
Abstract
BACKGROUND:
Integrating more prevention interventions into different workplace settings as a component of the role of occupational therapists has a significant relevance recognized by the occupational therapy professional community. Even if some studies suggested that occupational therapists already provide prevention interventions, and that other studies showed the efficacy of such interventions, the literature does not offer a comprehensive understanding of the specific practice of occupational therapists engaging in prevention in workplace settings.
OBJECTIVE:
The aim of the study was to describe the practice of occupational therapists toward the development of preventive behaviour at work among their clients.
METHOD:
Semi-structured interviews were conducted with 13 occupational therapists. Phenomenological analysis was used to examine the content of the interviews.
RESULTS:
Results suggest that occupational therapists form representations of preventive behavior that are consistent with theory, but those are limited and do not take into account the complexity of the concept. Results of the interviews found eight different interventions provided by occupational therapists toward the development of their clients’ preventive behavior at work.
CONCLUSION:
Occupational therapists recognize their role in supporting their clients’ development of preventive behavior at work. However, they appear to lack a conceptual understanding and resources to help them in their practice toward prevention.
Introduction
With more than 317 million occupational injuries occurring each year all over the world [1], work-related injuries or illnesses are a major public health concern. Many stakeholders such as governmental and trade union organizations, industries, as well as occupational health professionals, put forth efforts to improve injury prevention at work and the safety of workers. Various modalities can contribute to effective prevention of occupational injuries, such as work procedures, equipment engineering, workers’ training, or management strategies [2]. Those modalities imply a contribution from different stakeholders of a work organization, such as managers and workers. Preventive behavior plays a large role in the prevention of occupational injuries [3, 4].
Occupational therapists are centrally involved in interventions focusing on the rehabilitation of injured workers [5–8]. The literature offers a description of occupational therapy interventions that enable workers to return to work after an injury (e.g., assessment of work capacity, work analysis, environment adaptation, improvement of work behavior, and skills) [7, 9–11]. However, the literature offers little information about the practice of occupational therapists specifically oriented toward the improvement of prevention behavior of their worker clients. A study conducted with Australian occupational therapists revealed their primary prevention interventions were directed toward biomechanics education, manual handling, ergonomics, and prevention of burnout [7]. Results of a US survey also suggested that occupational therapists provide preventive interventions, such as education or ergonomics redesign, to workers [11]. Other authors, based on the results of a meta-analysis conducted on 346 articles, suggested that most often prevention interventions provided by occupational therapists were education to workers and employers, stress management, and ergonomics [10]. Research also suggested the efficacy of occupational therapy interventions in the prevention of work-related injuries or illnesses in various domains, such as ergonomics [12], mental health [13], and education for prevention [14]. Despite these few signs that occupational therapists provide prevention interventions for work-related injuries or illnesses and that these interventions seem effective, the literature does not provide an inventory or describe them in detail. In addition, the impact of the prevention interventions on services offered to clients is also absent from the literature. And, when compared with other services, such as rehabilitation, restoration, or compensation, one study reported that occupational therapists have limited involvement in prevention [15], despite that they believe prevention is the service that demands an increase in attention [7].
The role of occupational therapists in health at work has changed in nature and scope over the last years. The professional community now recognizes the importance of integrating more injury prevention interventions into the daily practice of occupational therapists [16]. In addition, the few scientific articles available to understand how occupational therapists contribute to injury prevention at work are 10 or more years old. Therefore, the first step to implement a greater involvement of occupational therapists in injury prevention is to understand their actual practice. This article presents the results of a study describing the involvement of occupational therapists in the development of injury prevention behavior of workers.
