
Abstract
BACKGROUND:
High levels of sitting are associated with increased risk of adverse health outcomes, including chronic disease. Extensive sitting at work is common, hence organisations should provide options to employees to reduce prolonged sitting.
OBJECTIVE:
To assess the efficacy and acceptability of a co-designed intervention to increase standing and reduce sitting in a public-sector office.
METHODS:
Forty-six adults participated in the quasi-experimental study (30 intervention; 16 control). The intervention involved providing sit-stand desks, prompts, workshops, and information emails to assist behavior change. Participants wore a thigh-mounted Actigraph GT3X+ for five working days and responded to an online questionnaire at baseline (BL), 6 (T1) and 13 weeks (T2) post intervention.
RESULTS:
Inclinometer-measured proportion of time standing increased in the intervention group from 14% (baseline) to 28% (T1) and 27% (T2) (67 minutes more standing over an 8-hour workday). Intervention participants reduced sitting time from 79% (BL) to 63% (T1 and T2), (80 minutes less sitting over an 8-hour workday). The control group showed no changes. The program was highly recommended (94%), and perceived to support behavior change (81%).
CONCLUSIONS:
This Move More, Sit Less intervention appears to be efficacious and acceptable. Future interventions should be co-designed to ensure culturally appropriate components and higher acceptability.
Introduction
High levels of sitting are associated with increased risk of adverse health outcomes, and sedentary behavior may be an independent risk factor for chronic disease especially amongst adults with insufficient or low physical activity levels [1, 2].
Exposure to high levels of workplace sedentary (sitting) time has become common, particularly in office environments [3]. Considering many adults spend large proportions of time at work, and there has been a steady decrease in the physicality of work tasks, workplaces have been identified as a priority setting to promote healthy behavior [4, 5]. As such, many organizations have identified a need to provide options to move more and sit less for their staff.
A range of interventions to reduce sitting have been reported, however this evidence has been generated in low generalizable samples of highly-educated, often active adults in health-related organizations and universities [6–8]. This is however, generally not the group at most risk from prolonged sitting [1]. More translational research studies are needed to examine the generalizability and acceptability of Move More, Sit Less strategies in diverse workforces and desk-based workplaces [9–12]. Moreover, workplace interventions could be strengthened by employing more participatory approaches which involve employees to co-design health initiatives, and thus, enhance engagement and ownership thereof [13]. Participatory approaches have yielded promising results in terms of increasing work-related physical activity and reducing prolonged sitting [12, 14] and further application is warranted.
Sit-stand desks have become increasingly popular in the media and the instalment of these devices is becoming more common in the workplace. Sit-stand workstations allow the user to alternate between sitting and standing postures at their desk without significant disruption to work practices or productivity [15, 16]. Previous studies have shown that the introduction of sit-stand workstations, with additional education and behavioral intervention components, can be an effective way to reduce sitting and increase standing in desk-based workers [15].
In this study we partnered with a public transport organization to co-design an intervention that was tailored to their staff, to deliver a culturally relevant program. The aim of this study was to assess the efficacy and acceptability of a co-designed multiple component Move More, Sit Less intervention in a ‘real world’ workplace setting.
Methods
Participants
Participants were employees of a public transport organization in Sydney, Australia. Eligible participants were aged 18 years and over, employed at least three days per week, and had sufficient English language proficiency to undertake study tasks. All participants were office based workers with computer based roles which included administrative functions such as emailing, making phone calls, report writing and attending internal/external meetings. The project was advertised to all staff of a division of about 200 members of staff as part of their workplace wellness program via email, and face-to-face recruitment by an internal Health & Safety professional. At the time of recruitment the workplace wellness program did not include any Move More, Sit Less initiatives; and participants continued to have full access to the workplace wellness program for the duration of the study. The University of Sydney Human Research Ethics Committee approved this study (HREC ref 2015/224) and all participants gave written informed consent.
Design
This study utilised a quasi-experimental design, with one intervention and one control group. Participants were allocated to the intervention group based on managerial consent and departmental financial provisions to provide sit-stand desks. Eligible staff members whose department was not purchasing sit-stand desks were allocated to the control group. There was allocation concealment during study recruitment and enrolment, but blinding was not possible once the study was underway due to the open plan nature of the office setting.
Data were collected during three assessment times; baseline (BL), 6 and 13 weeks after the commencement of the intervention (T1 and T2, respectively). The study took place from August to December, 2015.
