
Abstract
BACKGROUND:
The main function of respiratory protective devices is to provide an intact physical barrier between the environment and the user. To ensure that, a leak-tight fit of the facepiece to the user’s face is essential, regardless of the user’s individual facial features.
OBJECTIVE:
The main objective of this study was to assess the possibilities of developing customized respirators well-fitting to the anthropometric dimensions of the user’s face using 3D scanning and 3D printing techniques and to evaluate this custom-made device in terms of protective, usage and strength parameters.
METHODS:
Commercially available twin-filter half-mask type MP22/2 was selected as base model for customization. The 3D scans of the half-mask facepiece were performed using ATOS Core optical 3D scanner. Simultaneously anthropometric measurements of the test subject face were carried out with hand-held 3D scanner Artec EVA. Then digital model of the facepiece was matched to the shape of user’s face using Geomagic Touch X haptic device. Customized facepieces were printed out with use of selective laser sintering technique from thermoplastic polyurethane. After assembling, respirators were tested for compliance with the requirements of the European standards.
RESULTS:
The developed respirators proved to be very well-fitted to the user’s face, did not cause any imprints or skin irritations and were assessed positively in terms of protective, usage and strength parameters.
CONCLUSIONS:
The application of 3D scanning and 3D printing techniques for designing and fabricating customized half-mask facepieces constitutes a viable option for the future development of respiratory protective devices.
Introduction
Negative pressure respirators are the most commonly used Respiratory Protective Devices (RPD). Each such device consists of at least two elements: the facepiece (i.e. full-face mask, half-mask, quarter mask, mouthpiece, hood) and the filtering element that may constitute an integral component of the facepiece (e.g., filtering half-masks) or have the form of individual particle and/or gas filters. The main function of such devices is to provide an intact physical barrier between the environment and the user. In such devices during the inhalation phase the air is sucked through the filtering element under the facepiece and enters the respiratory system of the user. In this phase negative pressure occurs under the facepiece, which may lead to the leakage of contaminated air into the breathing zone, especially when the facepiece does not fit to the users face.
In order to provide a leak-tight fit of RPD various designs of the facepiece are developed. In case of standard filtering half-masks, nose clips in the form of metal elements fixed to the outer surface of the half-mask are often used (e.g. [1]). They are usually accompanied by a polyester, neoprene or polystyrene foam tape located at the height of the nose clip on the inner surface of the half-mask (e.g. [2]). Various types of spatially formed elements are also placed at the height of the nasal bridge (e.g. [3–5]), in the upper part of the half-mask or around the periphery thereof (e.g. [6]). They are most often joined with the facepiece by means of lamination or through different types of adhesives (e.g. hot-melt adhesives). The main construction element responsible for the proper fit of reusable half-masks and full-face masks is the part that is directly adjacent to the user’s face. It is usually made of thermoplastic silicone rubber, formed by injection moulding (e.g. [7]) in a way that maximizes the contact area between the facepiece’s rim and face of the user. In some designs adhesive tapes are used to fix the facepiece on the face; however, repeated putting on and removing of such devices may cause discomfort [8].
Even if the facepiece has the best possible design, it is necessary to identify its shape and dimensions in order to adjust it correctly to the user’s facial features. Moreover, to select the equipment with the highest possible efficiency, fit testing should be performed to determine the protection factor for each individual case. Quantitative methods for determining the fit factor are based on measurements of pollutants in the atmosphere surrounding the user and in the breathing zone under the facepiece. According to European standards, fit tests of RPD are carried out in laboratory conditions using a method for determining a total inward leakage, which includes leakage through the expiration and/or inhalation valve and penetration of pollutants through filtering elements. Studies indicate, however, that the fit factor determined under laboratory conditions often differs significantly from values occurring in the workplace [9]. This problem can be solved by assessing individual fit of equipment in the workplace, under conditions of actual use. The protection factor is then determined using air aerosol and condensation particle counter, which counts particles captured from the environment and from under the facepiece of the tested equipment in subsequent cycles. This makes it possible to calculate the workplace protection factor, which is compared to the nominal protection factor, calculated as the inverse of the maximum total inward leakage as defined in the European standards for the tested kind of equipment. This method is extremely effective but rarely used by European employers due to the high cost of testing.
Another way to ensure a proper fit of RPD, regardless of the user’s individual facial features, would be to customize the facepiece itself. New possibilities in this area have emerged with the development of rapid prototyping and additive manufacturing that have lately become more and more available even for small and medium-size enterprises. In particular, 3D scanning techniques showed high precision and accuracy when compared with traditional methods for facial parameter measurements [10]. Zhuang et al. employed 3D scanning technique to collect volumetric and contour data regarding face size and shape of US respirator users to develop new head forms for RPD testing [11, 12]. The head forms are currently used in drafts of new ISO standards for determination of basic ergonomics factors of RPD.
