
Abstract
BACKGROUND:
During the 2009 H1N1 influenza epidemic, roughly half of survey respondents reported having worn a hygiene mask. However, most were unsatisfied with commercially available masks.
OBJECTIVE:
The long-term goal was to develop a comfortable, high-performance hygiene mask. This study investigated holistic attitudes of mask wearers and identified the most prominent problems as a basis for developing a new mask.
METHODS:
In 2009, 2012, and 2015, identical surveys were conducted among Japanese university students. The rate of mask use, intended uses, and problems reported while wearing a mask were aggregated. Co-occurrence analysis of individual respondents’ data was conducted.
RESULTS:
For men, the most intended uses were influenza prevention in 2009 and common cold prevention in 2012 and 2015; common problems were humidity in the mask, glasses misting over, and breathing difficulty. For women, the most intended use was common cold prevention in all 3 years; common problems were humidity, glasses misting over, breathing difficulty, and makeup coming off.
CONCLUSIONS:
Men’s attitudes in 2009 were different from those in 2012 and 2015. However, women’s major attitudes were consistent in all 3 years. For both sexes, the most commonly reported problem was humidity in all 3 years. It is expected that more comfortable masks for daily use will result from improving humidity characteristics.
Introduction
Our long-term goal is to develop a comfortable, high-performance hygiene mask [1]. Hygiene masks are a type of personal protection equipment [2, 3]. Masks are classified by their purpose: for industrial uses [4], for medical uses [5], and for self-care uses in daily life. Wearing industrial-type masks is an occupational hygiene measure to protect the wearer from harmful substances in environments such as factories, farms, and construction sites [6]. There are national standards in Japan for industrial masks, such as dust-protective masks [7] and gas masks [8]. Medical masks are worn by health-care workers in medical institutions [9]. In Japan and some other countries, hygiene masks in daily life are commonly worn at the discretion of the individual user. The present paper focuses on hygiene mask use in daily life.
There are no national standards in Japan for self-care hygiene mask use in daily life. They are developed however a manufacturer sees fit. A hygiene mask consists of a fabric sheet that covers the wearer’s nose and mouth; two strings loop over the ears to secure it over the wearer’s face. After 2009, greater variety developed in mask design, with respect to shapes and size, materials used, and ply structures [10, 11]. There was also increased variety in the ear strings regarding length, shape, and materials [12]. In our survey in 2009 [13], 87.3% of men and 94.9% of women in Japan reported experiencing problems while wearing a mask.
In 2009, an influenza A (H1N1) epidemic occurred on a worldwide scale [14, 15]. In Japan, use of a hygiene mask in daily life was recommended through the mass media by the Ministry of Health, Labour and Welfare, and the Infectious Disease Surveillance Center in Japan. The use of hygiene masks increased accordingly, leading to shortages in some Japanese markets [16]. Our previous survey was conducted in the social setting of the end of that unusual year. It is possible that the results of the survey for that year may not apply to the current situation because of the influence of respondents’ increased sensitivity regarding influenza outbreaks.
This paper reports the number of mask wearers, intended uses, and problem awareness while wearing a mask in 2012 and 2015; this paper also presents the results of our previous survey [13]. Subsequently, holistic attitudes of mask wearers were computed by co-occurrence analysis. With a focus on holistic attitudes, the most prominent problems are identified toward developing a more comfortable hygiene mask.
Method
Survey method
Surveys were conducted three times using identical questionnaires. The first survey was conducted from October 2009 to February 2010, the second from November 2012 to February 2013, and the third from October 2015 to January 2016. In 2009, the respondents were university students in the Tohoku, Kanto, Chubu, Kinki, and Kyushu regions of Japan. In 2012 and 2015, the Chugoku region was included in addition to the regions surveyed in 2009. The pencil-and-paper questionnaire was distributed to the respondents and returned upon completion.