Intervention
The co-design process consisted of two phases. The first phase involved a top-down process whereby managers for workplace health and safety programs (n=3) were consulted to design intervention components that would be suitable and acceptable to their organizational context. The second phase of the co-design process involved three employee information and brainstorming workshops facilitated by the research team.
The phase 1 consultation informed the design of the intervention components, which consisted of sit-stand workstations (to be provided by the organization), computer prompts reminding the participants to stand at certain intervals throughout the day, weekly informative emails with video clips, infographics and stories with Move More Sit Less strategies, regular site visits by the researchers, and a workshop that involved a short information session about the benefits of moving more and sitting less, and a researcher-facilitated session to brainstorm strategies (also phase 2 of co-design process).
Phase 2 took a bottom-up approach to co-design and in the information sessions, the researchers discussed the details of the abovementioned intervention components, along with their pros and cons, to employees assigned to the intervention condition and facilitated a brainstorming activity to examine how they could sit less and move more at work using the information provided to them as discussion triggers. Brainstorming sessions were attended by 55% of intervention group participants. At the end of the session, the final set of strategies was agreed upon and communicated back to the managers.
Researchers used content and materials produced by the Heart Foundation NSW, (https://www.heartfoundation.org.au/for-professionals/physical-activity/workplace-wellness), The BlueEarth Foundation (https://www.bluearth.org/move-sit-less/) and ASAP Science (https://www.youtube.com/watch?v=uiKg6JfS658).
Control
The control group received no change in their work practices, or work environment, nor did they receive any educational materials and apart from the data collection, they received no further attention.
Protocol
Assessments, consisting of objective monitoring, and self-report online questionnaires, took place at three assessment time points in the intervention and control conditions. Baseline (BL) measures were conducted one week prior to the intervention, T1 took place in week 6 of the intervention and T2 took place in week 13 after implementation of the intervention.
Objective measures
During all three assessments the participants wore an ActiGraph activity monitor (model GT3X+ www.theactigraph.com) on the mid anterior thigh attached with an elastic band either on top or under clothing during work hours for five working days to identify episodes of sitting, standing or stepping based on the inclination of the thigh. This device has demonstrated reliability and validity for measuring postures and activities of daily living (sitting, standing, stepping) [17]. Stepping refers to taking steps (step counts), either isolated steps or for walking, running or stair climbing. The participants were provided with an activity monitoring logbook and asked to note the time and date they wore the device each working day, the times they started and finished work and any times they took the monitor off during that period.
Self-report measures
All participants received online questionnaires, using the Survey Monkey platform (www.surveymonkey.com), at the end of each assessment (BL, T1 and T2).
Participants reported their sex, age, height, weight, department, employment status (full time or part time, and hours worked per week) and type of office arrangement (own office or open plan). Additionally, Body Mass Index (BMI) was calculated as kg.m-2.
Outcomes measured in the online questionnaire included work performance, as assessed by self-reported ratings of efficiency, overall quality and overall quantity of work on a 10-point scale measured using the Health and Work Questionnaire (HWQ) [18]. The HWQ has been reported to have overall excellent internal consistency and structural validity according to the COSMIN appraisal [19]. Internal consistency reliability values were high for all sub-scales (0.84–0.96) [20] used in this study.
Musculoskeletal pain was assessed using the Nordic Musculoskeletal Questionnaire (NMQ), [21], where participants were asked how often (Never, Seldom, Sometimes, Often, Always) they were bothered by pain in various parts of their body in the last 4 weeks. The reliability of the Nordic Musculoskeletal Questionnaire (NMQ), using a test–retest methodology, found the number of different answers ranged from 0 to 23%. Validity tested against clinical history and the NMQ found a range of 0 to 20% disagreement [21]. Comparing pain in the last 7 days and clinical examination found sensitivity ranged between 66 and 92% and specificity between 71 and 88% [22].
Physical activity was assessed though the Single item physical activity question [23] in which participants report the number of days in the last week they had engaged in 30 minutes or more of physical activity (0–7). The overall agreement between the single-item and accelerometry in classifying participants as sufficiently/insufficiently active was 58% (k = 0.23, 95% CI 0.05 to 0.41) [24]. The single-item instrument demonstrated strong test-retest reliability (r = 0.82). Concurrent validity over the past week compared to the Global Physical Activity Questionnaire was modest (r = 0.53) [23].
