
Abstract
BACKGROUND:
Obesity prevalence in the workforce is clearly increasing. Simultaneously, manual lifting/lowering loads, referred to as Vertical Handling Tasks (VHT) in this paper, are common in industries and services. Performing VHT exposes workers to physical overload, which can be measured using a psychophysical approach. Various risk factors can increase this overload, including individual factors such as workers’ Body Mass Index (BMI).
OBJECTIVE:
To study the possible effects of workers’ BMI and some task conditions on physical overload during VHT.
METHODS:
Psychophysical data were collected from 51 participants having different body constitutions (including non-obese, overweight and obese). The participants performed 6 VHT (3 different loads ×2 workstation configurations), during which they lifted and lowered a test-box between their knees and shoulders. For each task, they reported their perceived exertion using the Borg Category Ratio-10 (CR-10) scale.
RESULTS:
The results showed that the CR-10 scale is sensitive to the variation of the task conditions tested. However, the psychophysical data pointed to a tendency to decrease the perception of physical overload as workers’ BMI increases.
CONCLUSIONS:
This may compromise the validity of the application of psychophysical data as an ergonomic approach for Work-Related Musculoskeletal Disorders (WRMSD) prevention in obese workers.
Introduction
Currently, in industrial countries, the obesity incidence has reached a high level, which is considered as the 21st century’s global epidemic [1]. This emerging problem seems to be a risk factor for occupational health and safety. For example, overweight and obese workers present greater absenteeism and for longer periods when compared to non-obese workers, with this absenteeism being frequently associated with musculoskeletal problems [2]. Low back pain is also an occupational health problem that is frequently more severe in workers with a higher BMI (Body Mass Index) [3].
In this field, different studies revealed that obesity can potentiate the occurrence of some muscular dysfunctions, for example, lower muscle strength relative to body mass [4, 5] and lower resistance to muscle fatigue [6, 7]. These dysfunctions can compromise the performance of physical activities, as well as postural maintenance. In addition, in obese individuals, the abdominal accumulation of fat mass leads to the anterior displacement of their body centre of mass, producing an adverse effect on postural stability when performing work tasks in a standing position and a higher risk of fall in works involving frequent postural changes [8, 10]. The limitations on postural maintenance and alternation may also be related to the fact that the obese present more restrictions in the ranges of motion of their body segments, owing to the accumulation of fat tissue around the joints [11, 12].
All previous findings have indicated that obesity can decrease workers’ physical capacity for occupational tasks, especially for those requiring a prolonged standing position and tasks involving significant physical effort, such as VHT (Vertical Handling Tasks). In the present study, the VHT, including lifting and lowering loads, were also considered because in addition to being very frequent in occupational contexts, they are considered one of the main causes of Work-Related Musculoskeletal Disorders (WRMSD) in the vertebral column, and in particular for the lumbar region [13].
The option to apply a psychophysical approach is based on the fact that it allows estimation of the physical overload perceived by the workers during this type of task. The psychophysical approach is considered as a subfield of psychology that establishes a relation between the stimuli and the resulting personal sensations or perception. This approach has been extensively used in previous studies focusing on VHT [14]. Psychophysical data have also been used as one of the criteria for the formulation of validated methods for assessing the risk of WRMSD in VHT, for example, in the NIOSH’91 Equation [13], the Manual Materials Handling Guide of Mital et al. [15], and the Method of Grieco et al. [16]. As a result of numerous studies in this area, there are extensive databases, as well as several multipliers and correction factors [15] that demonstrate the applicability of psychophysical data in the definition of safe limits for VHT.