Questionnaire context
The questionnaire content was identical in all three surveys. Demographic data for age, sex, and the respondent’s prefecture of residence were queried at the beginning of the questionnaire. Subsequently, experience wearing a hygiene mask (Q1), intended uses (Q2), and whether the respondent was aware of any problem while wearing a mask (Q3) and specific problems (Q4) were queried. In Q1, the experience of wearing a mask without intended uses of hay fever countermeasure was queried with respect to seasonal diseases [17]. Each multiple-choice item in Q4 was determined based on the result of a pretest. The questionnaire items were as follows: Q1. Do you wear a hygiene mask without hay fever? (Yes or No). (If yes is selected, continue to question 2.) Q2. For what purpose do you wear a hygiene mask? (Free description). Q3. Do you have some troubles or concerns with wearing a hygiene mask? (Yes or No). (If yes is selected, continue to question 4.) Q4. What are you troubled or concerned about? Multiple choice: (P01) Humidity (P02) Mist over glasses (P03) Breathing difficulties (P04) Awkwardness (P05) Makeup coming off (P06) Ear pain (P07) Feeling hot (P08) Feeling distraction (P09) Poor fit in size (P10) Other (Free description)
Analysis method
The analysis process used for the data is shown in Fig. 1. The number of mask wearers, the number of respondents for each intended use, and the number of respondents for each reported problem were aggregated for men and women by year. For aggregated data, the differences between men’s and women’s data, and differences among the data within each year, were tested statistically by chi-square test. P < 0.05 was considered statistically significant.
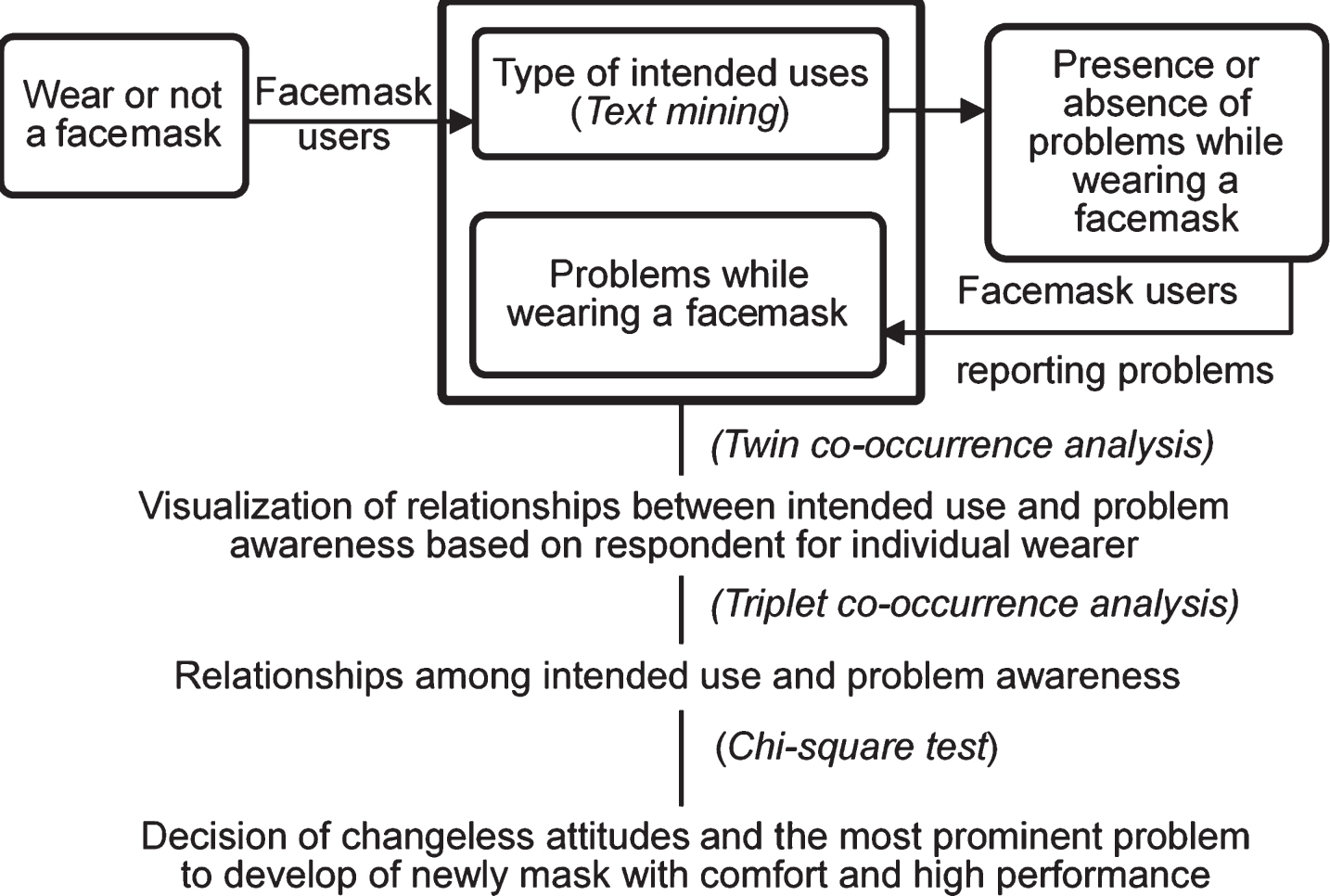
Analysis process of the data.