3D digitizing design method has been used to develop three different prototypes of half-mask facepieces taking into account Korean facial characteristics. Silicon models of masks were then made via silicon moulding and evaluated in terms of comfort and fit during wear and organoleptic tests [13]. In another study, a novel method for designing and fabricating facepiece prototypes was developed to accommodate different types of face profiles. Computer tomography of a solid silicone facepiece was customized using four different computer-aided design programs. Digital representation of the facepiece was then 3D printed from non-elastic UV-cured polymer and used to prepare silicon block mould from which silicon facepieces were casted [14].
Currently, research related to the design of new PPE focuses on adaptation to the individual needs of users, in particular the size and shape of the human body. The use of new technologies such as 3D scanning and 3D printing gives more and more opportunities in this area. Despite this, there are no RPD on the market fabricated with the use of this type of technology, and literature reports in this area are very limited. Therefore, the aim of this pilot study is to evaluate the functionality of half-masks customized to the facial characteristics of specified male study participant based on 3D scans and manufactured from new rubberlike thermoplastic polyurethane by 3D printing in terms of protective, usage and strength parameters according to the European standards.
Materials and methods
The overall methodology that was used within the study is presented schematically in Fig. 1. First the test subject was selected and his face was scanned using 3D scanning method. Simultaneously appropriate RPD was selected (elastomeric half-mask) and disassembled (all removable parts were disconnected from the facepiece). Then the facepiece was 3D scanned and its digital representation was customized by modelling its geometry to provide best fit to test subject’s face. At the last stage of the study the customized halfmask was 3D printed and all parts of the mask were put together.

Schematic diagram showing the overall research methodology approach.
A professionally active, healthy, 33 year old male, who had direct contact with the RPD on daily basis (paramedic with the fire department), was selected as a study subject.
Anthropometric measurements of test subject’s face were carried out with the use of 3D scanning technique using a handheld 3D scanner Artec EVA (Artec 3D, Russia). Scanning resolution was 0.5 mm and the scanning distance varied from 40 cm to 100 cm with a minimum field of view 21.0×29.7 cm. During the scanning process the participant was seating in the upright position on a chair rotating with constant angular velocity. The participant was also instructed to have his eyes closed and to keep a neutral face expression. The total of three face scans were performed (an example is shown in Fig. 2)

3D face scan of the test participant.
After scanning the 3D model of test subject’s face was processed using Artec Studio 9 software. First outliers removal tool was applied to get rid of points that were scanned but were located outside of the user’s face. It was followed by small object filter tool in filter-by-threshold mode to remove irregularities from the processed surface resulting from scanning errors. Threshold parameter was set at 1500 polygons. Then the holes filling tool was used with maximum length of the hole perimeter set at 10 mm. The edges tool was used to identify and fill out the holes in the mesh and smooth the edges of 3D model. To correct any remaining defects manual smoothing tool was used. Then files were exported to the ‘stl’ format for further processing.
Commercially available, twin-filter, half-face respirators type MP22/2 (Maskpol, Poland) were selected for customization. The individual components of the respirator are shown in Fig. 3. The respirator consisted of stiffening – element made of polypropylene (located on the inner part of the facepiece), harness made from polyethylene and strips made of textile rubber (used to fit the respirator to the face) and the facepiece made of silicon rubber. Silicone inhalation and exhalation valves were arranged in the slots in the stiffening element.

Components of the half-face respirator (color online: valve-fixing frame – green/upper right, harness – blue/middle right, standard facepiece – red/lower right).
Before 3D scanning the half-mask was disassembled. 3D scans were performed using ATOS Core optical 3D scanner (GOM GmbH, Germany) based on triple scan technology that combines views of the object captured with use of two cameras and the projector. Projection technology is based on the use of narrow-band blue light LED, so accurate measurements could be obtained regardless of the lighting conditions. Stereo camera worked on the principle of triangulation. The band patterns projected on the surface of the scanned object were recorded by two cameras. 3D coordinates of points on the plane of the scanned object were determined from the equations of transformation for each pixel of the camera with the resolution of 0.02 mm. High resolution of scans was especially important in terms of ensuring a proper fit of the facepiece to the user’s face. A digital representation of the facepiece geometry was then saved and used as a base model for customization.