In addition, Kayis and Kothiyal [17] defended that ergonomic interventions in VHT based on psychophysical criteria can produce concordant results with interventions based on biomechanical data. There is also evidence that the psychophysical approach can contribute to WMSD prevention in industrial contexts with manual handling loads [18, 19]. These proofs contradict the traditional perception that biomechanical, physiological and psychophysical approaches produced different and even contradictory results, supporting the application of psychophysical data as an important tool in the definition of acceptable limits of strength and load, or as an indicator of effort perception in preventing physical overload in occupational tasks [20]. For this purpose, there are some different techniques, such as questionnaires and scales, that have been extensively applied in quantifying physical overload and perceived fatigue during VHT, allowing the assessment of several WRMSD risk factors associated with these tasks, such as the Category Ratio-10 (CR-10) scale [21], Huskisson’s Visual Analog Scale and the Body Part Discomfort Rating Scale [22].
Psychophysical data have also been suggested as an important complement in biomechanical studies, focusing on the WRMSD risk assessment during manual handling loads [23, 24].
Regarding obesity as a potential WRMSD risk factor during manual handling loads, this has also been a factor studied through psychophysical approaches, but only a few studies have analysed the limitations and physical capacity of obese workers (Table 1). In this context, psychophysical data indicate that the increase in workers’ obesity seems to have no effect on the maximum acceptable weight during lifting tasks [25]. Another psychophysical study [26] collected data that pointed out that obese individuals report a greater perceived overload during tasks of holding loads at different static postures. As presented in Table 1, Corbeil et al. [27, 28] and Sangachin and Cavuoto [29] considered psychophysical data in addition to biomechanical data, collected during simulated manual handling tasks. In both studies the Borg CR-10 scale was used to collect the physical overload perception; however, no statistically significant differences were found in psychophysical scores between obese and non-obese workers.
Summary of previous studies that applied psychophysical approaches to study the obesity effect during manual handling loads
Summary of previous studies that applied psychophysical approaches to study the obesity effect during manual handling loads
Despite the identified need, the effect of obesity on physical capacity and musculoskeletal overload during working tasks, including VHT, is currently not well documented [26, 30]. For this reason, the main objective of the current study is to compare the psychophysical evaluation between obese and non-obese persons across different VHT. Based on this objective, two hypotheses were tested, namely, (i) the increase in workers’ BMI is related to the increase in perceived overload; and (ii) the increasing physical demands of VHT (e.g., higher loads) are related to a positively increasing trend in the psychophysical scores.
Participants and tasks studied
Primarily in order to test the experimental procedure, a pilot study was developed with a small sample of 14 participants [31]. In the current study, a sampling procedure with BMI classifications as the stratification variable was used to recruit a total of 51 participants (26 males and 24 females) with a mean age of 32.8 (±9.6) years old. According to participants’ BMI, and by applying the WHO [1] criteria orientations, the sample was divided into two groups, specifically non-obese (24 participants with BMI < 25 kg/m2) and overweight and obese (26 participants with BMI≥25 kg/m2). Participants were excluded if they have had any chronic or acute musculoskeletal injuries (assessed through a self-report questionnaire). The other criteria for participants’ selection were as follows: within the working age, and profession with similar physical requirements. In addition to BMI for the characterization of the sample, abdominal circumference (AC) and percentage of body fat mass (% BFM through the bioelectrical impedance technique) were also determined for each participant (Table 2). This last-mentioned parameter was quantified through an OMRON BF306® Body Fat Monitor (OMRON, Netherlands). This equipment allows for measurement of the % BFM integrating personal data, such as the participants’ height, weight, age and gender, in order to accurately define the individual obesity level [32]. It should be highlighted that the results obtained by this equipment are in line with the stratification sample based on BMI, and similar correlations between these anthropometric data were found in previous studies [25, 33]. However, the comparative study or correlation between these anthropometric data is not one of the objectives of the present study. These different data were only considered with the purpose of characterizing and categorizing the sample in a more complete way, as defended by Singh et al. [25].
