
Abstract
BACKGROUND:
Plastic shopping bags are used world over. However, users may suffer pain in or injury to their fingers because of the relatively thin plastic handles of those bags. Due to such drawbacks of the available bag handles, new designs are needed.
OBJECTIVE:
The purpose of this study was to develop a handle that can be used to carry many bags simultaneously. This handle was ergonomically designed and manufactured with soft grip. Then, an experiment was performed to test the usefulness of the developed handle.
METHODS:
The cardiac cost, discomfort ratings, activity levels of eight muscles, and peak plantar pressure (PPP) were the response variables in the experiment. The carrying style (with or without the handle), carrying method (dominant hand or both hands), and weight carried (5%, 10%, or 15% of the subject’s body weight) were the independent variables in the experiment. Twenty-six healthy, young volunteers participated in the experiment.
RESULTS:
It was found that carrying grocery bags in both hands using the bag handle was preferable to the other carrying methods because it reduced the cardiac cost, muscular stress, PPP, and average discomfort ratings.
CONCLUSION:
The results of this study demonstrated that the developed shopping bag handle provides an ergonomic solution for carrying multiple heavy plastic bags.
Introduction
Shopping is one of the ordinary daily activities for a broad range of human beings. Shoppers prefer to carry and transport items such as groceries, clothing, and sundries in flexible plastic bags [1]. The production of single-use plastic bags manufactured per year increased from 120,000 tons in 1960 to 12,700,000 tons in 2006 [2]. This daily activity might be associated with risk factors relevant to carrying weights [3, 4]. Relevant data have shown that overexertion injuries, primarily related to low back pain caused by lifting and carrying loads, resulted in direct costs of $96 million a year [5], and are considered as the leading cause of work related injuries in 2015 (e.g., accounted for 31 percent “356,910 cases” of the total injured cases for all workers) [6].
The carrying style of shopping bags varies from person to person depending on the number of bags carried and their weights. Bags might be carried in one hand [7] or both hands [8]. Possible obvious risk factors associated with carrying shopping bags are compression forces on the lumbar spine and strains and sprains in the fingers, wrists, elbows and shoulders [9, 10]. Besides, the application of excessive passive loads on the wrist tendons in the extreme flexion or extension postures decreases a person’s maximal force production capabilities [11]. The incidence of dominant-side wrist tendinosis reported by Harris et al. [12] was approximately 5.4 per 11 person-years, with the most common form being de Quervain’s disease. This evidence suggests that tools and tasks should be designed to enable the use of wrist postures involving only slight or no wrist extension [13]. Similarly, when multiple bags are carried, the load should be evenly distributed among the bags and between the sides of the body [14].
Many daily activities require the use of one’s hands [15]. Therefore, the hands are valuable organs, and it is important to prevent them from being harmed. Typical plastic shopping bags leave marks on the hands and cause discomfort if they are loaded and held for a period because of the large amounts of stress that are concentrated in their relatively thin handles [16, 17]. By using shopping bag handle, shoppers can easily transport filled plastic grocery bags without enduring pain associated with grasping the handles of the bags with their fingers [18, 19].
Although a variety of handles are available in the local market for carrying plastic bags, all have rectangular or elliptical shapes with small circumference dimensions that cannot fill the hand’s internal circumference. In addition, some of those handles have sharp edges. Therefore, an ergonomically designed bags’ handle that could be used to carry multiple plastic bags would be beneficial. Thus, the objective of this work was to develop a multiple bag handle that could be used to hold shopping bags for a period of time and that would minimize stress and pain in the hands [20].
Product development
The two most important factors that were considered when designing this product were hand comfort and used material type. It is well known that a proper distribution of the contact pressure of an object on the skin minimizes the associated health risks and is therefore directly related to the quality of life [21, 22]. The contact surface shape, material properties, and perceived comfort are the main factors related to the quality of an ergonomic product [23]. In general, ergonomic products are designed based on anthropometric data that are typically represented using maps of body surface data. This type of design process focuses on the similarity between the product surface shape and the portion of the human body that it contacts [24–26].
