
Abstract
BACKGROUND:
Healthcare workers experience a disproportionately high frequency of workplace assaults. Incidents involving firearms are of particular concern.
OBJECTIVE:
To provide detailed characterizations of recent hospital shootings to better inform prevention and mitigation strategies.
METHODS:
Quantitative content analysis of reports involving hospital shootings resulting in casualties derived from web searches for each year from 2012–2016. Data were abstracted independently by two investigators, with differences resolved by consensus. Data were compared between subgroups by chi-square test, Fisher’s exact test, or Kruskal-Wallis test, as appropriate.
RESULTS:
Eighty-eight shootings occurred in 86 hospitals resulting in 121 firearms-related casualties, including 54 victims and 67 perpetrators. Case fatality rates were 55.6% (n = 30) and 70.1% (n = 47), respectively. The most frequent sites involved were the emergency department, (n = 27, 30.3%), patient room (n = 19, 21.3%), and parking lot (n = 13, 14.6%). Grudge (n = 17, 19.3%), suicide (n = 14, 15.9%), and mental instability (n = 13, 14.8%) were the most common explanations for these shootings. Four inadvertent discharges occurred and were more likely to involve a female perpetrator (p = 0.03). Shootings were most frequent during summer (p = 0.03) and winter (p = 0.04).
CONCLUSIONS:
Out study findings on location and seasonal patterns can guide the development or improvement of prevention and mitigations strategies for hospital shootings.
Introduction
Although the frequencies of both fatal and nonfatal workplace violence in the United States have declined by two-thirds over the past two and one-half decades, violent incidents in the healthcare workplace doubled from 2012–2014 [1, 2]. Moreover, while healthcare workers comprise 13% of the U.S. labor force, these individuals experience 60% of all workplace assaults [3]. Firearm-involved incidents have received special attention, particularly in the healthcare settings [4–6]. During 2000–2011, 154 shootings associated with 235 casualties and a 55% case fatality rate among victims were reported in U.S. acute care hospitals [7]. Considering the markedly increased frequency of active shooter events, number of accompanying casualties, and incidents involving health care facilities, we sought to provide detailed characterizations of acute care hospital shootings to better inform prevention and mitigations strategies [8].
Methods
Quantitative content analysis methodology was used to review reports of acute care hospital shootings available online. Individual searches for the terms “hospital shooting,” “hospital violence,” “assault on healthcare provider,” shooting of healthcare worker,” and “guns and hospital” were conducted for each year from 2012–2016 using Google, Bing, AOL, and PubMed. Data sources were news bulletins and articles posted on television and newspaper websites. Incidents were included if they occurred in or on the grounds of a U.S. acute care hospital and involved at least one gunshot casualty whether caused by the perpetrator discharging a weapon or by law enforcement shooting an assailant. Multi-site shootings were included if at least one segment of the crime met inclusion criteria. Firearms discharges without any injuries or mortalities were excluded. Shootings in psychiatric or rehabilitation hospitals, skilled nursing facilities, or off-campus physician offices were also excluded. If all required data were not available in the sources identified in the initial search, secondary searches were performed using the same search engines employing the incident date, hospital name and location, or perpetrator name.
Data were abstracted independently by two investigators with differences resolved by consensus. Shooting locations were described by geographic region using the U.S. Census Bureau classification, with population-based frequencies determined using U.S. Census Bureau regional population estimates for each year of the study period [9, 10]. Locations were further categorized as urban or rural based on the 2010 U.S. census data. Shooting sites were also described by hospital size according to the number of beds, location within the hospital or grounds where the shooting occurred.
Perpetrators were described by age, gender, relationship to the hospital workplace, and apparent motive. The perpetrator’s relationship to the hospital workplace or its employees was classified using the system described by the National Center for the Analysis of Violent Crime [5]. Type 1 violence represented criminal behavior by an individual with no relationship to the workplace or its employees. Type 2 violence was perpetrated by workplace customers. We included patients, family members, and visitors of patients in this category. Type 3 violence was perpetrated by current or former coworkers, and Type 4 activity represented violence involving an individual who is not employed in the workplace but has a personal relationship to an employee. When an incident could be characterized by more than one type of violence, it was classified according to the primary apparent motive. For example, if the perpetrator and victim were both hospital employees and were involved in an intimate relationship, the incident was categorized as Type 4 rather than Type 3 violence.