The customization was performed by digital modelling the geometry of the previously scanned base facepiece to fit it to the specific anthropometric characteristics of the participant face. The modeling was performed with the use of haptic device type Geomagic Touch X of Geomagic Freeform Plus software. The comparison of the facepiece geometry before and after customization is shown in Fig. 4.
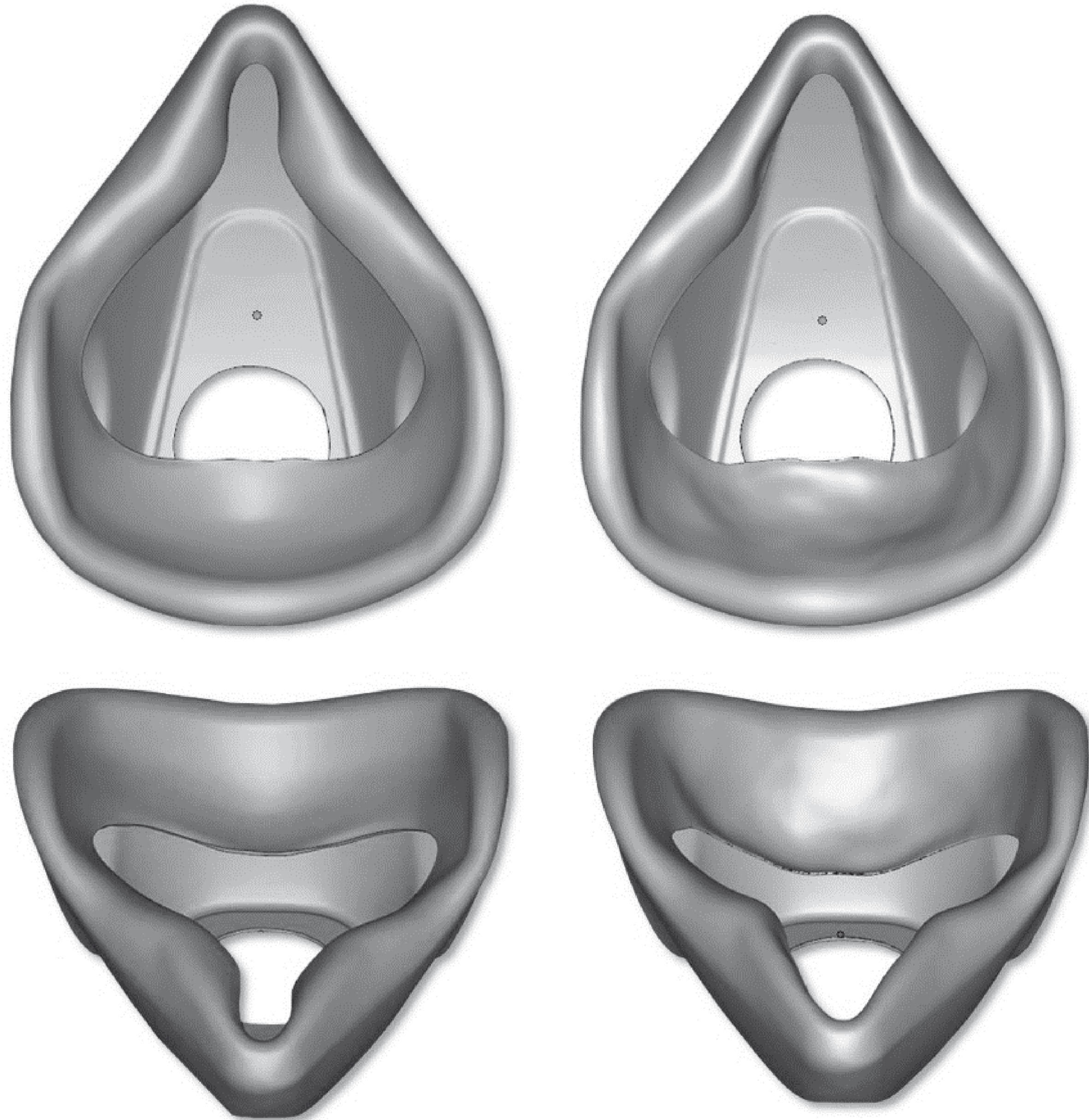
Comparison between standard (left) and customized (right) facepiece.
Five customized facepieces were fabricated using Selective Laser Sintering (SLS, technique that uses a laser to bind the powdered material together at certain points to create a solid structure) on EOS Formiga P100 3D printer. The resolution of print was 0.3 mm. To ensure full functionality of the prototypes rubberlike thermoplastic polyurethane (TPU) material type 92A-1, with permanent flexibility, high resistance to dynamic load and abrasion, rapid response to impact and operating temperature range from –20°C to 80°C, was used. Summary of the material characteristics is given in Table 1 (based on producers information [15]).