This study began by determining the design, dimensions, and material of the carrier that would distribute the load over the handle in such a way as to reach the objective. Hooks on which shopping bags could be hung were added at two different locations along the carrier to distribute the load. Finally, a comfortable and safe handgrip was designed. It was optimized for various geometric requirements and aimed to maximize the contact area between the hand and the handle [27]. Das [28] determined the optimal grip length (100 mm), grip diameter (35 mm), grip shape (circular), and handle orientation (perpendicular to the direction of the acting force) for such a device. These criteria were determined based on more fundamental studies of hand geometry and maximum contact pressure [27]. Furthermore, the bag handle was designed to be as small as possible while still enabling shopping bags to be carried comfortably. The initial design was as shown in Fig. 1a. Finally, the optimal material was determined to be hard plastic (high-density polyethylene) because it has a proven ability to support heavy loads without significant or permanent damage to its shape.
The hooks of the bag handle were designed to have an oblique shape to minimize the stress that could develop at the intersection of the handle the part containing the carrying hooks, which increased its strength. After selecting the handle material, shape, and dimensions, the design was modeled using 3D computer-aided design/computer-aided manufacturing (CAD/CAM/CAE “CATIA V5”) software. The resulting 3D models were then integrated into simulations that generate Numerical Control codes to operate CNC machines [29]. The final product was developed by adding hooks so that the load would be distributed evenly across the handle, as shown in Fig. 1b.
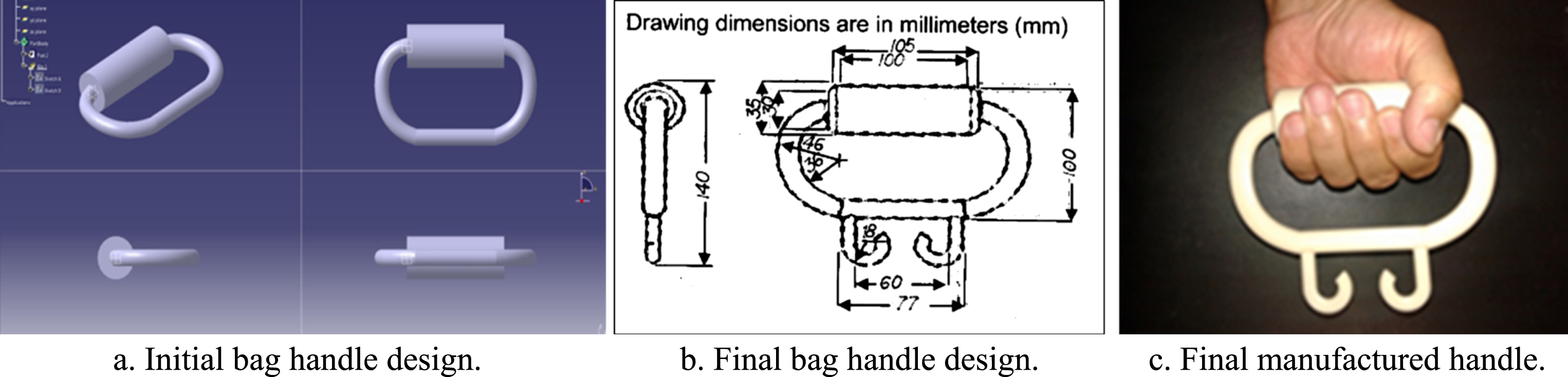
Handle design and manufacturing.
An experiment was performed to investigate the differences between carrying grocery bags using the developed handle for a period and without using the bag handle. A within-subjects experiment was conducted to test the effects of three factors: carrying style (with or without the handle), carrying method (dominant hand or both hands), and weight carried (5%, 10%, or 15% of the participant’s body weight). Each plastic grocery bag was filled with groceries of known weights so that the sum of their weights equaled the intended percentage of the participant’s body weight. The cardiac cost, discomfort rating, activity levels of eight muscles, and Peak Plantar Pressure (PPP) were the response variables. Only a mixed design was employed to analyze the PPP statistically, in which the limb (right foot versus left foot) was a factor in the between-subject design. The cardiac cost and discomfort rating were controlled using walking duration in seconds as a covariate factor.