Theoretical background
As mentioned previously, engaging in preventive behaviors at work is a major determinant in the prevention of occupational injuries and illnesses [3]. Preventive behavior consists of observable and measurable actions that a worker can do to protect his 1 own health and safety and those of his colleagues [4]. In this sense, it is a significant behavior to develop among injured workers to ensure a safe return to work and to reduce the risk of future injuries. In addition, a recent concept analysis found that preventive behavior at work is a relevant intervention target for occupational therapists [4]. In fact, results of that study suggest that the primary characteristics defining preventive behavior at work relate to either the worker, the work activity, the environment, or a combination of these components [4]. This is consistent with the occupational therapy assumptions that stipulate that human doing, or occupational performance, is the result of the interaction of various factors coming from three basic constructs, which are the person, the occupation, and the environment [17, 18]. Authors of the concept analysis suggested that occupational therapists have the expertise to help develop each of the five attributes of preventive behavior at work with their clients, which are as follows: 1) compliance with safety rules and procedures; 2) proactivity, participation, involvement, and initiatives related to prevention; 3) maintenance of physical environment; 4) concern for social environment; and 5) reflexivity and analysis of work situations [4]. Figure 1 shows the attributes of the concept. It also presents the antecedents that have to be developed before the expression of preventive behavior, as well as the consequences that can occur after the onset of preventive behavior.
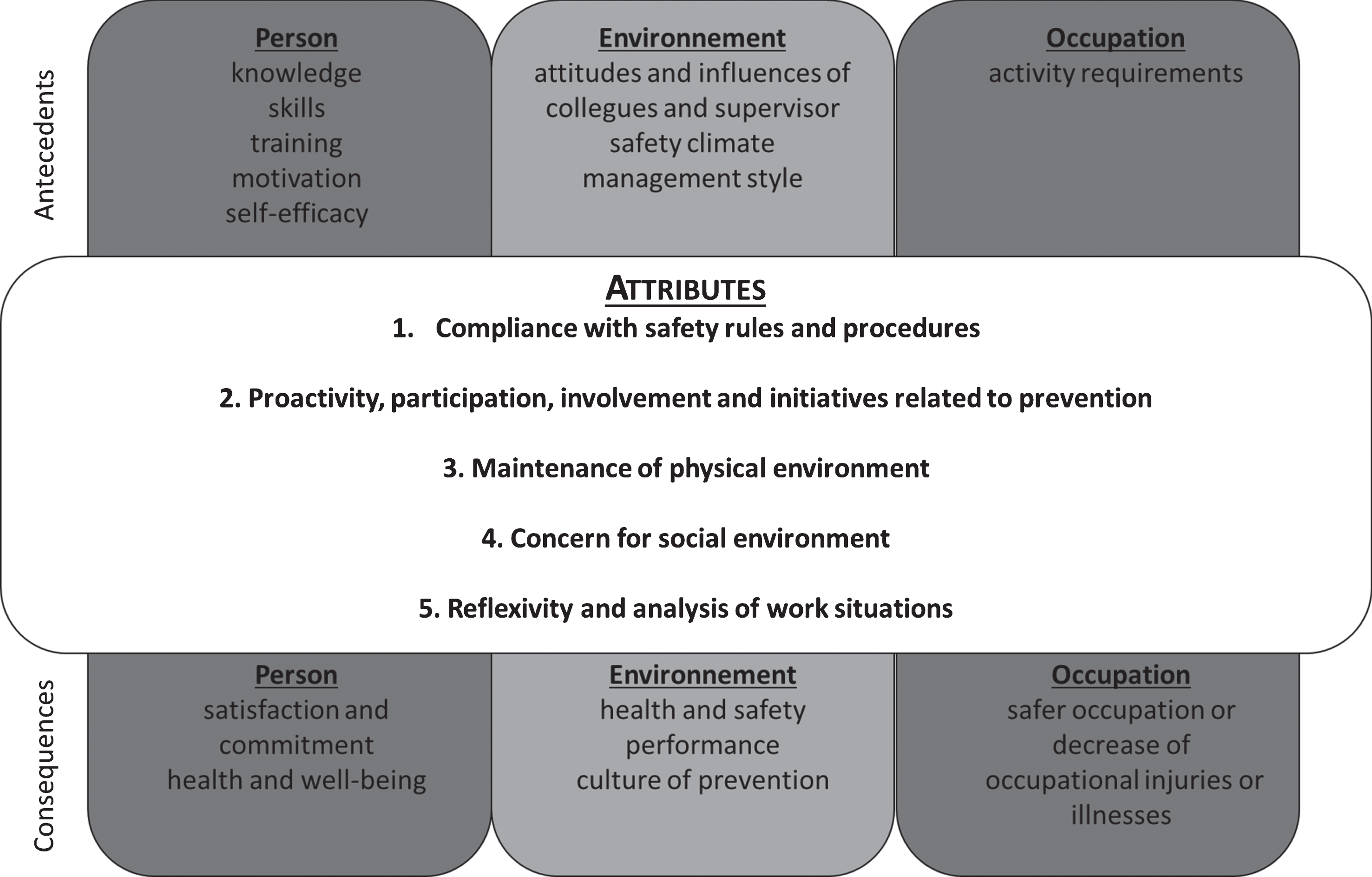
Characteristics of preventive behavior at work – figure adapted from Lecours & Therriault [4].