Mean and standard deviation (SD) of the parameters used for characterization of the sample (n = 51)
Mean and standard deviation (SD) of the parameters used for characterization of the sample (n = 51)
In a laboratory setting and after signing an informed consent, each participant was requested to perform 6 vertical handling tests (3 loads×2 workstation configurations) of lifting a box between knees height and shoulders height, with subsequent lowering to the original position. As in several studies focusing on the physical overload assessment associated with this type of task [25, 36], the VHT amplitude was defined based on participants’ anthropometric data. The participants stood in front of the test box, which was placed on a platform that located the box handles close to the participants’ knee height. The simulated VHT were performed with both hands and in the sagittal plane. It should be noted that this experimental design takes into account the most frequent VHT developed in real workplaces [37, 38]. Concerning the foot position, it was also defined by each participant in order to maintain the load close to the body and maintaining the same position across the lifting and lowering of the same test (as applied by Sangachin and Cavuoto [29]). With this purpose, before the data collection, participants were allowed to simulate the task of box lifting and lowering without load.
The three different loads considered were 5, 10 and 15 kg, with the difference of 5 kg between loads being defined as per the recommendation of Karwowski et al. [37]. According to these authors, it is necessary to have a minimum difference of 1.8 kg between the loads, so that the participants can properly distinguish their perceived effort during VHT. These loads also respected the recommended weight limit set by the NIOSH Equation [13].
The two workstation configurations consisted of performing the task with and without a physical barrier (between the load and the participant’s body) (Fig. 1). This high barrier (at a height of 60 cm from the floor) was used to replicate an industrial bin, as studied by McKean and Potvin [35] and Ciriello [38]. The barrier was constructed considering the anthropometric data of the Portuguese population [39], as the participants were all Portuguese and their stature was included in 90% of the stature’ values of this population, so the barrier exceeded the participants’ knee, and acted as a similar constraint for all participants. The use of this barrier could be more physically demanding because this condition compromises the knee flexion, increasing the trunk flexion and the trunk muscle overload, as evidenced in McKean and Potvin [35]. In addition, the barrier leads to an increase in the horizontal distance between the workers’ hands and the lumbar spine, increasing the overload associated with these tasks [13], especially for overweight and obese workers given the accumulation of fat mass in the frontal region of the body [40].

Experimental apparatus in the box reach moment (a) without and (b) with the high barrier.
The order of the presented tasks was randomly changed between different tests. The reason for this was to avoid the same order for all participants. For example, if participants were always requested to start with the easiest condition in terms of load and finish with the most difficult, the reported perceptions could be biased.
With the aim of simulating a realistic working performance, the participants were allowed to adopt their preferred handling technique relative to the posture adopted and velocity of movements, according to their individual capacities, as defended by Plamondon et al. [41] and Shanahan et al. [24]. A rest period of 60 seconds was established at the end of each test, in order to record the psychophysical data and to avoid physical fatigue, as described by Singh et al. [25]. In addition, each task was performed only once by each participant because it is known that increasing the handling repetition decreases the workers’ psychophysical capacity owing to an increase in muscular fatigue, as shown by Pinder et al. [42]. More importantly, according to Garg et al. [18], psychophysical studies are valid in tasks with intermittent muscle work (as in the present study) as well as in repetitive tasks within a given period of time.
The participants reported their perceived exertion using the CR-10 scale [21], from 0 to 10 points, to which the number 10 implies the perception of an extremely high physical intensity, similar to the effort of running for a few minutes at the fastest possible speed or to manual lifting and/or carrying very heavy loads. This score of 10 is close to the maximum effort a given person has ever experienced.
Borg [21] argues that the application of these types of scales is necessary as a way to quantify subjective sensations of physical overload, such as the perception of effort and discomfort. An advantage of the CR-10 scale is the fact that each score is associated with an effort that is well perceived by different individuals, allowing the use of these values as a reference for various comparisons, such as the physical effort between different workers. This scale has been widely used in the quantification of physical overload and perceived fatigue during VHT by individuals with different levels of obesity [26, 29]. Furthermore, this evaluation of individual overload without the use of direct measurement equipment on the participants’ bodies facilitates the data collection procedure and is a more realistic simulation of the considered tasks [14, 24]. It should be highlighted that previous results [41, 45] demonstrated that the CR-10 scale is a reliable and valid tool for monitoring the perceived exertion during ergonomic interventions at work, and its application has been suggested for estimation of the WRMSD risk level through the workload self-assessment by workers exposed to manual handling of loads [19].