The collected data were then analyzed using Statistical Package for the Social Sciences (SPSS Version 22; www.spss.com) software. Factors that were identified as significant were further analyzed using the t-test or Tukey’s test to differentiate between their significance levels. In addition, if an interaction effect was determined, a simple effect technique [30] was employed to ascertain the strength of the effect for each carried load. The Shapiro–Wilk [31] test was implemented to verify the normality of the data. The statistical significance was set at the 95% confidence level.
Participants
Twenty-six young, active male college students volunteered to participate in this experiment in which students were encouraged to do their ergonomics course projects throughout experimental work in the lab. This was orally announced during ergonomics classes. The means (±standard deviations) of their ages, weights, and heights were 20±1.7 years, 655.3±93.2 kgs, and 1.733±0.073 meter, respectively. Allof the participants were volunteers and were right-leg dominant, as identified based on their preferred kicking legs [32]. Potential participants were excluded from this experiment if they had experienced spinal pain or neuromuscular disorders in their upper or lower extremities in that year. Each of the participants signed an informed consent form approved by the University Human Subjects Internal Review Board and underwent a thorough clinical examination to ensure the absence of hip and knee pathologies that might affect their gait during the PPP test. The foot examinations consisted of measurements of the passive and active ranges of ankle joint, subtalar joint, and metatarsophalangeal joint motion, as well as pronation/supination.
Response variables
Cardiac cost
Each participant’s heart rate was recorded using Biosig Insta-Pulse Heart rate monitor # BIS-203. The instrument was calibrated based on the manufacturer’s guidelines. The cardiac cost was calculated as the difference between the participant’s mean heart rate during the test and his heart rate immediately after starting to walk after a 3 min period of seated rest and without carrying any bags [33, 34].
Discomfort ratings
The discomfort ratings were based on locally perceived discomforts (LPDs) in the hands, upper arms, and shoulders. A full hand–wrist map with five regions, shown in Fig. 2, regions as well as upper arm and shoulder.was employed. Groenesteijn et al. [35] proposed a discomfort rating system consisting of three 12-cm-long lines corresponding to pain, numbness and pressure, and tiredness in the relevant body part. Participant was asked to rate his discomfort on each of these three measures by marking the corresponding line at the start of each trial and immediately after executing the task. These ratings were quantified on a six-point scale ranging from 0 (no discomfort) to 5 (extreme discomfort). Discomfort ratings are easy to use and require almost no training [36]. The increase in discomfort rating was considered for the statistical analysis.

Hand map for subjective assessments of (1) index finger, (2) middle finger, (3) ring finger, (4) little finger, and (5) palm, and subjective rating scales for (top) pain, (middle) numbness and pressure, and (bottom) tiredness.
Each participant’s maximum discomfort rating was determined as a reference point to facilitate comparison of the different participants’ responses [17]. Each discomfort rating was divided by the same participant’s maximum discomfort rating, using the formula
where i is the participant number (i = 1, 2, …, 26); j is the carrying style number. (j = 1, 2); k is the carrying method type (k = 1, 2); l is the carried load (l = 1, 2, 3); Y ijkl is the normalized value as a percentage of the ith participant’s discomfort rating when using the jth carrier type and kth hand type and carrying the ith load; X ijkl is the raw discomfort rating for participant i when using the jth carrier type and kth hand type and carrying the lth load; and Max i is the ith participant’s maximum discomfort rating.
The participants were subjected to surface electromyography (sEMG) following a standardized procedure to assess muscle activation [37–43]. The sEMG activities of the right hypothenar (RHT), right thenar (RT), right brachioradialis (RB), right flexor digitorum superficialis (FDS), right deltoid medial part (RD), right lower trapezius (RLT), right erector-spinae (RES), and left erector-spinae (LES) were measured while the participants carried loads using one or both hands. The selected muscles are those involved in closing the hands and balancing while carrying loads. All of the participants were right-hand dominant.