Based on the responses for individual respondents, relationships between an intention for use and reported problems were visualized by twin co-occurrence analysis. Subsequently, holistic attitudes composed of intended use and reported problems were analyzed by triplet co-occurrence analysis. Finally, holistic attitudes in each year were tested statistically by chi-square test. Attitudes among wearers that did not change were identified. Problems that needed to be addressed were prioritized in developing the new mask.
Aggregated respondents
The numbers of aggregated respondents were 1519 (consisting of 715 men and 804 women with a mean age of 20.4 years [standard deviation; SD = 2.6] and 19.9 years [SD = 2.6], respectively) in 2009; 2892 (1403 men and 1489 women, aged 20.2 years [SD = 1.5], and 19.4 years [SD = 1.1], respectively) in 2012; and 3197 (1147 men and 2050 women, 19.8 years [SD = 1.5] and 19.6 years [SD = 1.3], respectively) in 2015.
Rates of mask use
The rates of mask use (Q1) were 44.1% in men and 53.4% in women in 2009, 46.9% in men and 72.9% in women in 2012, and 48.2% in men and 75.4% in women in 2015. In each year, the percentage of women who wore masks was significantly higher than that of men (P < 0.001 for each). There were no significant differences in the percentage of male wearers among the 3 years (minimum P = 0.080). In contrast, the rate of female wearers in 2012 and 2015 increased compared with 2009 (2012, 2015: P < 0.001 for each). These results showing constant rates of use among men and increasing rates among women in 2012 and 2015 were likely caused by men being consistent with respect to health care and becoming accustomed to wearing a mask; by contrast, the health-care consciousness of women increased.
Intended uses
Responses with regard to intended use (Q2) in the form of free written descriptions were labeled according to the word meaning by text mining approach. The labeled data were then aggregated. The codes and labels are listed in Table 1. The term “prevention” was used to signify avoidance of infection by the common cold, influenza, and so on. The term of “countermeasure” signified controlling symptoms after such infections had occurred. Subsequently, the rates of mask wearers with each intended use were aggregated according to Table 1. Figure 2 shows the rate of respondents per intended use by year.