The Borg CR-10 scale was affixed within the participants’ field of view and was presented and explained to the participants before the tests. As each test involved lifting followed by lowering, it was requested that the psychophysical evaluation be made considering the two different movements or tasks, with the participants assigning a score for each of them separately.
Regarding the statistical analysis, IBM® SPSS® Statistics 24.0 software was applied. Primarily, a division of the sample into two groups (non-obese and overweight/obese, as mentioned above) was made for descriptive statistics of the psychophysical scores distribution, considering the medians, as well as the maximum and minimum values.
The possible correlation between the participants’ BMI and the psychophysical scores was explored by computing the corresponding Spearman Correlation coefficients. The BMI was the anthropometric variable used in this correlation because it is a linear variable, independent of participants’ age and gender and, in the current sample, it is in accordance with the obesity levels definition by bioelectrical impedance. The application of the Spearman test is justified by the fact that it was intended to verify the correlation between a variable expressed along a numerical scale (BMI as the independent variable) and variables measured on an ordinal scale (such as psychophysical scores, as dependent variables) [46].
The medians of psychophysical scores between different data groups were also compared, in order to test the existence of significant differences between the following: The levels of obesity of the participants, constituting two independent groups (non-obese versus overweight and obese, in this case according to BMI); lifting and lowering tasks, constituting two dependent groups of related data, because the tasks are performed by the same individuals who assign the scores; workstation configurations, i.e., with and without the obstacle, separating the data into two related groups for the same reason presented in the previous paragraph; loads of 5, 10 and 15 kg, considering three groups of related data, assuming that the scores are perceived and assigned by the same individuals.
For this purpose, different non-parametric tests were applied, as the scores constitute variables expressed in an ordinal scale. The selection of these tests, represented in Fig. 2, was supported by the number of groups of data compared, as well as by whether or not the datasets were related (paired) [47]. For all statistical tests, a probability p (p-value) of less than 0.05 was considered significant statisticalevidence.
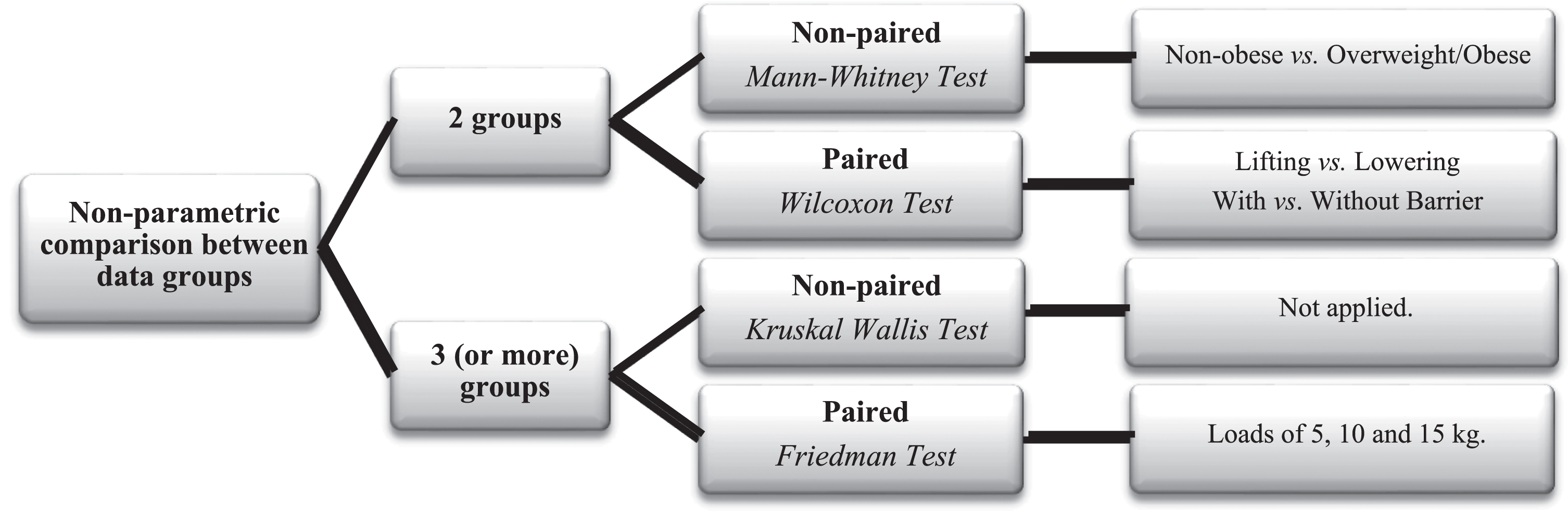
Selection of the non-parametric statistical tests used to compare the psychophysical results across different data groups.