Preventive behavior at work is a complex concept that is formed from multiple attributes that interact together. Therefore, each of the attributes have to be developed among workers to ensure a safe return to work.
As occupational therapy interventions in the general field of health prevention often focus on behavior changes among individuals [19], to develop workers’ preventive behavior is a significant and relevant prevention practice to apply in the specific field of health at work.
Thereby, to improve occupational therapists’ preventive interventions in health and safety in the workplace and to better align theory and practice, it is important to first describe their current practice in this field.
The aim of the study was to describe the practice of occupational therapists toward the development of preventive at work behavior among their clients.
Method
Research design
A phenomenological qualitative design was followed to achieve the research objective [20–22]. A phenomenological design allows the experience that is studied to be described, in this case the professional practice provided by occupational therapists to clients for the development of preventive behavior at work, from the view of the population involved, namely occupational therapists. This design uses the meaning that people give to their experiences to interpret and understand a lived experience. This design is useful for subjects studied little [20], as is the case in this study. Further, phenomenological design allows the structure of a phenomenon to be described; thus, it can be understood in a more detailed, holistic, and comprehensive manner [23].
Participants
Participants had to meet the following criteria: 1) to be an occupational therapist with at least 1 year of experience; 2) to speak and to understand French, and; 3) to engage in workers’ development of preventive behavior. Participants were recruited through a purposive sampling strategy [24] and selected using a maximum variation sampling strategy [25]. Thus, participants were selected on criteria such as practice area (e.g. rehabilitation center, private practice, or outpatient clinic), gender, age, experience, and education level. Participant diversification of is desirable in the phenomenological design to collect different responses and enrich the description of the phenomenon [21, 26]. No participant who was contacted declined to take part.
Data collection
Individual, semi-structured interviews with open questions were conducted with the participants by a trained research assistant. The aim was to collect information on their daily professional practice that applied to workers’ development of preventive behavior on the job. The interview questionnaire was validated with a pre-test method. Its content and clarity were verified with two occupational therapists and a researcher on health and safety in the workplace, and modified and tested with another occupational therapist before being used to gather information for this project. The preset order of questions was not methodic and could vary depending on the participant to allow for individual ways of structuring thoughts. The meetings lasted 60 to 90 minutes and were conducted in French. Interviews were recorded with digital audio. After the eleventh interview, responses started to become repetitive, and little new information was found, suggesting a saturation of content [27]. Because of the specificity of the subject, this was not unexpected. In fact, Guest, Bunce, and Johnson (2006) suggested that for qualitative studies aiming at understanding perceptions and experiences of individuals sharing a similar reality, 12 interviews is generally enough to reach saturation [28]. Therefore, after all participants who were initially contacted (n = 13) to take part in the study completed the interviews, recruitment ended.