Code and label of intended use of wearing a mask
Code and label of intended use of wearing a mask
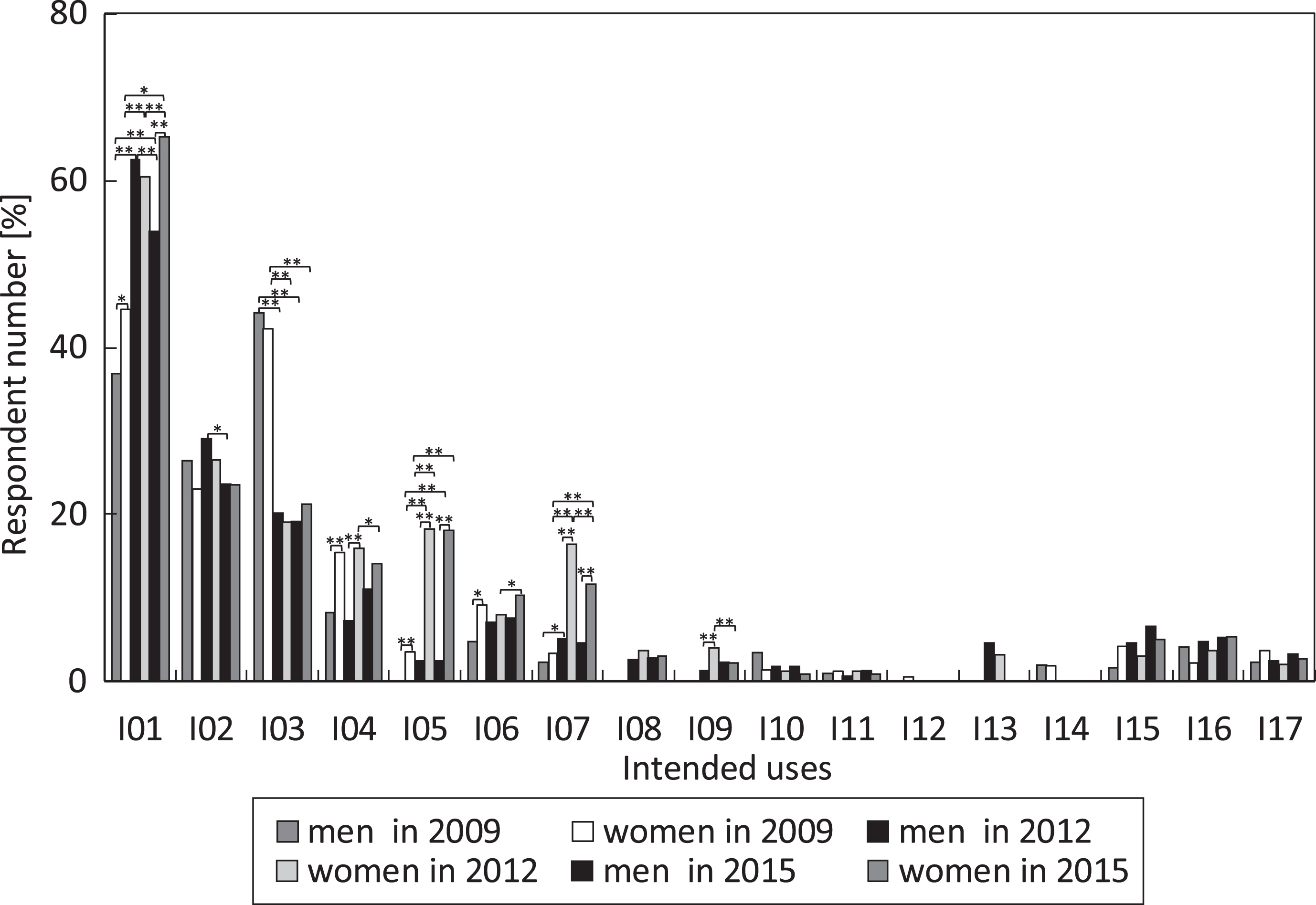
Intended uses for mask wearer in the 3 years. (men in 2009; n = 315, women in 2009; n = 429, men in 2012; n = 658, women in 2012; n = 1086, men in 2015; n = 553, women in 2015; n = 1546).
In each year, the most commonly reported intended uses among respondents were common cold prevention (I01), etiquette (I02) (it is considered impolite to display cold symptoms in public in Japan) [18], and influenza prevention (I03).
Comparing male and female respondents, more female than male respondents cited I01 in 2009 (P = 0.035) and 2015 (P < 0.001), and more female respondents cited masks as a “common cold countermeasure” (I04) in 2009 (P = 0.004) and 2012 (P < 0.001), “hide of my face” (I05) in all 3 years (P < 0.001 for each), “drying prevention” (I06) in 2009 (P = 0.025), “coldness countermeasure” (I07) in 2012 and 2015 (P < 0.001 for each), and “cough countermeasure” (I09) in 2012 (P = 0.001).
In a comparison of the 3 years, the rates of male and female respondents citing I01 and I05 in 2012 and 2015 were greater than in 2009 (I01, men, women: P < 0.001 for each; I05, men in 2012: P = 0.005; men in 2015: P = 0.006; women in 2012 and 2015: P < 0.001 for each). In addition, the rates of female respondents who reported I07 in 2012 and 2015 were higher than that in 2009 (P < 0.001 for each). By contrast, for I03, the rates in 2012 and 2015 were conspicuously smaller than that in 2009 (men, women: P < 0.001 for each).
These results show that there was a difference between the intended uses reported by men and women. Moreover, the intended uses were different between 2009 and the later years. After the influenza outbreak in 2009, the respondents’ concern with influenza prevention seemed to have decreased. However, the median number of intended uses remained at 1 for men and 2 for women in all 3 years. Thus, it was evident that mask use for influenza prevention (I03) shifted to the other intended uses of I01 and I05 for both men and women and I07 for women.