The electrical activation of each muscle was measured using a wireless portable 8-channel Biomonitor ME6000 electromyograph (Mega Electronics Ltd., Kuopio, Finland) with a band-pass filter of bandwidth 8–500 Hz and a 14-bit A/D converter at a sampling rate of 1000 Hz. The raw data were recorded and processed by MegaWin 3.1 (Mega Electronics Ltd., Kuopio, Finland) and filtered using a bidirectional fourth-order Butterworth filter with a 20 Hz low-pass cut-off to remove high-frequency noise.
The sEMG procedure began with shaving and cleaning of the skin using alcohol to reduce the skin impedance to less than 20 kΩ. Then, two disposable, circular (10-mm-diameter), pre-filled Ag/AgCl Ambu blue sensor surface electrodes (Ambu A/S, Ballerup, Denmark) were placed 20 mm apart to minimize potential cross-talk from adjacent neutral sites. Those were applied longitudinally to the direction of the muscle fibers, at the midpoint of the palpated muscle belly nearly halfway between the motor endpoint area and the distal part of the muscle. All of the recording electrodes were fixed to the skin using strapping to minimize potential movement artifacts. No participant reported in any way that the strapping interfered with participant movement.
Isometric maximal voluntary contractions (MVCs) were measured before the trials to normalize the sEMG data for each muscle against a maximal reference. The participants’ joints were placed at the appropriate angles, and isometric resistance was introduced by an adjustable chain connected to fixed horizontal climbing bars [44]. The protocols of measuring the flexion MVCs of the right hypothenar and right thenar muscles were similar to those ones used in Griffin et al. [45]. The participants were instructed to push against the chain maximally and hold the maximum position for 3 s. Each MVC was repeated three times with a rest period of 60 s between successive actions. The measurement procedures were standardized regarding body posture, verbal instructions, and encouragement [46, 47]. The principal investigator performed the measurements.
Peak plantar pressure (PPP)
The PPP is the maximum pressure that develops between the foot and the ground while the foot is in contact with the ground, and it indicates the foot and ankle functions while walking. A Tekscan Mat Model Strideway 2 with 0.91 meter wide by 2.60 meter long (Tekscan, Boston, MA, USA) was used to perform static PPP measurements while the participants were standing and dynamic foot pressure measurements while they were walking. The HR Mat sensor is an ultra-thin (0.007”, 0.18 mm) flexible printed circuit that is used for pressure detection and transforms the raw pressure information into related colors. The sensor consists of 8352 individual pressure-sensing locations, referred to as “sensing elements,” which are distributed evenly across its surface and are arranged in rows and columns. Each sensing element can be viewed as an individual square on the computer screen by selecting the 2D display mode. The plantar pressure data were sampled at a rate of 50 Hz and were passed through a PC interface board (Super-Receiver) to the computer for storage and analysis using the system software. The insoles were calibrated using that subject’s weight before the data were collected.
The accuracy of this pressure-sensing system has been well documented by other research groups [47, 48], and consistent reliability has been reported for measurements of high pressures under the heel, metatarsal head, and hallux [49]. Furthermore, when the applied pressure was compared with the calibration pressure, the measurement error was found to be in the range from 1.3% to 5.8% [48].
For each carrying scenario, the data from three out of five self-paced speed-walking trials were used to ensure the stability of each subject’s measurements. The data from any test in which the participant altered his stride were considered unacceptable. The highest pressures recorded under the heel, metatarsal head, and hallux for the right and left feet were used for analysis. The PPP data from each participant’s individual trials were averaged for statistical analysis and were scaled according to the participant’s body weight.
Experimental protocol
An orthopedic physician screened the potential participants. Demographic and anthropometric information for each participant, including his weight with his shoes off, was gathered and recorded before the experiment was performed. Then, the schedule was established. Each participant underwent 12 experimental sessions in 4 days and was asked to wear fitting light clothes such as T-shirts and shorts during the execution the experiment.
