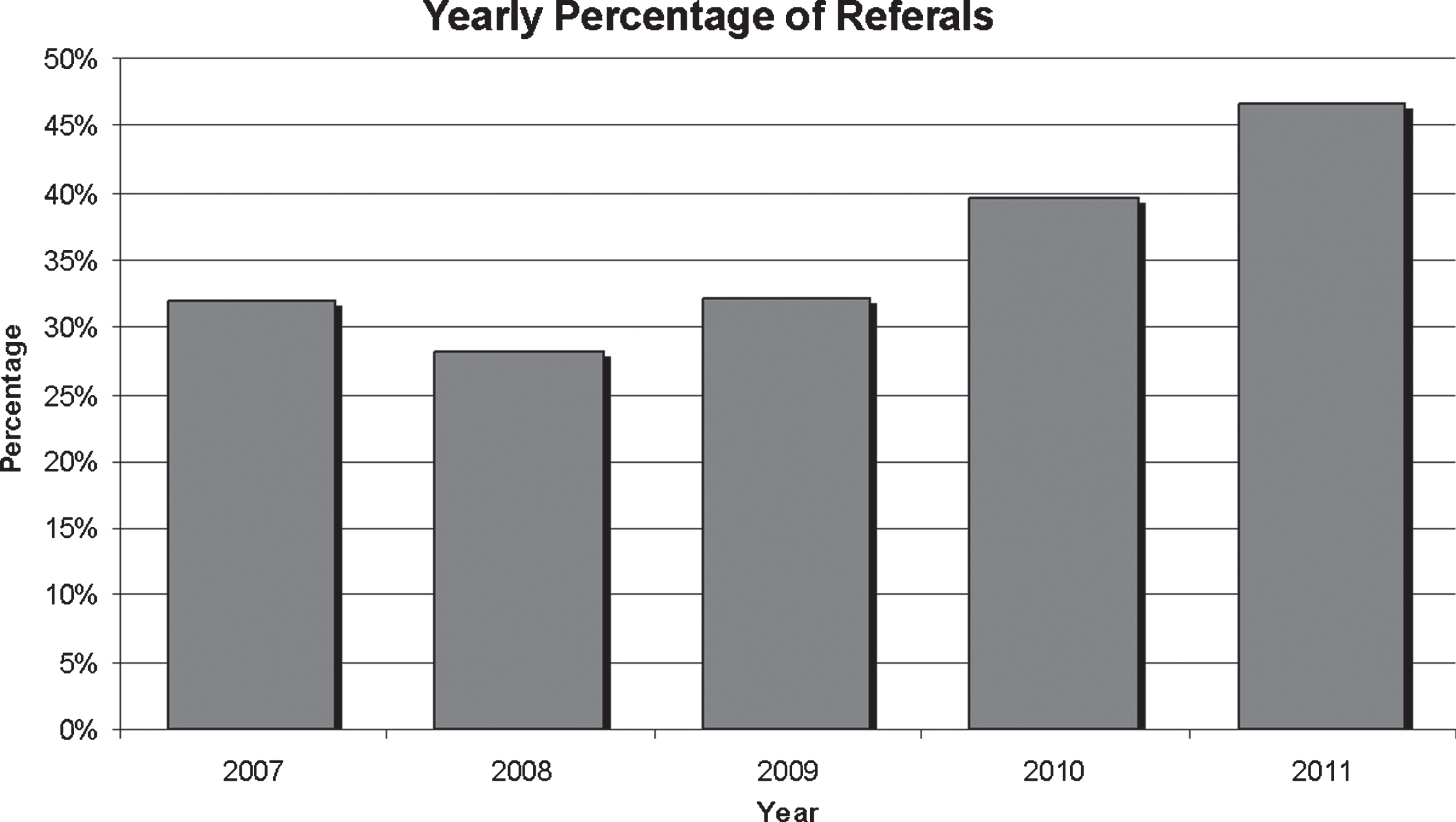
The number of referrals to the conditioning program over the years of the study.
The objective of this study was to determine if the kinesiology program had an effect on preventing WRMSDs in patient care workers that have had a previously WRMSD acute case, which was confirmed. In addition, to determine if age, position: RN, RPN, PCA or sex had an impact on injury rates in order to better direct the program in the future, but none of these had an impact on subsequent risk. Data over 4 years was analyzed which allowed for a large study population and a comprehensive data set. In addition, this allowed analysis of the progress and development of the program over the years, also indicating a positive outcome for the future. By counting the number of WRMSD it focused the attention on the employees at hand and whether or not they prevented future injury by taking part in the comprehensive multidisciplinary program.