Analysis
Data were analyzed through a phenomenological analysis as described by Giorgi [22, 29]. The primary goal of phenomenological analysis is to derive meaning units from the raw data to capture the experience of participants, namely occupational therapists, related to a phenomenon, namely their role in the development of preventive behavior at work. After all interviews were transcribed verbatim, the data were analyzed through the five-step process of the phenomenological analysis proposed by Giorgi [22]. First, a reading of the entire set of data was done to get a sense of the whole. Second, multiple other readings were conducted to identify meaning units and to assign them codes. Open coding was favored because of the inductive approach used. Units were passages of discourse based on their meaning and relevance to the objective of exploring the occupational therapists’ role in the development of preventive behavior at work of their clients. The QSR NVivo 10 software was used to support the analysis. The third step was to transform meaning units into expressions that were revealing of the experience of participants. The fourth step synthesized a general structure of the comprehension of the phenomenon based on participants’ experiences. Finally, the fifth step was used to refine the structure to clarify and interpret data related to participants’ experience of the phenomenon. Several rounds between applying the raw interview data into the general structure allowed us to fine-tune the analysis process. To improve the validity of the analyses, a second researcher verified the meaning units identified, the codes assigned, and the structure produced. Inter-rater agreement was verified periodically throughout the analysis. After four rounds of coding, an inter-rater agreement was found that was more than 90% of the meaning units identified and codes assigned.
Results
Analyses of interview produced three types of results. First, the descriptive characteristics of participants were compiled. Second, representations 2 of preventive behaviour at work that participants displayed emerged from the data. Finally, interventions toward the development of workers’ preventive behavior that occupational therapists integrate into their daily practice were identified.
Descriptive characteristics of participants
Thirteen occupational therapists completed the interview, 11 women (84.6 %) and 2 men (15.4 %). The mean age of participants was 32.5±8.0 years, and their average amount of experience with workplace health and safety was 6.8±7.1 years. Participants had an education level that varied from bachelor’s degree in occupational therapy to a doctorate in progress. Finally, the sample included participants from diverse practice areas in which where occupational therapy interventions with workers’ health and safety occur. Table 1 lists the main characteristics of participants.
Descriptive characteristics of participants
Descriptive characteristics of participants
*F = female, M = male.
The analysis process showed that, for all participants, the understanding of preventive behavior at work is oriented toward the ways in which the worker adopts a behavior that prevents the onset of injuries. Despite this shared view of preventive behavior at work, analyses described three different representations that are present among the participants, which are as follows: 1) preventive behavior refers to a reflective process; 2) preventive behavior refers to the application of knowledge; and 3) preventive behavior refers to a prescription.
For some participants, preventive behavior refers to a reflective process as they define it by the reflection and by the analysis of a work situation. To illustrate this first representation of preventive behavior at work, a participant explained that “it [preventive behavior] is a behavior that allows the worker to anticipate what problems could arise in his work by analyzing the situation.” 3
In the same vein, another participant argued that, for the client to adopt a behavior that reduces the risks to health or safety in his work, he must first understand his work situation. The following excerpt illustrates this representation:
It seems to me, as I understand it, that preventive behavior at work is when the person analyzes a work situation, understands it, recognizes the risks that may be related to it, and decides to adhere to a behavior that can reduce these risks.
Participants also stressed the importance of not performing tasks automatically, but of thinking, questioning, and adopting the most suitable behavior and thus reducing risks. One participant expressed this idea:
Preventive behavior is when the worker is going to be able to see where and when there is a risk in his job […] and he does not just do a task because he saw someone doing it or because someone told him, ‘You do it that like that!’ He is able to ask himself the question, ‘What position would be best according to what I’ve learned about techniques of lifting, postural hygiene, conservation of energy […]?’
Still respecting the idea that preventive behavior refers to a reflective process, participants raised the important idea that preventive behavior implies that the worker is mindful of himself in his work situation to make the right decision to perform his tasks without putting himself in danger. For example, a participant explained that ‘[preventive behavior] is when he [the worker] becomes aware of how he stands, how he positions himself, and when he has a good ability to analyze himself to correct himself.’
Analyses of the interview data revealed a second representation of preventive behavior at work. In fact, for several participants, preventive behavior refers to the application of knowledge. They explained that, for them, preventive behavior is the ability of the worker to obtain and to learn methods or techniques and afterward to apply apprenticeship in his work situation. In fact, a participant explained that preventive behavior is present if workers ‘inquire and apply what they have learned.’ Another participant expressed this representation as follows: ‘To have a preventive behavior is to be able to generalize what has been learned, to become aware of it, and then to be able to reproduce it during work.’