The bag-carrying sessions began on the second day. The order in which the experimental conditions were applied was randomized to minimize the participants’ learning effects. All of the experimental sessions were performed in a controlled laboratory environment with a dry bulb temperature of 20°C–22°C, 50% –55% relative humidity, 360–400 Lux of light (as measured on a desk), and 60–65 dBA of noise. The participants were asked not to take part in any physical activities before participating in the experiment to eliminate fatigue due to external factors.
The MVCs of the participant’s muscles were measured at the beginning of each testing day. Before placing the surface EMG electrodes, the experimenter prepared the skin by shaving excess hair and cleaning the area by rubbing alcohol. Then, the EMG electrodes were placed on the participant’s RHT, RT, RB, FDS, RD, RLT, RES, and LES and were secured with double-sided adhesive tape. After the electrodes had been prepared, MVC trials were performed to collect reference measurements that were used to determine the muscle contraction strength percentages [50]. Then, MVCs were conducted for the selected muscles, with 1-min rests between measurements. The MVCs were performed according to the standard methods used for muscle testing. For EMG data processing, the root-mean-squares (RMSs) were calculated. In addition, the RMSs were normalized to the maximum RMSs of the tested muscles in the reference activities.
After the MVC tests had been completed, the participant was asked to sit in a chair at the starting point of the walkway for 3 min to recover from any muscle fatigue. The participant’s resting heart rate and discomfort rating were measured while he was standing, before he began to walk. Then, the participant was asked to carry the assigned load as close to the body as close as possible, using the selected carrying method. The participant was asked to walk five times around the