Effectiveness of multidisciplinary intervention
While the evidence is still somewhat contradictory particularly in relation to low back pain [27], some studies have addressed the effectiveness of WRMSD prevention programs that could be effective in various environments. For example Shariat [28] found that exercise intervention was helpful for office workers. Likewise, Ojala et al. [29] found that outpatient rehabilitation successfully improved employees’ physical capacity. Van Eerd et al. [16] systematically reviewed the state of knowledge on workplace interventions to prevention of upper extremity musculoskeletal disorders. They found that resistance training can help prevent and manage these disorders. From an ergonomic perspective, Teeple et al. [10] in a meta-analysis found that of safe patient handling and mobilization programs were effective for reducing injuries. Therefore, it is no surprise that combining aspects of all these types of interventions was effect in reducing WRMSD in our study.
Effect of number of subsequent WRMSD cases computed after one-way ANOVA analysis
Effect of number of subsequent WRMSD cases computed after one-way ANOVA analysis
While it is not possible in the current study to identify which aspects of the individualized multifactorial intervention program were most effective, strong evidence was found indicating that an intervention consisting of some individualized combination of education for body mechanics training, job shadowing, and exercise programs combined with primary preventive measures is effective at reducing risk of subsequent injuries. The program at the Continuing Care centre also takes into account individualized needs. Due to this, there is no set number of sessions and set program to follow. Every employee’s specific needs are taken into consideration; therefore if someone requires additional education, training or job shadowing they may receive it.
Failure to detect any effect regarding age, position or sex, is somewhat confusing and may be due to multiple factors. It is possible that the physiological benefits of youth equate to the benefits of multiple years of work experience regarding risks of sustaining WRMSDs. The particular tasks and roles for each position differs significantly in the hospital setting. It has been shown that PCAs are more likely to sustain WRMSDs than RNs or RPNs based on their particular work tasks [6]. However, our findings did not indicate that PCAs were more likely to be subsequently injured than any other position. This could be due to the fact that all types of WRMSDs were taken into consideration and therefore strains and injuries due to repetitive movements were also included (not just injuries sustained while lifting or repositioning patients). Further analysis on specific disorder/injury cause, and location would be needed to determine if each position is more likely to provoke certain forms of WRMSD. The small percentage of male participants could have influenced the lack of effect regarding sex, although the nursing profession is primarily female dominated and therefore would be next to impossible to have an equal population of males and females without using a significantly smaller sample size.
Development of program
The hospital-based intervention was not easily accepted by the employees with 64% of employees either choosing not to follow the program or never being referred over the four year term. Participation could not be enforced and because it might require significant physical effort some workers choose not to participate or they abandon after a short time such that they can not be included in the participant group. Like any new program introduced into an established department, the program was met with significant resistance for several years, with a very limited number of participants being referred from the beginning until 2007–2008. However, as the years progressed a certain amount of confidence and trust in the program developed within the OHSS team and the employee population. Therefore, as the program advanced, a larger percentage of individuals were being referred by the OHSS staff and more individuals were adhering to the program and willing to participate. Moreover, the overall rate of WRMSD injuries reduced by 52.6% from 2008–2011. In addition, as the program developed, certain changes were implemented in hopes to benefit the employees and improve the program. For example, enhanced education regarding body mechanics training, along with newer approaches to assessments were developed throughout the years. This included the introduction of job shadows in 2009. The changes may prove to be significant and impact future studies using data after 2009 only.
Study limitations
The study did have certain limitations. Once discharged from the program employees are encouraged to continue with the measures set in place during the program. However, it is not possible to determine if the employees continue to adhere to the program (i.e continued exercise program, use proper body mechanics, etc.). No questionnaire regarding employee impression of the program or adherence afterwards was implemented during this study. This was primarily due to the fact that the inclusion criteria stated that the study population had to be employed during the time period of 2007–2011, therefore a large percentage of the study population were no longer employed at the Continuing Care centre during the time of this study. Another significant limitation to the study was the lack of documentation. In order to determine if each WRMSD adhered with the case definition established, detailed information was needed from the employees chart notes. Many employees were eliminated from the study due to incomplete documentation and insufficient details regarding their involvement in the program and this may have biased the results, though it is not possible to know in which direction.
Conclusions
This study demonstrates the effectiveness of a multidimensional intervention program involving: education for body mechanics training, job shadows, and exercise programs for injured employees. In addition, the organization has put in place primary preventive measures including mechanical lifting equipment and a written no lift policy and procedures including education sessions to further protect their employees from WRMSD. This successful program may be used as a baseline example for other establishments hoping to lower the rate of WRMSDs in their nursing personnel. Future studies should include specific type of WRMSD and location, in order to determine if the program should be adapted to include specific interventions targeting problem areas for different positions.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We acknowledge the efforts of Dr. Melanie Mehes and Quoc Hao Mach for analytical support as well as Michelle Laurence for writing and formatting help.