The rates of wearers who reported problems and concerns were aggregated in each year (Q3). The rates were 87.3% (n = 315) and 94.9% (n = 429) in 2009, 85.0% (n = 658) and 90.8% (n = 1086) in 2012, and 82.1% (n = 553) and 89.3 (n = 1546) in 2015 for men and women, respectively. Overall, higher percentages for reported problems were observed in each year. The rate of women reporting problems was higher than that in men in all 3 years (P < 0.001 for each). With respect to years, the rates of both men and women showed a decreasing trend. Statistically, there were significant differences between 2009 and 2015 (men: P = 0.044; women: P < 0.001). It seemed that the decreasing trend was influenced by an increase in the variety of masks available in the Japanese market and Japanese consumers’ increasing adoption of masks.
The number of respondents who reported problems while wearing a mask (Q4) was aggregated. Figure 3 shows the rates of respondents who reported problems in the 3 years. The problem reported most often was “humidity” in the mask (P01), regardless of year or sex. Comparing men and women, there were a significantly higher number of female respondents reporting “humidity” (P01) (2009: P = 0.004; 2012, 2015: P < 0.001 for each). There were also a significantly higher number of women than men who reported “makeup coming off” (P05) (2009, 2012, 2015: P < 0.001 for each) and “poor fit in size” (P09) (2009, 2012, 2015: P < 0.001 for each). Additionally, significantly more female than male respondents reported “ear pain” (P06) in 2012 and 2015 (P < 0.001 for each) and “awkwardness” (P04) in 2009 (P = 0.005) and 2012 (P = 0.045). By contrast, there were higher rates of men who reported “feeling distracted” (P08) in 2012 (P = 0.005) and 2015 (P < 0.001). These results show that there were differences between the problems reported by men and women.

Problems reported while wearing a mask in the 3 years: men in 2009 (n = 315); women in 2009 (n = 429); men in 2012 (n = 658); women in 2012 (n = 1086); men in 2015 (n = 553); and women in 2015 (n = 1546).
Comparing among the 3 years, the proportion of male respondents who reported P03, P04, and P08 in 2012 and 2015 were smaller than those in 2009 (P < 0.001 for each). In 2012 and 2015, the number of female respondents who reported P03 (2012, 2015: P < 0.001 for each), P04 (2012, 2015: P < 0.001 for each), P05 (2012: P = 0.012; 2015: P = 0.043), and P08 (2012, 2015: P < 0.001 for each) was smaller than that in 2009. Meanwhile “ear pain” (P06) was reported at higher rates in 2012 and 2015 than in 2009 (P < 0.001 each).
These results showed that the esthetic concerns of “awkwardness” (P04) and “makeup coming off” (P05), and the issues affecting higher-level thinking of “breathing difficulty” (P03) and “distraction” (P08) in 2009 became lower over time. As mentioned above, it seemed that the decreasing trend in the number of reported problems reflected the increased market availability of a wider variety of masks in terms of different colors, shapes, and sizes, as well as their increasing adoption by the public.
A hygiene mask is a health-care product for individual users. As a first step to understanding the holistic attitudes of individual wearers, the relationships between intended use and reported problems were analyzed by twin co-occurrence analysis [19]. Using an equation (1), the Jaccard coefficient, J was calculated [20].
The number of respondents who had responses of X1 or X2, were entered as the denominator, and the number of respondents who had responses of X1 and X2, entered as the numerator. The co-occurrence networks were visualized by KH Coder software [21]. Figure 4 shows co-occurrence networks with J > 0.2. The nodes with more responses are illustrated with larger circles. Stronger co-occurrences are illustrated with thicker lines.