Process evaluation
At BL, T1 and T2, participants responded to open-ended questions in the online survey about their perceptions of the program: overall impressions, likes and dislikes about specific intervention components, intentions and expectations of the program. Additionally, at each follow-up measurement, intervention group participants responded to questions about the feasibility and sustainability of the program. Please refer to Table 1 for the exact questions asked. Workshop attendance and study completion rate were recorded and calculated.
Process evaluation questions included in the online questionnaire at the three time points BL, T1 and T2
Process evaluation questions included in the online questionnaire at the three time points BL, T1 and T2
Objective measures
We collected and processed Actigraph data using Actilife (6.13.3) and then used R (www.r-project.org) to process raw Actigraph inclinometer data to derive sitting, standing and stepping output based on hour, days and hours per day, and to analyze this data. For details, please contact the corresponding author.
The purpose of these analyses was to estimate the association between the intervention and the proportion of time spent standing, sitting or stepping at work; and the number of prolonged sitting episodes (continuous sitting for 45 minutes or more). We also explored how the proportions of standing varied through the work day.
Log book data were used to select Actigraph data corresponding to periods where the device was worn at work. Graphical displays were used to rectify inconsistencies between log-book periods and recorded data. A workday was considered valid when recorded wear time was >70% of the workday, and the workday was longer than 4 hours. If a participant had less than three valid workdays for an assessment time (BL, T1 and T2), their data for this time point were excluded.
Identifying and rectifying data inconsistencies
An Actigraph device collects data from the moment it is initialized until the data are downloaded. When the device is not being worn, data shows long periods in either standing or sitting inclinations, while when it is worn, data vary between inclinations. Periods of wear/non-wear are identified by summarizing inclination by hour, and plotting as a time series. We expected that the periods of variable inclination would align with log-book wear times. When this was not the case, we assumed there was an error in the log-book data. Participants could have omitted a period of wear from their log-book, or log a period when they did not wear the device, or get the time or date wrong. Errors could also have been introduced during manual entering of data from individual log-books, and during exchange of data (especially for dates) between software.
To identify these errors, for every participant and time point, we looked at a time series of all the data from their device, with log-book periods overlaid. These examinations were done blind to treatment allocation. If a log-book entry overlaid data that looked like the device was not worn, the rest of the time series was examined for activity periods without corresponding log-book entries. If there were no putative activity periods, the log-book entry was deleted. If there was an unlogged period of activity, the original log books were checked for data entry errors, and the period was added to the log-book. Using this method, in total 18 individual adjustments were made to the data.
The proportion of time in each inclination (standing, sitting and stepping) was analyzed using linear regression. Data were grouped into periods of sitting, or standing and stepping. We analyzed the count of periods, and the count of prolonged sitting episodes (continuous sitting for 45 minutes or more) using Poisson regression. Evidence of over-dispersion was tested by comparing Poisson and negative binomial models with likelihood ratio tests.
The unadjusted regression models included parameters for treatment (control, intervention), assessment time points (BL, T1 and T2), and their interaction. To account for the clustering of observations due to repeated measures within participant, we used robust cluster standard errors. The models were assessed for goodness of fit using quantile-quantile and residual plots. Outlying and high leverage observations were identified from residual plots and using Cook’s distance. Significance level was set at p < 0.05.
As a descriptive, exploratory analysis of changes in standing through the work day, proportion of standing per hour was plotted against work hour. A LOWESS smoother was fitted to these data to give an idea of the trend in standing proportion through the day (Fig. 3).
Self-report measures
Self-report data were analyzed with STATA IC14 (www.stata.com). For work performance and physical activity outcomes change scores were calculated between T1 and BL, and T2 and BL; these change scores were used in mixed model logistic regression analyses and sex, age, BMI, baseline, assessment time point (T1 and T2), treatment (control and intervention) and interaction between assessment time point and treatment were included as fixed factors, and participant ID was included as random factor to take repeated measures into account. Significance threshold was set at p < 0.05. Musculoskeletal pain was summarized descriptively.