perimeter of the ergonomics laboratory, and the stopwatch was used to measure the elapsed time [51, 52]. Starting from the third round of walking, the participant’s PPP and heart rates, as well as the sEMGs of the selected muscles, were measured for 5 s in the last three rounds. When the participant had completed the carrying task using the assigned method, he was asked to rate the discomfort in his hands, upper arms, and shoulders using the rating scales mentioned earlier. The means of the heart rates, PPPs, and sEMGs of the muscles measured during the last three rounds of walking were calculated and recorded for later analysis. Finally, the participant was offered a 15-min break before performing the next carrying task, which allowed the experimenter to prepare and set up the subsequent carrying condition.
Results
Cardiac cost
The carrying style by the carried weight had a significant effect on cardiac cost, F(2,48) = 3.26 and p < 0.047. As shown in Fig. 3, when the weight of the carried grocery bags was 15% of the participant’s body weight, the cardiac cost was significantly lower when the bags were carried using the handle than when they were carried without using the handle, with t(51) = –7.848 and p < 0.0001.
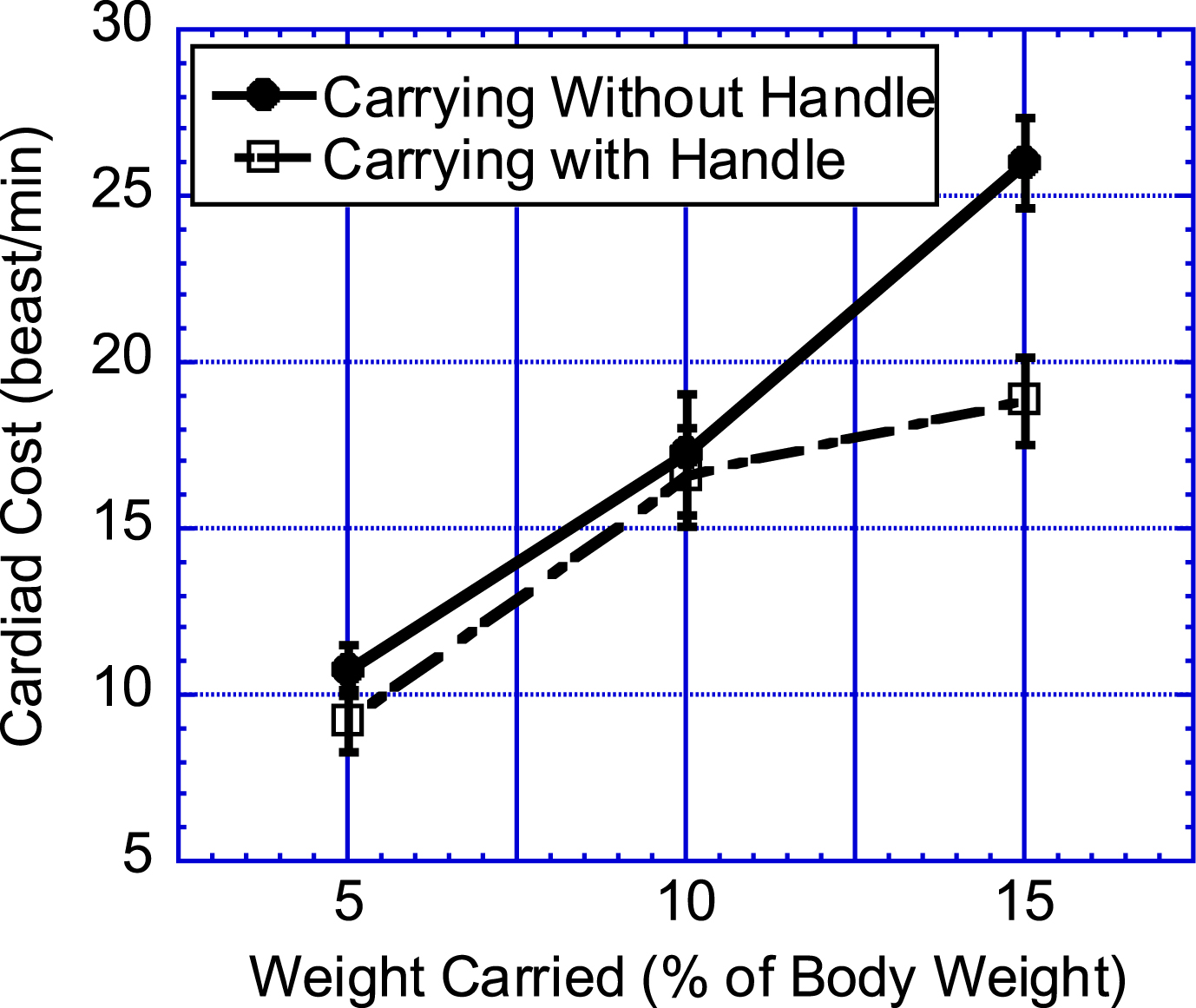
Effect of carrying style by carried weight interaction on participant’s cardiac cost.
The results showed that all of the main independent variables significantly affected the participants’ discomfort ratings, as shown in Table 1 and Fig. 4. Bag carrying style had a significant effect on perceived discomfort ratings in the index, middle, ring, little, palm, and shoulder. Carrying method and weight carried had significant effects on perceived discomfort ratings in the index, middle, ring, little, palm, upper arm, and shoulder.
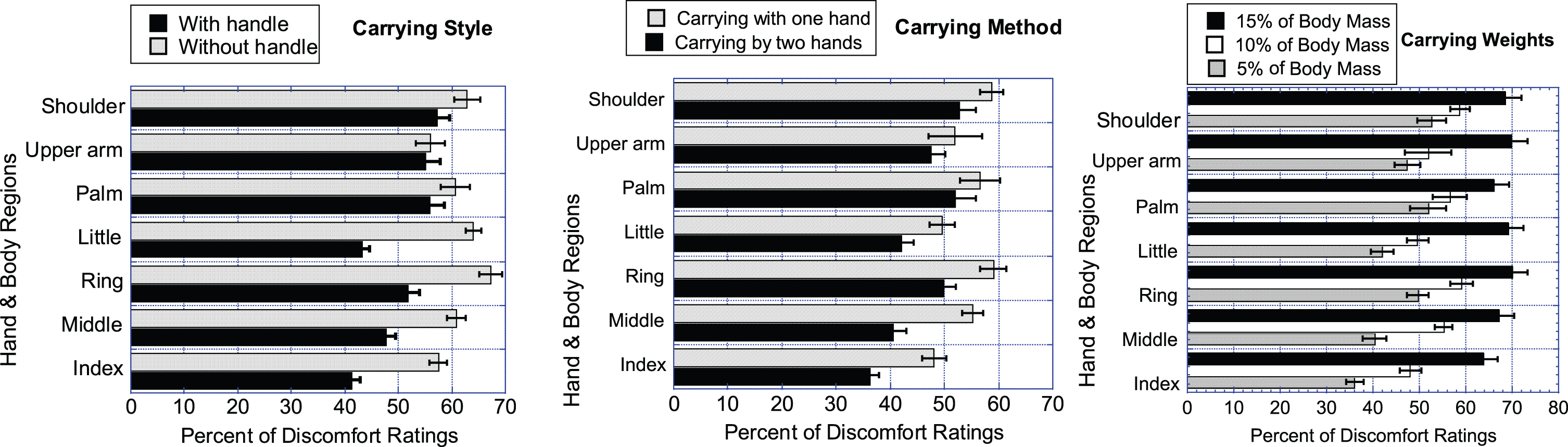
Effects of carrying style by carrying method by carried weight interaction on participants’ discomfort ratings.