The last representation reported by participants concerns preventive behavior at work being a prescription. For some participants, preventive behavior is defined as a requirement to be respected by the worker, as explained by a participant who said that preventive behavior at work refers to a worker who ‘meets employer’s standards or labor’s standards.’
Other participants talked about preventive behavior as being a prescription developed by all stakeholders around work, involving workers, organizations, and even society. This verbatim quote illustrates this idea:
For me, it [preventive behavior] would be all the actions or decisions that one takes, namely the person who is the worker, but it can also be the organization. I think that even at the level of the society there are things that happen to avoid an eventual incident at work that could affect the physical or psychological integrity of a worker or a group of workers. So it’s really what we put in place to avoid situations where people could be put at risk.
This broader view of the origin of the prescription implies that the worker is involved in the definition of what has to be respected toward prevention.
Interventions toward the development of preventive behavior at work
Analyses finally allowed to identify several interventions related to prevention that are provided in the daily practice of occupational therapists. Eight categories of interventions have emerged from the analyses. Figure 2 provides these categories as well as the description of prevention interventions that emerged from data analysis.

Description of interventions related to prevention provided by occupational therapists.
Risk assessment is an intervention that was reported by all participants. In fact, occupational therapists mentioned that they evaluate several aspects that may cause risks for the worker’s health and safety. Among others, they evaluate a client’s work techniques, work requirements, physical environment, and workstation as well as labor relations in the workplace. Participants found it important to get a whole and precise portrait of the possible risks for their client, in order to plan suitable interventions thereafter, as expressed by this participant who explained he had to ‘analyze the client’s disabilities versus the demands of the job before deciding what interventions to put in place.’
Second, education is an intervention that was reported to be included in almost all clients’ therapy, according to participant reports. The education provided is oriented toward various subjects, such as postural hygiene, joint protection, and compensatory strategies, as expressed by a participant: ‘I will teach compensatory strategies, postural hygiene, and postural correction that can be applied to work.’ Pain and energy management are also interventions often provided by occupational therapists toward injury prevention. In fact, a participant explained that ‘it is important to teach energy conservation principles so the client does not run out when he returns to work, which could lead to an injury.’
Awareness and encouragement is another intervention that emerged from the data. In fact, it appears that occupational therapists encourage their clients to report occupational health and safety risks they note in their work. They also encourage clients to report to colleagues or supervisors the work methods or preventive initiatives that they find effective. A participant expressed the idea as follows: ‘I try to get clients to be proactive in their environment, in their work team, and to suggest to others the safe work methods that we have tried together, because everyone should benefit from it in the end.’ This category of interventions also concerns the awareness-raising of the client toward maintenance of the physical environment to reduce risks to health and safety, as reported in this excerpt of transcript: During workplace visits, I will ask him [ the client ], for example: ‘Is the work environment like this all the time? Is there always dust on the rails? Have you thought about cleaning? It’s going to be easier to push [your trolley] if it is clean.’
Rehabilitation, such as the development of work capacity or practice of new/compensatory work strategies, is seen as a means to reduce occupational risks that was reported by most participants, as illustrated in the following excerpt:
I want to develop new ways of doing things that improve how well a job task is done […] I tell the client: ‘Bring me a problematic situation about your work and we will find a method of doing it well.’ […] So, basically, we practise together to change the manner of doing the work tasks, to avoid injuries.
The fifth subcategory of strategies provided by participants to reduce risk to health and safety faced by their clients is Adaptation. More precisely, participants talked about the ‘adaptation of workstations, of work physical environment.’ This intervention was reported by some participants as an action of the occupational therapist and by other participants as an activity to teach to the client, so he can do a proper adaptation of his workstation.