Qualitative measures
The qualitative evaluation mainly focused on the participants’ perceptions and overall opinions of the Move More, Sit Less program. In addition to the participants’ views of the program, the evaluation also assessed the participants’ job satisfaction, work performance and health through open-ended survey responses, researcher observations during site visits and informal conversations with participants. The qualitative feedback collected via open-ended survey questions were independently coded by one investigator (SY) to identify recurring topics and themes. This was followed by discussion with two other investigators (LE, JYC) to reach consensus on the main themes identified.
Results
A flow diagram of participants through the study can be found in Fig. 1. Forty-six participants enrolled in the study (30 intervention, 16 control). At baseline there were 25 male and 21 female; 63% were aged between 36 and 55 years; all were working full-time and 55% were overweight or obese (Table 2). Of the intervention participants, 87% had not previously had or used a sit-stand desk. There were no significant differences for any of the demographic or weight status variables between the control and intervention groups.
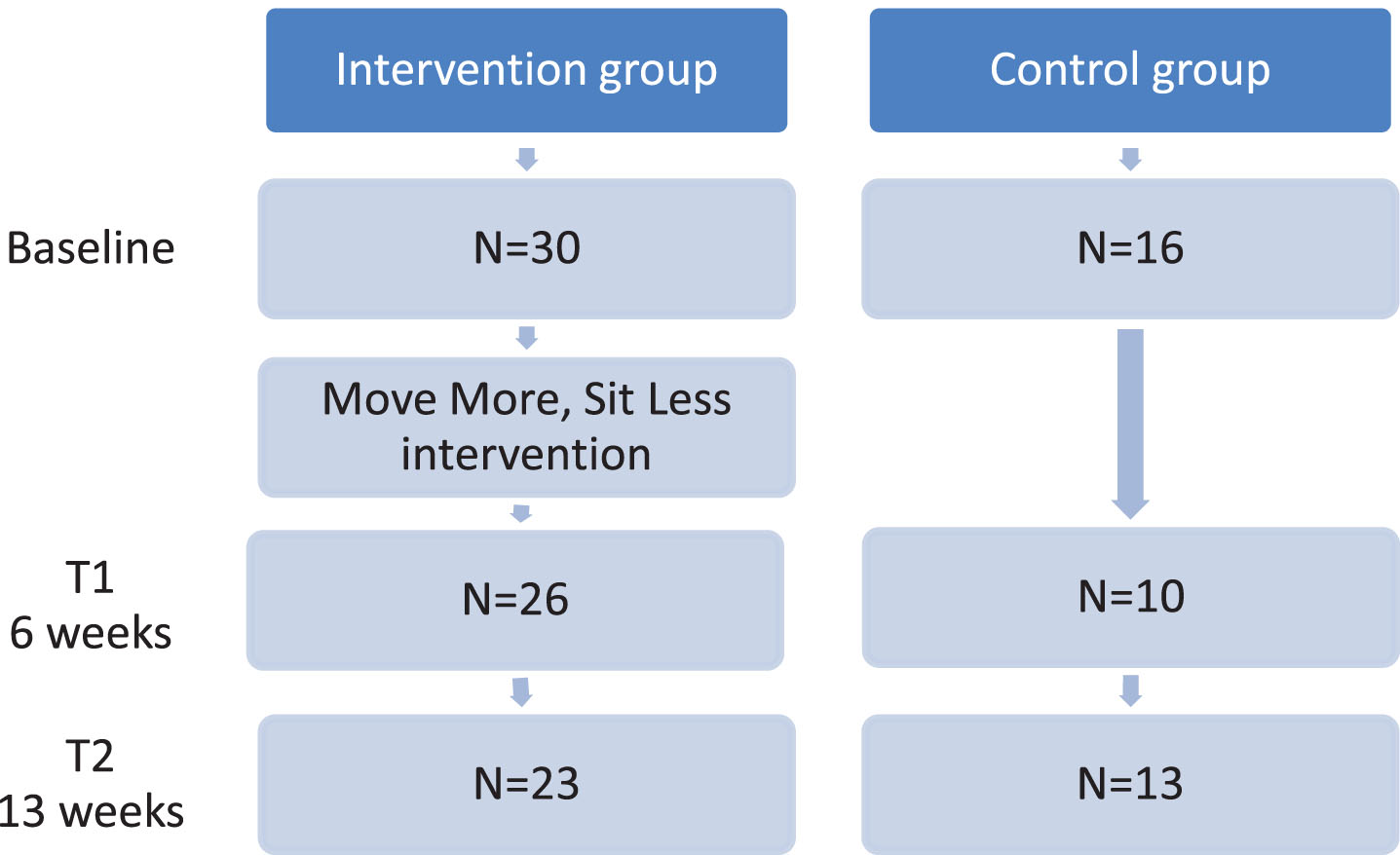
Flow diagram of study participants in the intervention and control groups.