F-and p-values for the upper extremity parts. Their discomfort rating was significantly affected by the main effects of the three independent variables
The carrying style significantly affected the participants’ muscular activities (RHT, RT, FDS, RD, and RLT), which were substantially lower when they carried the grocery bags using the handle than when not using it (Table 2). The carrying method significantly affected all measured muscular activities, which were substantially lower when they carried the grocery bags using both hands than when using only their dominant hands. In addition, the carried weight significantly affected all measured muscular activities, which were substantially higher when they carried greater weights in their grocery bags. Furthermore, the carrying method by the carried weight interaction significantly affected the participants’ sEMG results in the RHT, RT, RB, FDS, and RLT. The carried weight significantly affected the participants’ muscular activities of RD, RES, and LES in absence of the interaction between the carrying method and the carried weight (Fig. 5).

Effects of carried weight on participants’ RD, RES, and LES MVCs. % MVCs of Right Deltoid Medial Part, Right Erector-Spinae, and Left Erector-Spinae.
F-and p-values for the muscles. %MVC was significantly affected by the main effects of the three independent variables and the interaction between the carrying method and the shopping bags’ weight
As shown in Fig. 6 and Table 3, when the carried weight was 10% of the participant’s body weight, the muscular activities were significantly lower when both hands, instead of just one hand, were used to carry the grocery bags. Similarly, when the carried weight was 15% of the participant’s body weight, the muscular activities were again significantly lower when both hands, instead of just one hand, were used to carry the grocery bags.

Effects of carrying method by carried weight interaction on participants’ RHT, RT, RB, FDS, and RLT MVCs.
t-and p-values for the muscles. % MVC was significantly affected by the interaction between the carrying method and the shopping bags’ weight
*n.s. means not significant difference.
The PPP was found to be significantly higher for the right foot (256.3 (13.9) kPa) than for the left foot (235.75 (13.6) kPa), with p < 0.041. The effect of the carrying method was also significant, with F(1,50) = 5.25 and p < 0.026. The PPP was substantially higher when only one hand was used to carry the load (250.2 (9.9) kPa) than it was when both hands were used (241.8 (11.0) kPa).
The carried weight also significantly affected the participants’ PPPs, which were higher when they carried greater weights in their grocery bags, with F(2,100) = 16.08 and p < 0.0001. The PPP increased significantly from 234.43 (11.4) kPa to 245.75 (9.9) kPa when the carried weight increased from 5% to 10% of the participant’s body weight, with p < 0.003. In addition, the PPP increased significantly from 245.75 (9.9) kPa to 257.88 (11.5) kPa when the carried weight increased from 10% to 15% of the participant’s body weight, with p < 0.012. Finally, the PPP increased significantly when the carried weight increased from 5% to 15% of the participant’s body weight, with p < 0.0001.
Discussion and conclusions
In this study, the responses of healthy young male participants carrying grocery bags with weights of approximately 5, 10, and 15% of their body weights while walking at self-paced speeds were examined. These loads were chosen to create levels of exercise varying from easy to somewhat difficult for this young population [10].