Characteristics of TPU material
After the facepieces were printed, half-masks were reassembled as shown in Fig. 5.

Components of the customized half-face respirator (valve-fixing frame – green/upper left, harness – blue/middle left, customized facepiece – white/lower left).
Customized half-masks were tested for compliance with the requirements of European standards harmonized with the Directive 89/686/EEC on conformity assessment of personal protective equipment [16]. Protective, usage and comfort as well as strength and durability parameters were evaluated. The summary of testing methodology is presented in Table 2. The results were interpreted in reference to the requirements described in EN 140 : 1998 standard [21].
Summary of the testing methodology
Summary of the testing methodology
N – as prepared (new), TC – thermally conditioned sample.
Statistical analysis was performed for half-mask performance tests where results were expressed by numeric values. Statistical analyses were conducted using STATISTICA 12 software (Statsoft, Round Rock, TX, USA). Descriptive statistics for all variables of interest were calculated.
Results and disscussion
Protective parameters
Test results of the average Total Inward Leakage (TIL) for each exercise for ten full measurements are presented in Fig. 6.
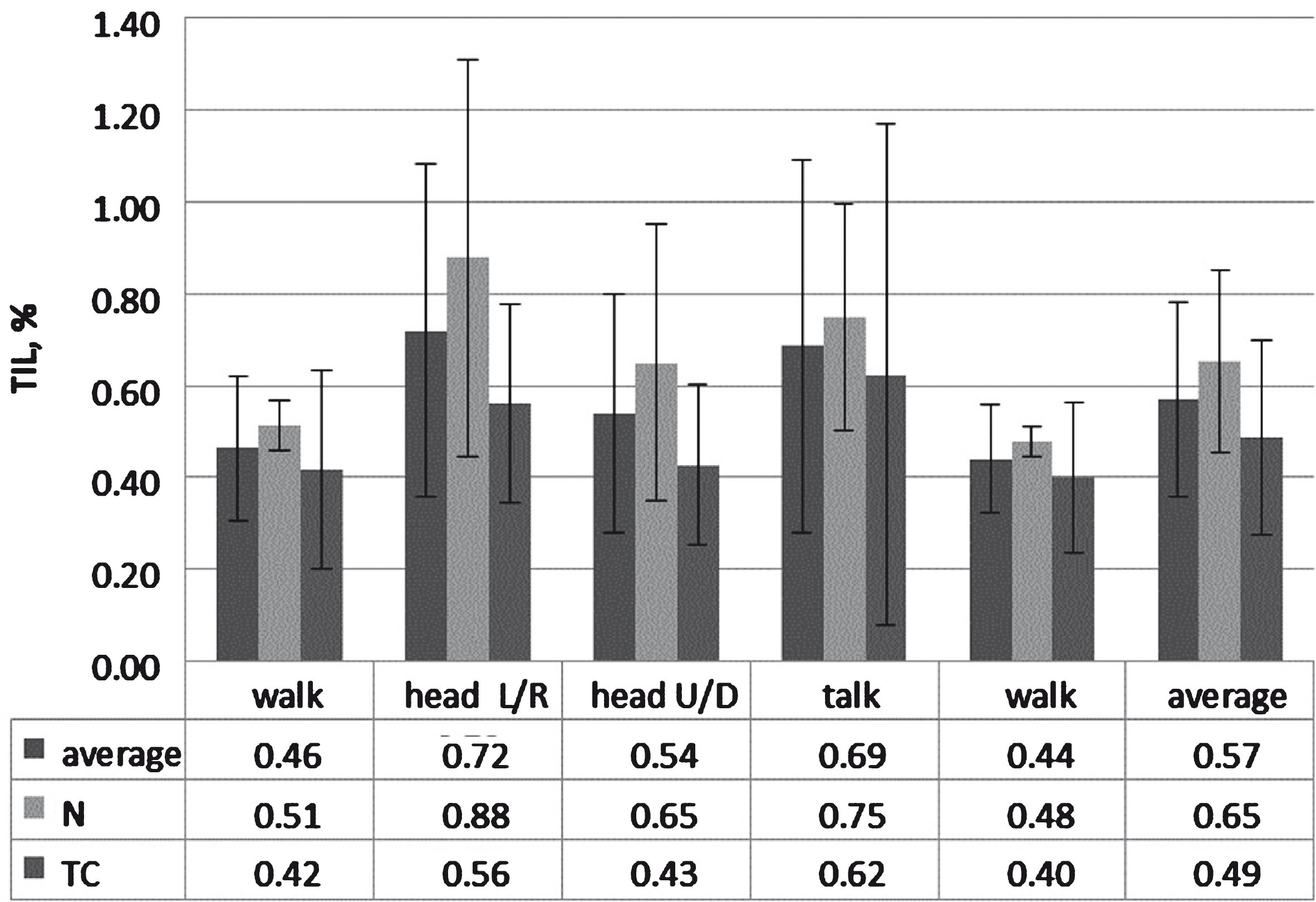
The average results of TIL for each exercise; N – as prepared (new), TC – thermally conditioned sample.