Demographics of participants, %
Forty-one participants (27 in intervention group; 14 in control group) provided valid inclinometer data (see 3.9) and were included in the analyses. Results of analyses of the inclinometer data can be found in Table 3.
Time at work spent standing, sitting and stepping, by inclination and assessment time, including the difference between treatments at each assessment time point
Time at work spent standing, sitting and stepping, by inclination and assessment time, including the difference between treatments at each assessment time point
T1 –First follow-up (6 weeks after implementation of intervention); T2- Second follow-up (13 weeks after implementation of intervention).
Standing, sitting, and stepping proportion estimates for each time point and treatment group are presented in Fig. 2. At each time point, the null hypothesis (H0) tested is that there was no difference between the Intervention and Control groups in the proportion of time spent in an inclination. At baseline, there was no evidence against H0 for either standing, stepping, or sitting (p = 0.93) (Table 3).

Proportion of the work day spent standing (top), stepping (middle), and sitting (bottom), by treatment and assessment time point.
In the control group, proportion of workday standing remained at an average of 14% through the entire study. The intervention group showed a doubling in the proportion of their workday spent standing (14% to 28%) from BL to T1 and the effect remained similar at T2 (27%). At T1, people receiving the intervention stood, on average, an additional 15% (95% confidence interval (CI): 9%,20%, p < 0.001) of their workday compared to the control group, which equates to about 67 minutes more standing over an 8-hour workday.
The proportion of time spent sitting during work was similar for control and intervention groups at baseline (79% and 78%, respectively, p = 0.58). At T1, the proportion of sitting during the workday decreased to 63% in the intervention group only and at T2 this decrease was sustained (Fig. 2, bottom). This equates to about 80 minutes less sitting over an 8-hour workday. The proportion of sitting time in the control group remained unchanged throughout the three time points (79%, 79% and 80%, respectively).
The proportion of the workday spent stepping was significantly higher in the intervention group than in the control group at T2 (10% and 7%, p = 0.01). This equates to about 10 minutes more stepping over an 8-hour work day at T2 in the intervention group.
There was no evidence of over-dispersion, so the Poisson model was used for estimation. We found a decrease in the numbers of episodes of prolonged sitting (more than 45 minutes continuous sitting) at T1 and T2 in the intervention group. At baseline, intervention and control groups had an average of 1.75 and 2.09 episodes of sitting per work day, respectively (p-value for difference: 0.51). At T1 the intervention group had an average of 1.19 (95% CI: 0.89, 1.6) prolonged sitting episodes compared to 2.08 (95% CI: 1.65, 2.62) in the control group (p-value for difference: 0.001). At T2, the intervention group averaged 1.15 (95% CI: 0.91, 1.45) prolonged sitting episodes, compared a control group average of 2.37 (95% CI: 1.82, 3.08) (p-value for difference: <0.001).
Temporal patterns of standing
When looking at the temporal patterns across the hours of the working day (Fig. 3), it seems that the increase in standing at T1 and T2 in the intervention group is more pronounced in the earlier part of the work day, but even in the later hours standing proportion is higher than in the control group.