Carrying grocery bags using one’s hands is an almost global task that is performed by anyone who shops for groceries. Shoppers may accomplish this task by using one of the two main methods: holding the grocery bags close to one side of the body or holding the bags close to both sides of the body. Carrying plastic bags in front of the participant’s body is not preferred by the shoppers when compared to carry groceries using paper bags. As expected, distributing the load between both hands decreased the participants’ cardiac costs, discomfort ratings, muscular activities, and PPPs [53]. The results of this study agree with those reported by Irion et al. [10] and Fredericks et al. [54]. In addition, this study showed that the cardiac cost could be lowered by carrying grocery bags using the developed handle when compared to carry the load without the handle.
An important physiological feature was observed when the carried load was placed directly above the body’s center of gravity [55]. The results of the present study, as well as those of others, Kamon and Belding [56] and Michael et al. [57], revealed that the cardiac cost and the activities of the RES, LES, and RLT are the lowest when the load is evenly distributed and positioned close to the body.
The PPP was reduced significantly by holding the grocery bags with both hands rather than with just one hand because this arrangement spread the load between the two feet. This finding agrees with those of previous studies [51, 58], where increasing the carried weight also significantly increases the PPPs in the feet.
Carrying loads using the designed grocery bag handle was found to decrease both the discomfort ratings and muscle activities compared to those when the loads were carried without the handle. The logical explanation for the reduction in muscle activity while using the handle is that the handle increased the contact area between the hand and the handle. The correlations between carried weight, pain discomfort and perceived exertion have been investigated in several studies. Ling et al. [59] reported that increasing the load also increases the level of discomfort. Similarly, Beekley et al. [60] found that participants’ levels of discomfort were significantly higher when they carried loads that comprised higher percentages of their body weights. Lloyd et al. [61] reported that pain and perceived exertion in all body regions increased when the carried load was increased from 10% to 70% of the participants’ body weights. Goslin and Rorke [62] further showed that there is a linear relationship between perceived strain and the weight of a carried load. Quesada et al. [63] reported that no load and a load with a weight equal to 15% of a participant’s body weight produced similar results regarding perceived exertion but participants perceived higher strain while carrying 30% of their body weights. The increase in the participants’ subjective ratings of perceived exertion when performing asymmetric carrying instead of symmetric carrying that was observed in this study has been demonstrated previously [64–66].
In conclusion, a shopping bags’ handle with an oblique profile and a high-quality non-slip grip was designed in this study to provide a more comfortable grip. Unlike the currently available handgrip which is made of hard rubber, the newly designed improved handle is made of durable and high-quality rubber that prevents it from causing blisters on the palms. In addition, existing handles are straight, causing wrist strain due to the bent wrist posture required to use them, as well as reducing shoppers’ comfort and increasing their fatigue when carrying grocery bags for long distances. Both ends of the newly designed handle are bent to ensure that the wrists remain straight while carrying bags. The improved handle was found to increase comfort while carrying bags. With this new tool, a person can lift and carry 15% of his body weight comfortably. Thus, this study revealed that it is advantageous to carry grocery bags close to the body with both hands using the developed handle.
Future research might build on the findings of this study and extend to investigate other populations, especially the young females and the elderly (both males and females) as these two populations are heavily involved in the task of shopping and carrying shopping bags, possibly for longer periods.
Despite the authors’ repeated attempts to recruit females by distributing flyers and pamphlets in the girls’ section, only male participants were recruited for the study. Another restriction on the finding pertains to the participants’ pool recruited for this laboratory study. The participants were recruited from the college student population, and none of the participants had significant prior manual lifting experience. However, the results presented herein may apply to an experienced population for similar carrying transfer tasks.
Also, participants’ walking speed was self-paced to simulate the practical condition when exposed to different load stresses. All these factors could have an impact on the level of carrying capability during a carrying task. On the other hand, those variables should not affect the main findings of this study, such as the importance of using such kinds of proposed devices for handling shopping bags. This study, therefore, includes carrying methods and a tool so that the individual can choose the most appropriate one for himself and the specific context.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors are grateful to the Raytheon Chair for Systems Engineering for funding.