The apparent motive or explanation for each occurrence was categorized using a previously described system [7]. Grudges were defined as incidents with an apparent revenge motive as well as those representing intimate partner violence. Shootings of ill relatives were defined as likely euthanasia. Attempted or actual escape of a patient from law enforcement or correctional authorities merited its own category. Social violence was defined as violence that had spilled over from the surrounding community onto the grounds or into the confines of the hospital that was otherwise unrelated to the workplace. Shooting incidents in which the perpetrator exhibited bizarre behavior in the absence of another apparent motive were defined as mental instability. We modified this classification system by adding a category for inadvertent firearm discharges resulting in a casualty.
Casualties were classified as either injury or death of the perpetrator or victim(s) that were a direct result of firearm discharge. They were further described by gender and by their relationship to the hospital workplace or its employees. The type and source of weapons involved in the shooting incident were recorded, when available. The date of each incident was recorded. In order to examine a seasonal relationship for shootings, winter months were defined as December-February, spring as March-May, summer as June-August, and fall as September-November.
Data were summarized using descriptive statistics. Dichotomous variables were compared by the Fisher exact or Chi-square test, as appropriate. Seasonal variations in event frequency and motives were examined first using the Kruskal Wallis test, with subsequent pairwise analysis by the Fisher exact test with Monte Carlo estimation. Trends in annual shooting frequency were examined over the study period by the Spearman correlation. Significance was considered as p < 0.05.
Results
Frequency and location of shootings
Eighty-eight incidents involving 88 perpetrators and 86 hospitals met inclusion criteria during the five-year study period, resulting in 121 firearms-related casualties including 54 victims and 67 perpetrators. Two hospitals experienced two shootings. There were 4769, 4753, 4676, and 4648 acute care hospitals registered with the American Hospital Association in 2012, 2013, 2014, and 2015, respectively(American Hospital Association, personal communication, August 31, 2017). As 2016 data were not available, we used 2015 data as an estimate for 2016. Thus 1.8% of U.S. acute care hospitals experienced at least one shooting during the study period, representing an average rate of 0.38% (1/263 hospitals) per year. Fourteen shootings occurred in the northeast (0.50 incidents per ten million population per year), 36 in the south (0.60 incidents per ten million population per year), 19 in the Midwest (0.56 incidents per ten million population per year), and 19 in the west (0.51 incidents per ten million population per year). There was no significant difference in the occurrence rate by region, p = 0.81. Eighty-six (97.7%) shootings were in urban settings. Eleven (12.5%) incidents involved hospitals with fewer than 100 beds, while 42 (47.7%) involved facilities with 100–399 beds, and 35 (39.8%) occurred in hospitals with at least 400 beds. The frequency of shootings by year and by location inside or outside of the hospital is described in Fig. 1. The emergency department, patient rooms, and the parking lot represented the most common shooting sites, together accounting for 59 (66.2%) incidents (Table 1). Overall, among the 88 incidents occurring in 89 locations, 72 (80.9%) shootings occurred inside and 17 (19.1%) shootings occurred outside of the hospital building.

U.S. acute care hospital shootings by location and year.
Locations of U.S. acute care hospital shootings, 2012–2016
*One incident involved both the parking lot and an unspecified inside location.