Workers’ BMI and perceived exertion
As mentioned, the Spearman test was applied in order to determine if the increase in the workers’ BMI correlates positively or negatively with the psychophysical scores. Table 3 lists the statistical significance summaries of the correlations between the workers’ BMI and the Borg CR-10 scores, obtained through the statistical test for each VHT studied.
Correlation between workers’ BMI and psychophysical scores CR-10 (n = 51)
Correlation between workers’ BMI and psychophysical scores CR-10 (n = 51)
Legend: ρ – Spearman coefficient of correlation; *significant at p < 0.05.
According to data previously obtained by Ayoub and Dempsey [14], the psychophysical data are dependent on the workers’ physical constitution. According to the authors, a good physical conditioncan increase the psychophysical capacity in the VHT.
In the current study, it was expected that the increase in workers’ obesity, reflected in the increase in their BMI, was positively correlated to the increase in psychophysical scores (as evidenced by Park et al. [26]). A hypothesis that was tested was that the obesity condition is associated with the increase in workers’ perceived exertion. However, the results obtained do not seem to support this premise. According to Table 3, there are statistically significant correlations in the opposite from expected direction; in this case, an increase in BMI is negatively correlated to the increase in psychophysical scores, evidenced in tasks involving higher loads (10 and 15 kg). This evidence is closer to the results obtained by Singh et al. [25]. These authors demonstrated that the increase in workers’ BMI does not influence the maximum acceptable weight for loads during lifting tasks. As in the current study, Singh et al. [25] tested VHT and evidenced that obesity does not seem to be a factor that diminishes the perceived ability to perform this type of task. As supported by the referred authors, these results may be related to the fact that overweight and obese workers are continually exposed to a greater physical overload owing to their excessive body weight, and therefore, they may differ from non-obese workers in the individual judgment criterion for defining acceptability of perceived exertion during VHT and probably have laxer criteria. Second, previous psychophysical comparisons using scales (visual analogue or category) seem to show that obese individuals present alterations of stimulus-response characteristics for different physical stimuli [48]. These results may compromise the validity of using the Borg CR-10 scale as an ergonomic approach in WRMSD prevention in workers with higher levels of BMI.
Data obtained in previous studies also seem to indicate that the exertion perceived by the overweight and obese workers is more aggravated during tasks with a predominance of static muscle work (as verified by Park et al. [26]), compared with dynamic tasks such as VHT (as evidenced in the present study and in Singh et al. [25]). This is supported by other studies [5, 6] that have demonstrated that obese workers have certain muscular dysfunctions, such as a lower strength relative to body mass and a lower resistance to muscular fatigue, during the performance of isometric muscular contractions. It should be noted that even in VHT tasks, when these involve a high repeatability and are developed for longer periods, the psychophysical capacity in overweight and obese individuals can be reduced, as evidenced by Sangachin and Cavuoto [29].
In order to better understand the psychophysical scores distribution, the sample was divided into two groups of individuals according to their level of obesity (categorized according to their BMI). The distributions of the medians and minimum and maximum values of these scores for each group are presented in Table 4.