Collaboration was also an important strategy discussed by participants, and many of them reported using it in their daily practice with workers. They primarily referred to collaboration as the way to work in partnership with the employer and other collaborators to put in place conditions that promote the prevention of risks to health and safety when a client returns to work. A participant expressed this idea with a situation of mental health problems:
What happens most often is when a worker returns to work after a stoppage due to a mental health problem, the employer, the worker, the occupational therapist, and the insurance agent are trying to find solutions to put good conditions in place, we ask: ‘What conditions will we put in so the person does not relapse?’
An often reported strategy was Control. In fact, participants talked about the importance of the control of several factors in their practice with workers. Among others, they explained that they ensure the client wears his personal protective equipment during task training and during workplace visits, as expressed by a participant: ‘When we make our visit in the workplace, we have to check if the client wears his helmet, his safety glasses, his boots, his bib. Precisely, we have to ensure he is able to follow the rules.’ Other participants also reported that they must ensure the client follows work procedures prescribed by his work. Finally, some participants expressed the idea that they often correct client’s work positions if he adopts postures that put his health and safety at risk.
The last strategy evoked by almost all participant is Enablement. Participants discussed the presence of enablement in their daily practice with workers in several manners. Among others, they reported enabling clients to ask for help and to communicate with others in order to not put themselves at risk for work-related injuries or illnesses. Diverse modalities are used to develop communication abilities of the worker, such as role plays, as illustrated in this excerpt of transcript: ‘I have already done role plays with a patient. He has to practise saying his opinion to an employer.’ Another form of enablement reported by participants as being part of their practice is to help clients become able to analyze work situations to identify risks to health or safety. A participant explained the way he approached this issue with a client in this excerpt:
I tell him [the client], ‘Evaluate the risks associated with the task you are doing to make sure you can do it. If you cannot do it well, different methods can be found.’ So, through the analysis of the work situation, I am enabling him to do analyses while we are doing our therapies.
Another participant expressed this idea of enabling clients to analyze work situations:
Well, I enable them [the clients] to perform activity analysis. I want to ensure they can understand the potential risks [of the work activity] and they can also understand the potential risks associated with their capacities. I tell them, ‘You have the capacities, so evaluate the risks associated with the task you’re doing to make sure you’re able to do it.’
A last type of enablement strategies evoked by participants was about training the client to be able to mobilize resources and to solve problems. The following excerpt of transcript illustrates this idea:
I’m trying to make the worker able to find his own solutions because at some point we will not be there all the time. After the identification of the problem, let’s find out what could be the solutions, and choose the best among those that are possible. After that, test and evaluate if the solution you chose was the best.
Representations of preventive behavior at work
Study participants form representations of preventive behavior at work that are consistent with theory. However, their understanding of preventive behavior at work is reductive and does not consider the complexity of the characteristics that define the concept. In fact, the first representation suggests that preventive behavior at work refers to a reflective process, which actually suits the attribute #5, which is the reflexivity and analysis of work situations. The second representation participants form about preventive behavior concerns the application of knowledge. Interestingly, this representation may be related to antecedents of the concept in the sphere of the person that concern apprenticeship, namely knowledge, skills, and training. This representation also agrees with the several interventions related to education of the clients reported by participants. Finally, a last representation emerged from the data and concerns preventive behavior at work as being a prescription. Discrepancies exist between the participants’ perceptions of this representation. Indeed, for some participants, preventive behavior is the individual responsibility of the worker to comply with the prescription set by the employer or a legal organization. For other participants, preventive behavior at work still refers to a prescription, but one which must be established by all the stakeholders of an individual workplace, suggesting that workers have a responsibility in defining the rules and actions to be taken. This divergence of perceptions is interesting and may reveal a lack of knowledge about the legislation. In fact, in the Canadian province of Quebec, the Act respecting occupational health and safety recommends a shared responsibility of prevention between the worker and the employer [30], suggesting the worker has a role to play in the establishment of prevention strategies. Also, antecedents and consequences of preventive behavior at work concern not only the worker himself, but also the social environment and work organization. It then appears that the whole work environment and everyone in it has to be involved in the onset of a worker’s preventive behavior.