The mean age of 73 perpetrators with this demographic available was 45.3±18.4 years, ranging from 16 to 88 years. Seventy-nine (89.8%) perpetrators were male, 7 (7.9%) were female, and in two (2.3%) cases gender was not specified. Grudge represented the most common motive for shootings, followed by suicide and mental instability, together accounting for 44 (50.0%) incidents (Table 2). There were four inadvertent discharges of firearms brought into a hospital despite applicable federal or state law, or local hospital policy that banned weapons from hospitals. The first case occurred when a gun fired after it was brought into a magnetic resonance imager by a patient. The discharge resulted in self-injury. The second instance was an accidental discharge of a firearm in a restroom by a licensed concealed carry permittee that injured a bystander. A third incident resulted from a hospital employee dropping a backpack containing a firearm that discharged, wounding the employee. The final inadvertent discharge occurred after a woman dropped her purse containing a gun, wounding her 2-year old child. Inadvertent discharges represented 2 of 7 (28.6%) shootings involving female perpetrators compared to 2 of 79 (2.5%) shootings involving male perpetrators (p = 0.03).
Apparent motives and explanations for U.S. acute care hospital shootings, 2012–2016
Apparent motives and explanations for U.S. acute care hospital shootings, 2012–2016
The most common form of workplace violence observed was Type 2, or customer-perpetrated. The most frequent forms of unclassified violence involved the perpetrator as victim and inadvertent discharges (Table 3). No shootings represented mass killings, defined as those in which at least three persons died. The total of 54 victims included 18 (33.3%) staff and 36 (66.7%) patients, visitors, and others (Table 4). The case fatality rate for victims was 55.6%, including 55.6% for staff and 55.6% for others (p = 1.0). There was no significant difference in mortality by victim gender, which included 12 of 23 (52.2%) males and 18 of 27 (66.7%) females, (p = 0.30).
Workplace violence classification of U.S. acute care hospital shootings, 2012–2016
Workplace violence classification of U.S. acute care hospital shootings, 2012–2016
*2 inadvertent discharges resulted in self-injury. These incidents were categorized as inadvertent discharges and were not additionally counted under self as victim.
Victim outcomes, U.S. acute care hospital shootings (n = 88), 2012–2016
The most common perpetrator outcome was actual or attempted suicide (Table 5). Of the 34 attempted suicides, 31 (91.2%) were successful. In total 67 (76.1%) perpetrators were shot to end the incident, including 34 intentional and two unintentional self-inflicted wounds, 30 by law enforcement, and one by an armed physician. The case fatality rate was 47 of 67 (70.1%) for perpetrators who were shot and 48 of 68 (70.6%) when including an additional perpetrator death from tasing by law enforcement. Excluding suicides and attempted suicides, the corresponding perpetrator case fatality rates were 48.5% and 50% respectively. The perpetrator case fatality rate did not significantly differ from that of victims, whether (p = 0.10) or not (p = 0.52) suicides were included. The overall firearms case fatality rate including victims and perpetrators was 63.6%.
Perpetrator outcomes, U.S. acute care hospital shootings, 2012–2016
Seventy-six (86.4%) perpetrators were known to have possessed weapons at the time of the shooting, of which 68 (89.5%) were firearms and eight (10.5%) were edged weapons. Five (7.4%) of the 68 firearms possessed by criminals were stolen from on-site security, law enforcement, or corrections department personnel, while the remainder were brought to the hospital by the perpetrator. Four of the five firearms stolen from law enforcement were fired by perpetrators, killing one and wounding three police officers.
Temporal occurrences of shootings
Overall, there was a significant (p = 0.03) seasonal variation in shooting incidents (Fig. 2). Pairwise comparisons between seasons confirmed significant increases in winter (median number of events = 5, range = 3–12) compared to spring (median number of events = 1, range = 0–4), p = 0.04. Summer (median number of events = 6, range = 3–9) was associated with significantly more incidents than either fall (median number of events = 3, range = 2–5, p = 0.04), or spring (median number of events = 1, range = 0–4, p = 0.03). While motives did not vary significantly by season (p = 0.13), the most common motive observed in winter and fall was grudge, accounting for 31% and 23.5% of shootings, respectively. In summer months, mental instability (31.3%) and suicide (18.8%) were the most frequent motives.