Medians (maximum; minimum values) of psychophysical score distributions between groups defined by workers’ BMI
Through the descriptive analysis of Table 4, it can be observed that the medians between the two groups are close, not evidencing a significant difference. This was confirmed by the Mann– Whitney statistical test, which showed that the difference between the medians of the two groups is not statistically significant. It is concluded that there is variation in the psychophysical scores throughout the sample of participants with different BMIs (according to the Spearman test, as presented in Table 3), but there are no significant differences between the medians of the different groups defined.
Similar results were obtained by Sangachin and Cavuoto [29], and these authors verified that in relation to the perception of effort along repeated manual tasks, there were differences between the CR-10 scores given by obese and non-obese individuals; however, this difference between groups did not reveal statistical significance.
In order to verify if certain task conditions during VHT, such as higher loads and/or workstation configurations with physical barriers, are related to the increase in the psychophysical scores assigned by individuals with different physical constitutions, different statistical tests were applied (describedin 2.2).
Regarding the distribution of scores between groups of data segregated by the presence or absence of the physical barrier in the workstation configuration, the Wilcoxon test demonstrated that there are significant differences across all tasks tested, as evidenced in Table 5, with a slight increase in the scores for the barrier configuration, compared to the without-barrier configuration. The physical barrier between the load and the worker enhances the horizontal reach range during the VHT. This occupational condition is frequent in real occupational contexts and increases the biomechanical overload during these tasks [35]. According to the data obtained, this condition also significantly influences the perceived exertion during the tested tasks. This evidence is in line with the results obtained by Ciriello [49], which demonstrated that the increase in the horizontal distance (obtained by placing a physical barrier similar to that used in the current study) decreases the maximum acceptable weight of workers performing tasks involving manual lifting loads.
Comparison of the psychophysical scores between the workstation configurations without and with barrier, as well as between lifting and lowering
Comparison of the psychophysical scores between the workstation configurations without and with barrier, as well as between lifting and lowering
Legend: *significant at p < 0.05; **significant at p < 0.001.
In addition, the Wilcoxon test attempted to compare the scores assigned to tasks of lifting and lowering (Table 5), and it was verified that for some of the tasks tested, there are significant differences in which the scores tend to be slightly higher for lifting in comparison with lowering tasks in the same occupational conditions.
In this area, Lee [50] also verified that in lifting tasks, there is a significant increase in the minimum acceptable duration of intervals between handlings, compared with lowering the same load. These results demonstrate that workers need more time to recover when lifting, compared to lowering. This evidence is supported by the fact that between lifting and lowering, the activated muscular mechanisms are different, as supported by McKean and Potvin [35]. Another study [49], by using a psychophysical approach, verified that the maximum acceptable weight is significantly higher for lowering, in relation to lifting in the same occupational conditions. Thus, the psychophysical data collected in the current study seem to be in agreement with those previous results.
However, it should be noted that this difference in the score distributions between lifting and lowering is significant only in the more biomechanically favorable tasks, involving the handling of lighter loads (5 and 10 kg) without a barrier. In the most demanding tasks, with higher loads and with a physical barrier, exertion perceptions are similar between lifting and lowering the same load. In these tasks, the load and the barrier seem to assume a greater influence on the psychophysical scores.
Finally, by applying the Friedman test, it was found that there are statistically significant differences between the scores assigned to all handling tasks with different loads, in this case 5, 10 and 15 kg (Table 6). As expected, the increase in the load handling increases the CR-10 scores significantly, evidencing the sensitivity of these psychophysical data to this task condition [14].
Statistical significance of the comparison of psychophysical scores between loads
Legend: **significant at p < 0.001.