In summary, representations that occupational therapists form of preventive behavior at work are consistent with its theoretical definition, but they lack precision and do not reflect all its characteristics. A lack of theoretical understanding of the complexity of preventive behavior at work appears to be part of occupational therapists’ practice. Training and resources must be provided to them, so they can be aware of the five attributes and of antecedents that must be developed among their clients, to promote an involvement toward prevention of injury when workers return to employment.
Interventions toward the development of preventive behavior at work
Even if representations of preventive behavior at work are incomplete and do not reflect the entirety of the concept, occupational therapists provide several interventions in their daily practice to develop their clients’ preventive behavior at work. A closer look at these interventions allows to understand that occupational therapists provide interventions that contribute directly to the development of their client’s preventive behavior at work. In fact, most interventions reported by occupational therapists are linked to the development of attributes or antecedents of preventive behavior at work. Figure 3 illustrates the relation between interventions reported by participants and characteristics of preventive behavior at work.

Description of interventions related to prevention provided by occupational therapists in relation with preventive behavior at work characteristics.
The interpretation of the results of this study allows to understand that occupational therapists use different strategies to address the five attributes of preventive behavior at work. In addition, the involvement required by the worker is different across the various strategies; thus, the attributes are not developed with the same intensity. First, it appears that attribute #1 (compliance with rules and procedures) requires a low level of involvement from the worker, as occupational therapists can only provide correction to ensure the worker follows the rules and procedures prescribed by his job. In fact, the discourse of participants indicated that if a worker conforms to rules and procedures, occupational therapists do not specifically address this attribute with their client. Also, if the worker fails to respect a rule or a procedure, they remind him to do it properly, without further implication on his part. Second, attribute #2 (proactivity, participation, involvement, and initiatives related to prevention) and attribute #3 (maintenance of physical environment) are addressed with strategies requiring a higher involvement from the worker. In fact, the awareness and encouragement may reinforce motivation and self-efficacy toward prevention, which are antecedents of preventive behavior at work that may empower the client to adopt preventive behavior in his work tasks. Finally, the highest level of involvement from the worker is asked during interventions aiming to develop attributes #4 (concern for social environment) and #5 (reflexivity and analysis of work situations). Intervention strategies linked to the development of these attributes imply a high involvement from the worker, who must analyze his work task, evaluate the possibilities of action, make a decision, perform an action, and evaluate its impact. Burke et al. (2006) concluded, in a large meta-analysis conducted on the results of 95 quasi-experimental studies, that prevention modalities requiring a high involvement from the worker would be more effective in acquiring knowledge, changing behavior, and reducing work-related injuries or illnesses, compared with modalities that need less involvement from workers. As preventive behavior at work requires the manifestation of its five attributes [4], it would be important for occupational therapists to use strategies that demand a high involvement from the worker in the development of all attributes of preventive behavior.
Our analyses revealed that, interventions provided by occupational therapists seem intuitive. It appears that participants in the study are not aware that they are working on the antecedents or attributes of preventive behavior, neither can they link interventions provided to preventive behavior characteristics. This finding may be related to the lack of guidelines for prevention interventions in occupational therapy. In fact, practice guides in health and safety at work exist to support occupational therapists in specific interventions, such as the evaluation of work capacity of injured workers [31], the management of low back pain [32], and the support of the vocational goals of workers with mental health problems [33]. However, none is related to interventions supporting prevention and workers’ development of preventive behavior. In this sense, results of this study may provide bases to plan an occupational therapy practice guide related to prevention and to workers’ development of preventive behavior. Moreover, occupational therapists should be given professional development training so they can better understand the complexity of preventive behavior at work. Better mastery of the concept and of its main characteristics could improve prevention interventions provided to injured workers, which would reduce the risk of injuries after they return to work. Occupational therapists have the expertise to develop preventive behavior at work with their clients [4], but they must be given the resources to do so. In fact, results of a systematic review related to occupational therapists’ work-related practice revealed that knowledge on injury prevention is an important requirement to offering the best quality of practice [34].