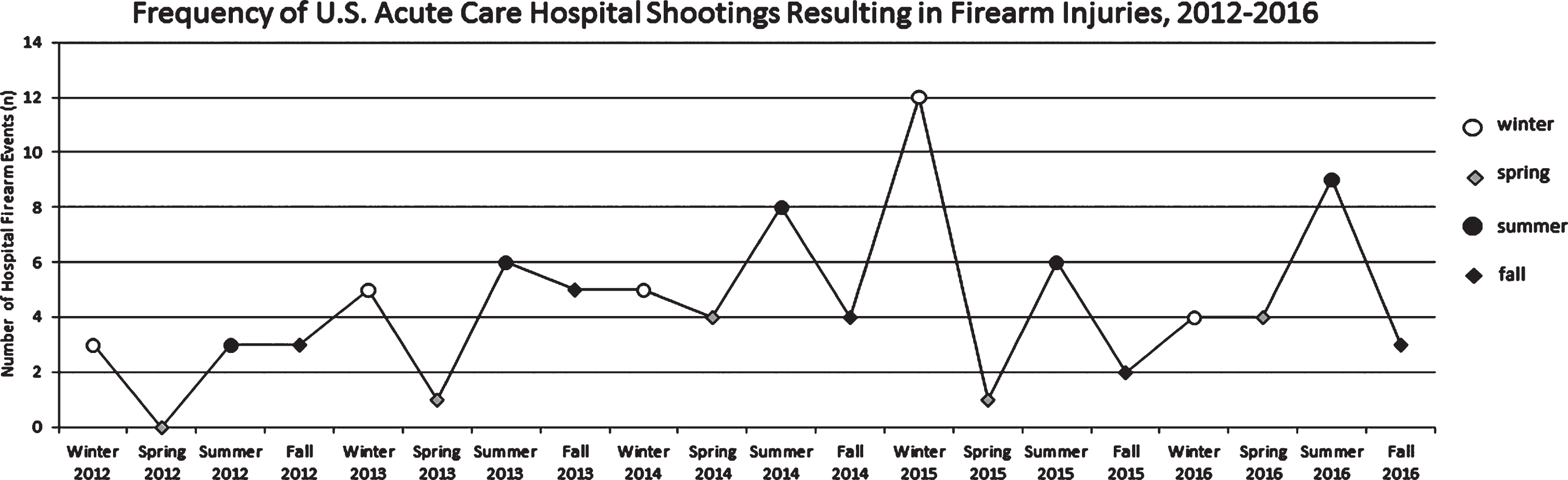
Frequency of U.S. acute care hospital shootings resulting in firearm injuries, 2012–2016.
We report for the first time a seasonal variation to hospital shooting incidents, with significantly increased frequencies during summer and to a lesser degree, winter months. This phenomenon is consistent with recognized patterns of violent criminal behavior. U.S. Department of Justice data from 1993–2010 National Crime Victimization Surveys, which evaluate nonlethal crime, noted increased rates of aggravated assault and intimate partner violence during the summer months [11]. A recent study of 88 large U.S. cities examined the seasonality of assaults and homicides from 1964–2004. Both crimes peaked in July with a second homicide peak in December [12]. These findings are not unique to the U.S. as evidenced by data from Italy showing homicides peaking in July and August, followed by December and January [13].
Several theories have attempted to explain the seasonality of violent crime including variations in environmental conditions and patterns of human social interactions. The summertime peak in violence is associated with increases in ambient temperature. Basu, et al. examined the association between emergency room visits for mental health issues, self-harm/suicide, and intentional injury/homicide in California from 2005–2013. The authors observed 4.8%, 5.8%, and 7.9% increases in visits for these indications, respectively, with ≥10°F rises in mean daily temperature [14]. Two other investigations also noted increased suicidality with seasonality and increases in ambient temperature, independent of daily sunlight duration [15, 16]. These findings are congruent with our observation of mental instability and suicide representing the leading motives for summer month hospital shootings. In contrast, the winter homicide peak has, at least in part, been attributed to Christmas holiday-related increases in social interactions coupled with prevalent alcohol use [12]. Regardless of the causes of seasonal variation to hospital shootings, this recognition may inform the need for security and law enforcement training in prevention and mitigation that occurs prior to the peak seasons and takes into account the locations and reasons for the shootings. Additionally, these findings may guide the selection of locations monitored by security and law enforcement, as well as staffing numbers of security personnel. As 72 (80.9%) of shootings occurred inside the hospital in at least 13 different locations, centralized controlled entry points should be considered. Suggested means include security check points and screening of individuals entering the premises, staff use of electronic card keys, and easily deployed devices that effectively secure interior doors to specific units [17]. The emergency department, where 27 (30.3%) shootings occurred deserves specific attention. Importantly, no strategies for prevention and mitigation will becompletely successful. Thus it is recommended that all hospitals have an active shooter response plan to secure areas within the facility while maximizing the preservation of life and health of staff and patients [17].