The maximum TIL noted for the 50 measurements was 1.57%, while the maximum average of the 10 measuring cycles was 0.72%. In all cases the TIL was slightly lower for the samples subjected to thermal conditioning, which may result from the increase of the plasticity of the 3D printed material after heat treatment. Both of the above results were below the limit values of the EN 140 standard that are equal to 5% for single measurement and 2 % for average TIL. Requirements of the standard have been met with considerable reserve, which is equivalent to the fact that the developed models of respirators meet the requirements of the standards of the most important protection parameter, which is the total inwardleakage.
The test results of

The test results of breathing resistance of developed models of half-masks: N – as prepared (new), TC – thermally conditioned sample.
In the case of new respirators the maximum inhalation resistance was respectively 5 Pa, 18 Pa, 39 Pa at 0.5 l/s, 1.6 l/s and 2.7 l/s. For respirators conditioned it was slightly higher and amounted to 7 Pa, 21 Pa, and 42 Pa. The observed difference could be the effect of a slight stiffening of inhalation valve discs of the half-mask and was independent of the customization process because original valves were used to assemble the customized half-mask model. The maximum resistance of the exhalation at flow rate of 2.7 l/s for the new respirator was 28 Pa, and for thermally conditioned 29 Pa. The average value was higher by 3 Pa, which may confirm earlier observations concerning the stiffening of valve discs. According to the requirements of standards mentioned above, the breathing resistance should not exceed 200 Pa for inhalation and 300 Pa for exhalation at constant air flow of 2.7 l/s. Inhalation resistance should not exceed 50 Pa at a constant flow rate of 0.5 l/s and 130 Pa with a constant flow of 1.6 l/s, which is considerably higher than the results obtained for the developed respirator model. Thus it can be concluded that the customization did not adversely influence the breathing resistance of the respirator as it fulfils the requirements of the standard.
Another important utility parameter closely linked with the shape of the facepiece is so called ‘dead space’ expressed in terms of the

The test results of carbon dioxide content in the inhaled air.
According to the European standards the average content of carbon dioxide in the inhaled air should not exceed 1.0 % by volume. Obtained average concentration of carbon dioxide in the inhaled air was 0.57% by vol. for new half-mask and 0.60 % by vol. for thermally conditioned one. The observed difference in the results confirms the earlier observation concerning the stiffening of discs of exhalation valves. Nevertheless, the change in geometry of half-masks during customization had no significant influence on the dead space of the half-mask as it fulfilled the requirements of the standard with awide margin.
Ergonomic parameters of the customized half-mask were assessed during
The results of strength and durability evaluation are presented in Table 3 along with the interpretation of the results.
Strength and durability parameters of customized half-masks
Strength and durability parameters of customized half-masks
A good quality respirator equipped with high-efficiency filters is not nearly enough to ensure a proper protection of workers exposed to dangerous airborne contaminants. Personal characteristics of users face play a vital role in this matter because they can adversely affect the fit of the protective device. In present study a new method of designing and fabricating customized RPD using 3D scanning and 3D printing techniques was described. The respirators were tested in terms of protective, usage and strength parameters according to the European standards to confirm that this newly-developed method can constitute a viable option for the future development of RPD.
Presented results show that the use of these emerging technologies to develop products for the individual protection of workers provides a huge advantage in terms of facepiece customization. The preliminary results show that the proposed approach can bring improvement especially in terms of efficiency and perception of comfort, which greatly affects the uptake of RPD. Although, the present study is limited in terms of sample size, its shows a research potential of the discussed issues and indicates the need for further exploration. Moreover, the initial conclusions are indeed promising, and particularly relevant to workers with distinct facial features.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The publication is based on the results of Phase III of the National Program “Safety and working conditions improvement”, financed in the years 2014–2016 in the field of research and development work by the Ministry of Science and Higher Education and the National Centre for Research and Development (the Program coordinator is the Central Institute for Labour Protection—National Research Institute). We would like to express our gratitude to R. Głodek, K. Bociek and P. Ćwietkowski for technical assistance during this research.