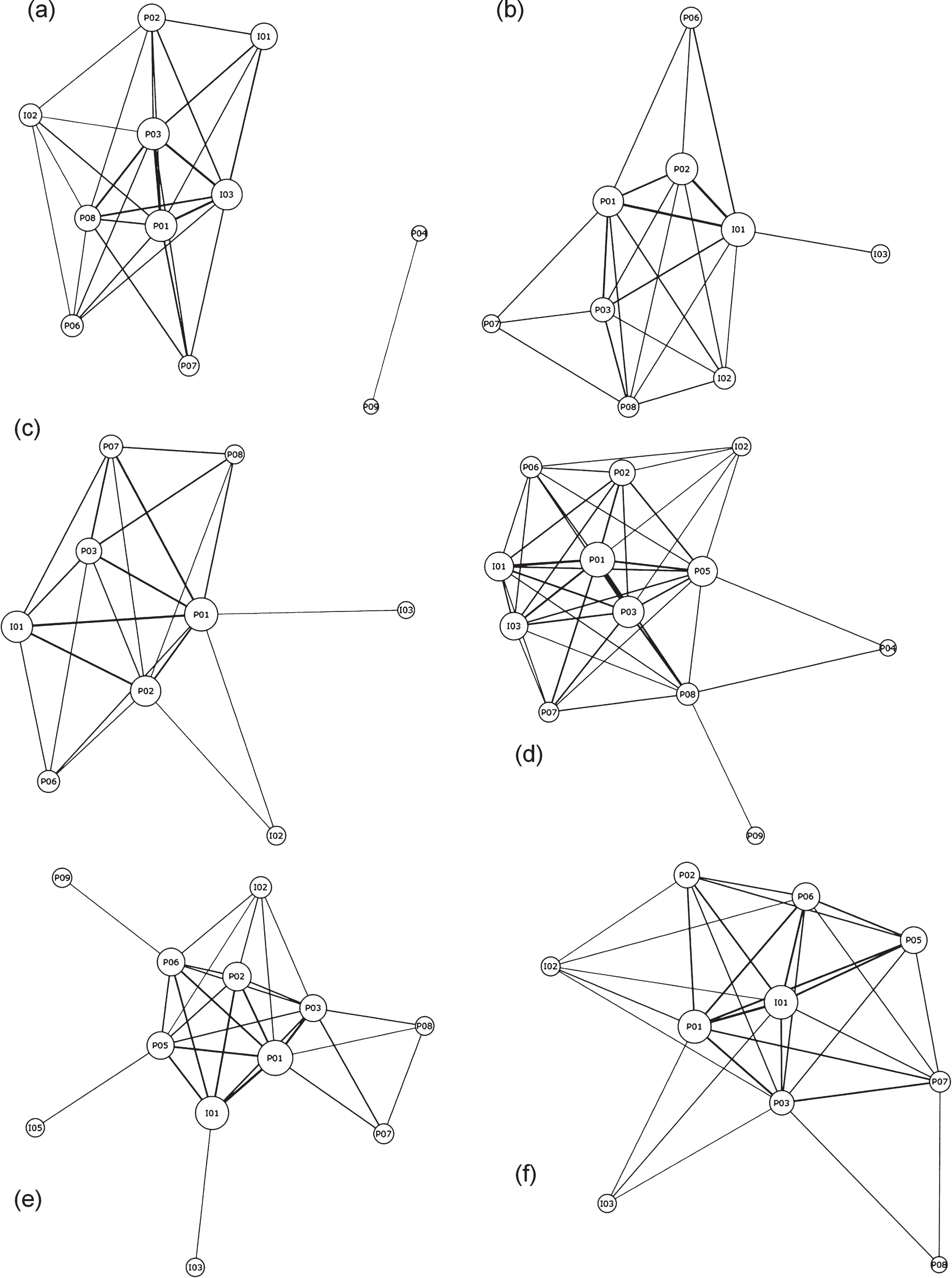
Co-occurrence networks with Jaccard coefficient, more than 0.2. ((a) men in 2009; n = 249, (b) women in 2009; n = 381, (c) men in 2012; n = 553, (d) women in 2012; n = 976, (e) men in 2015; n = 442, (f) women in 2015; n = 1350).
Focusing on relationships with a higher Jaccard coefficient (J > 0.3), at male networks (a) in 2009, the J of I01-P03 was 0.319. The J of I03-P03, P01, P08, and P02 were 0.407, 0.397, 0.349, and 0.304, respectively. At female networks (b), J of I01-P01, P03, P02, and P05 were 0.455, 0.352, 0.314, and 0.311, respectively. The J of I03-P01, P03, P05, and P02 were 0.383, 0.340, 0.304, and 0.301, respectively. At male networks (c) in 2012, J of I01-P02, P01, and P03 were 0.433, 0.430, and 0.303, respectively. At female networks (d), J of I01-P01, P02, P05, P06, and P03 were 0.467, 0.375, 0.363, 0.353, and 0.330, respectively. At male networks (e) in 2015, J of I01-P01, P02, and P03 were 0.423, 0.389, and 0.311, respectively. At female networks (f), J of I01-P01, P05, P06, P02, and P03 were 0.485, 0.405, 0.395, 0.359, and 0.329, respectively.