Results of this study described the practice of occupational therapists about preventive behavior development of their worker clients. Some of the interventions identified are similar to those reported in previous studies, such as education and adaptation of workstations [7, 10]. However, this study allows to recognize new and never formally identified prevention interventions that are part of occupational therapists’ practice, such as control, awareness, and encouragement. Moreover, results of this study go further than the simple list of interventions. In fact, results interpretation makes it possible to group these interventions into strategies that reduce risks to health and safety and that promote preventive behavior among workers, which are indicative of the roles of occupational therapists, such as enablement, collaboration, adaptation, and education [35]. Results of this study provide a better understanding of current occupational therapists’ interventions about prevention at work and can serve as a basis for conceptualizing their practices within a framework that will support and improve their work.
A last interesting result that emerged from the data of this study is that, even though some occupational therapists involved in the study (i.e., those working in a private clinic) work with clients who have mental health problems, most of interventions identified are aimed at preventing physical injuries or illnesses. However, in Canada, more than 75% of absences from work are related to mental health [36], resulting in costs in excess of $20 million annually [37]. As occupational therapists are increasingly involved with a clientele living with work-related mental health difficulties and because of the holistic view of health shared by them [38], it would be appropriate to look at their practices in relation to the prevention of workplace mental health problems.
One limitation of this study to consider is the bias of social desirability that may have been present during data collection. Indeed, results of this study are based on the analysis of interview data and, possibly, occupational therapists have amplified or improved prevention interventions they put in place with their clients. Observing interventions or reading client files could have helped to reduce this bias. Also, this study reflects the reality of occupational therapists working in just one province of Canada. Results may have been different in other Canadian areas or in other countries. However, given the innovative aspect of this study on a little explored subject and the rigorous phenomenological analysis process, the scope of the results remains interesting.
Conclusion
Altough the literature suggests that occupational therapists are little involved in the prevention of work-related injuries and illnesses [15], it appears that they have the expertise to develop preventive behavior among their worker clients [4]. Integrating more prevention interventions into the practice of occupational therapists who work with workplace health and safety concerns has a significant relevance recognized by the professional community [16]. It may also reduce the financial and human costs associated with work-related injuries and illnesses [39]. Even if some studies have suggested that occupational therapists provide prevention interventions in their daily practice [7, 10] and that others demonstrated the efficacy of such interventions [12–14], the literature did not offer a comprehensive understanding of the specific practice of occupational therapists toward their clients’ development of preventive behavior at work. With this aim in mind, phenomenological analysis of interview data was conducted with 13 occupational therapists who practice in workplace health and safety and were asked to describe their daily practice toward their clients’ development of preventive behavior at work. Results of the study suggest that occupational therapists form representations of preventive behavior that are consistent with theory, but those are limited and do not take account of the complexity of the concept. Results also described eight different types of interventions provided by occupational therapists toward the development of attributes or antecedents of preventive behavior at work.
Finally, results suggest that occupational therapists recognize their role in support of their clients’ development of preventive behavior at work. However, occupational therapists may face a lack of knowledge and resources to help them in their practice toward prevention, such as the absence of a practice guide to support their interventions aiming to develop their clients’ preventive behavior at work. Also, as knowledge about injury prevention is considered a key to success in the effective practice of occupational therapists who are concerned with health and safety in the workplace [34], it is important to provide opportunities for professional development in this area. Occupational therapists’ skills development tools about prevention seems to be a promising avenue for a greater implication in interventions related to their clients’ development of preventive behavior at work. In this sense, the next step would be to plan a practice guide to support occupational therapists in their interventions related to the development of their clients’ preventive behavior at work.
Conflict of interest
The authors declare that there is no conflict of interest.
Footnotes
The masculine form is used for brevity. It should be noted that the worker may be a man or a woman.
A representation is an understanding of an abstract concept.
Sentences in quotes correspond to excerpts of transcripts of interviews with occupational therapists who participated in the study. These transcripts were translated from French into English for this publication.
Acknowledgments
The authors would like to thank all the participants of the study as well as the members of the Laboratoire de recherche en ergologie de l’Université du Québec à Trois-Rivières for the review of this manuscript.