At the beginning of the study, the results presented above were expected, namely, the effect of the physical barrier, the difference between lifting and lowering the same load and the effect of the load on the perceived exertion during VHT, considering a heterogeneous sample according to workers’ BMI, including non-obese and overweight/obese workers. However, as mentioned previously, there were no significant differences in psychophysical scores between these two groups. Thus, it is possible to conclude that the CR-10 scale allows differentiation of the task conditions tested, considering the scores of all individuals, regardless of their physical constitution. Consequently, it is concluded that these psychophysical approaches in WMSD risk assessment studies and ergonomic intervention in VHT may not be advisable when obese workers are involved. In these cases, as advocated by previous studies [23, 27], it is considered essential that the use of psychophysical data, such as the Borg CR-10 scale, can only be used as a complement in a biomechanical study that considers the evaluation through other techniques, such as electromyography or kinematic analysis.
There are limitations that should be discussed with respect to this study. First, most VHT in workplaces are not scaled. It is also likely that differences may exist for all obesity levels between tasks with different constraints and loads.
However, the results of the current study and the data obtained in previous studies point to the lack of concordant conclusions about the effect of obesity on the psychophysical scores associated with performing manual tasks. Accordingly, a proposal for future work might be the application of other psychophysical data collection techniques to study this, as depicted previously by different studies [22, 51], such as the Visual Analog Scale and/or the Body Part Discomfort Rating Scale, which may be more sensitive in the evaluation of the effect of obesity during VHT. These scales could complement the results obtained by the Borg CR-10 scale. Another proposal could be to verify the validity of the CR-100 scale [52], as this is a scale with a greater range of scores and is thus more sensitive to differences between medians assigned between individuals with different constitutions and physical abilities.
In addition, based on previous results [18, 42], the tasks were performed only once by each participant, in order to avoid muscular fatigue, because the present study was intended to test different occupational conditions. A future study might collect psychophysical data after the repetition of these tasks, so that the participants might create more rigorous judgments about their physical exertion. However, this experiment should be conducted across various time periods or days to avoid muscular fatigue. This procedure was not possible in the current study as it was very challenging to recruit obese volunteers. At the same time, increasing the sample size might be an important objective for future investigation.
Another factor that could be improved in a future study is the participants’ physical condition assessment. As mentioned above, in the present study, a number of criteria were considered at the sample’s constitution (e.g., having an identical profession, no musculoskeletal disorders), and different anthropometric data were collected in order to support the stratification of the sample into non-obese and obese workers (as the bioelectrical impedance that supported the BMI classification). Nevertheless, in a future psychophysical study, a specific questionnaire for the physical condition assessment might be applied.
It is also acknowledged that the current study did not investigate the lifting/lowering motion patterns adopted by the participants. This study is limited in that only the psychophysical approach was considered. In the future, biomechanical and physiological studies should be developed to provide a more complete understanding of the obesity effects on human lifting/lowering capabilities.
In short, at this point of time, the possibilities described above remain hypotheses to be tested, and the current study can be seen as a good starting point for future investigation in this research field. Future studies for testing these hypotheses are needed; this requires further research in order to understand the obesity effects on the biomechanics, physiology and psychophysics of VHT.
Conclusions
The association of obesity with several pathologies, such as cardiovascular, oncological and musculoskeletal, has been clearly demonstrated. In occupational contexts, the prevalence of obesity in the working population is relevant and tends to increase. However, this factor can have a negative impact on the working capacity of individuals. Based on this evidence, during VHT, it was expected that overweight and obese workers’ perceived exertion was higher when compared with that of non-obese workers. However, according to the collected psychophysical data (through the Borg CR-10 scale), there was a tendency for workers with a higher BMI to report lower scores. These results may be related to the fact that overweight and obese individuals are continually exposed to greater physical overload, mainly because of their excessive body weight. For this reason, their personal effort criteria are likely to be different compared to non-obese individuals. This study shows that special attention should be paid to overweight and obese workers, and the use of a psychophysical approach to assess risk with these workers does not seem to be the best strategy for a field risk assessment.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This work has been supported by FCT – Fundação para a Ciência e Tecnologia within the Project Scope: UID/CEC/00319/2019. The authors want also to acknowledge the work of the participants, who volunteered to participate in this experimental study.