These results showed that stronger relationships between intended use of a mask and reported problems in 2009 were not the same as those in the later years. In 2009, there were stronger relationships between the intended use of a mask for common cold prevention (I01) or influenza prevention (I03) and reported problems in men and women. In the later years, only the intended use for common cold prevention (I01) had a stronger relationship with reported problems.
Holistic attitudes for individual wearers
As a next step, holistic attitudes were studied by triplet co-occurrence analysis of one intended use (X1) and two reported problems (X2, X3). Table 2 shows co-occurrence among intended use and reported problems with a high Jaccard coefficient (J > 0.15) by triplet co-occurrence analysis.
High Jaccard coefficient among by triplet co-occurrence analysis
High Jaccard coefficient among by triplet co-occurrence analysis
I: Intended uses, P: Problem awareness.
For men, there were no common attitudes among the 3 years. Attitudes in 2009 were different those in 2012 and 2015. In 2009, triplet co-occurrences of I03-P01-P03, P06, P07, or P08, and I03-P03-P07 or P08 had high Jaccard coefficients. In 2012 and 2015 only, high Jaccard coefficients were shown for I01-P01-P02 and I01-P01-P03. There were no significant differences according to the chi-square test. Meanwhile, women had co-occurrences of I01-P01-P02, P03, or P05 in three surveys. Additionally, high Jaccard coefficients for I01-P01-P06 and I01-P02-P05 were shown only in 2012 and 2015.
These results show that holistic male attitudes in 2009 were influenced by the social situation surrounding the influenza pandemic. Meanwhile, attitudes among women overall did not change in the 3 years. Overall, based on the holistic attitudes of men in 2012 and 2015 and those of women in all 3 years, when the problem of “humidity” (P01) is improved, it is expected that other problems for men and women who intend to use masks for common cold prevention will improve as well.
The mask sheet and ear string need to be improved from the viewpoint of hygroscopic, thermal, and air flow properties. These properties are considered to depend on the climate between the wearer’s facial surface and inner surface of the mask sheet. This climate is influenced by material characteristics, fit between the wearer’s facial surface and the sheet, and individual usage characteristics such as facial expression and mouth movement.
In the present paper, mask wearers’ attitudes toward hygiene mask design with respect to better comfort and performance were investigated by repeated surveys in 2009, 2012, and 2015. The surveys comprised queries of whether respondents wore a mask in their daily lives, their intended use, and problems encountered while wearing a mask.
Even after the influenza epidemic ended, the rate of mask use in 2012 and 2015 did not decrease compared with 2009. Moreover, the rate of mask use increased significantly among women in the three surveys. The main intended uses in 2009 were influenza prevention for men and common cold prevention for women. In 2012 and 2015, the main intended uses were common cold prevention for both men and women. It was shown that the highest rate of problems reported by wearers while wearing a mask in both men and women were related to humidity in the mask for all 3 years.
Co-occurrence analysis based on responses for individual mask wearers showed that attitudes among men in 2009 were different from those in 2012 and 2015. In the later years, among men, the main intended use was common cold prevention, and the most reported problems were humidity, glasses misting over, or breathing difficulty. Meanwhile, attitudes among women were consistent in all 3 years. Among women, the main intended use was common cold prevention and the most commonly reported problems were humidity, glasses misting over, breathing difficulty, or makeup coming off.
When hygiene masks are improved to address the problem of humidity from the viewpoint of hygroscopic, thermal, and air flow properties, related physical problems for those who use masks for common cold prevention will also be resolved. Moreover, improvement of not only the mask sheet but also the ear strings is needed for masks to be sufficiently comfortable for mask wearers.
As a foremost consideration, surveys were conducted to acquire less biased data, considering the large number of respondents and dispersion of questionnaire areas in Japan. When the survey results of different occupational groups and different age groups in each area will be added to these results, it is expected that the subjects will provide an accurate representation of the entire Japanese population. Furthermore, in the near future, a survey will be conducted for non-Japanese respondents having different head shapes and sizes. Considering the various head characteristics and consciousness of people of different races while wearing a hygiene mask, global hygiene masks with individual adaptations will be designed.
Conflict of interest
The authors have no conflict of interest to report.
Footnotes
Acknowledgments
The authors are especially grateful to university teaching staff for their cooperation in conducting the questionnaire survey.