Inadvertent firearm discharges causing injury represent another unique finding of the current study, accounting for 5.7% of hospital shootings in this series. In each instance hospital policy, or state or federal law proscribed the possession of weapons in the hospital. In the cases where hospital policy governed the presence of weapons, it was unclear whether and how these policies were communicated to persons entering the premises. Regardless, these incidents were avoidable had individuals adhered to existing laws and policies, standard magnetic resonance imaging precautions, and basic firearms safety rules.
Our findings also confirm those of a prior study investigating acute care hospital shootings from 2000–2011 [7]. Both reports describe a majority of incidents occurring inside, in large urban hospitals, and overwhelmingly perpetrated by males. Additional shared findings include more than half of shootings occurring in the emergency department and parking lot, with grudges and suicides representing the most common explanations. Moreover, in both studies, the perpetrator was most commonly a current, former, or rejected prospective intimate partner. Thus, these appear to represent targeted attacks by presumably determined shooters, which could potentially explain why the 55.6% case fatality rate among victims was higher than the 19% national firearms assault-related case fatality rate [18]. Two-thirds to three-quarters of shootings ended with perpetrators being shot, while approximately one-third of shootings ended with perpetrators committing suicide. Both investigations found similar case fatality rates for victims, 55.6% and 55.0%, respectively, and perpetrators, 70.1% and 79.0% respectively.
While eight (9.1%) shootings were triggered by an attempted escape from custody, of these five (62.5%) were initiated by the perpetrator disarming law enforcement personnel. The latter scenario was observed in 13 (8.4%) of hospital shootings reported by Kelen, et al., raising the question of whether law enforcement should disarm while responsible for individuals in custody who are also patients [7]. Those arguing in the affirmative would suggest that these shootings would have thus been avoided. Alternatively, it is not possible to determine how many escape attempts would otherwise have been successful with unarmed officers present, leading to subsequent violent crimes perpetrated by escapees. If officers are to remain armed in hospital-based assignments, our findings suggest that improved training in situational awareness and weapon retention may be advisable.
The current study offers a number of strengths. We employed methods similar to those used in a prior investigation, allowing a comparison to and confirmation of published findings. Notably, we identified a significant seasonal relationship to hospital shootings and recognized the issue of inadvertent discharges. We also appreciate several limitations. It is possible that not all hospital shootings resulting in firearms-related casualties were captured by our internet search strategies. Underascertainment could have resulted either from incidents not being reported or from reported incidents having been deleted from the internet. We believe that the impact of these two scenarios is likely to be small, considering that the shootings of interest are rare, typically considered newsworthy, and were identifiable as long as five years after occurring. The current investigation likely underestimates the broader potential risks of in-hospital firearms discharges, since we excluded facilities other than acute care hospitals and discharges not resulting in casualties. Finally, incomplete reporting precluded complete data ascertainment for some variables in a number of incidents.
In summary, approximately one in 263 (0.38%) U.S. acute care hospitals annually experiences a shooting with casualties, of which at least half occur in the emergency department, patient room, or parking lot and are perpetrated by determined shooters, resulting in higher case fatality rates than nationally observed in firearms assaults. Our study confirms earlier characterizations of U.S. acute care hospital shootings while describing a previously unreported seasonal variation to such incidents. Additionally, we identified inadvertent discharges as a previously unrecognized source of readily preventable hospital-based firearms injuries. These observations may be considered when developing comprehensive hospital workplace violence prevention and mitigation plans.
Conflict of interest
None to report.