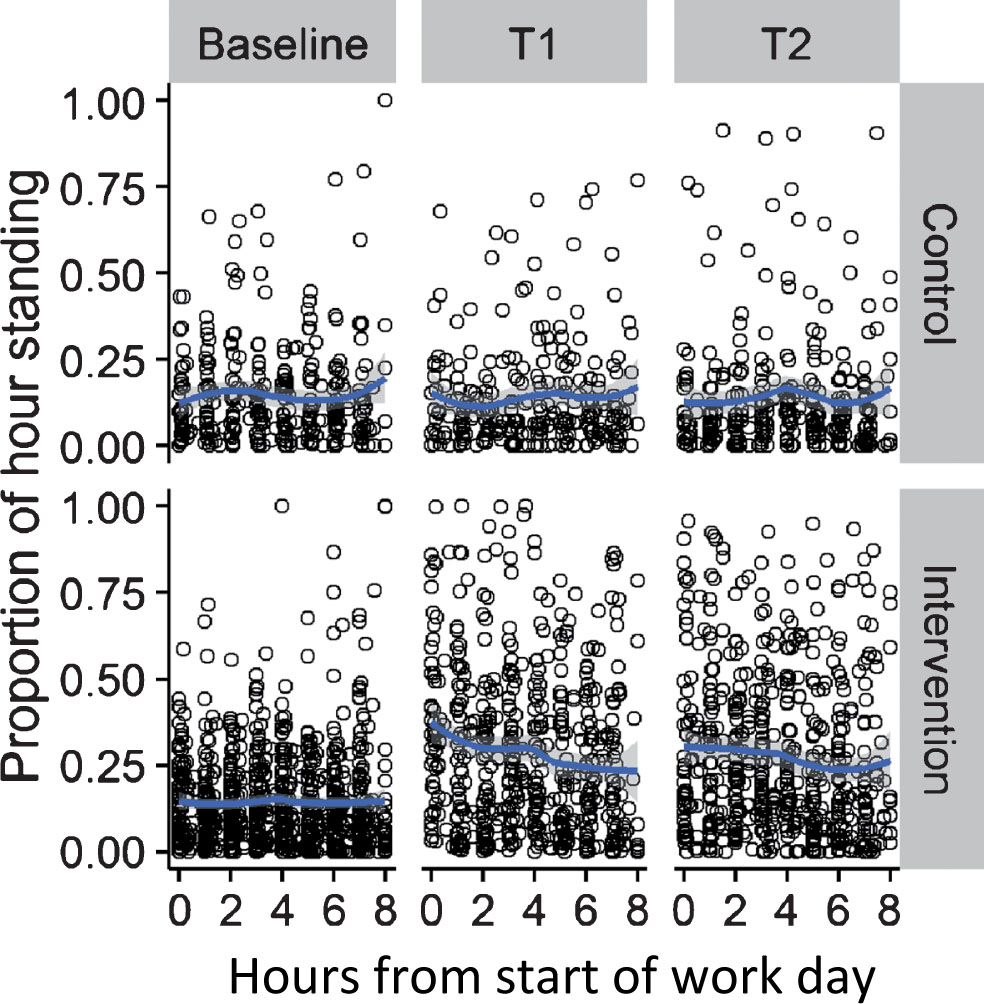
Changes in proportion of standing per hour for the first eight hours of the work day, by assessment time point (Baseline; T1; T2) and Treatment (Control, Intervention).
The results of the self-report measures on physical activity, and work performance can be found in Table 4. No significant changes were observed in the number of reported days of 30 minutes of physical activity. Although not significant, trends suggest improved work performance related outcomes, with higher ratings of looking forward to going to work every day, being able to concentrate on work, efficiency at work, and quality of work being observed in the intervention group. Importantly, there were significant interactions between assessment time point and treatment for the rating of “How well I am able to focus/concentrate”, where the participants in the intervention group increased their scores from BL to T1 and even further to T2 (6.7, 6.8, 7.7, respectively), while the control group participants’ scores decreased from 5.9 to 5.2 and 4.6, respectively, (p = 0.041, 95% CI: 0.13, 6.0). A similar effect was seen for ratings of ‘Quality of work’, which increased significantly from BL to T1 and T2 (7.5, 7.8, 8.2), respectively in the intervention group, while the ratings decreased in the control group (7.1, 7.3, 5.9, respectively. p = 0.034, 95% CI: – 4.9, –0.2).
Descriptive statistics (mean (SD)), of the self-report measures in the control and intervention groups at the three time points Baseline (BL), T1 and T2, as well as regression results (p-value and 95% CI). P < 0.05 is considered significant
Descriptive statistics (mean (SD)), of the self-report measures in the control and intervention groups at the three time points Baseline (BL), T1 and T2, as well as regression results (p-value and 95% CI). P < 0.05 is considered significant
Descriptive statistics of musculoskeletal pain at the three assessment times can be found in Table 5. Overall the proportion of participants reporting being bothered by musculoskeletal pain and discomfort “always or often” in different parts of the body was low over the course of the three assessment time points. In the intervention group, 31%, 5% and 6% reported feeling pain the neck or shoulders “always or often” at BL, T1 and T2, respectively, showing a downward trend. In the control group however, no sign of a trend was seen with, 14%, 11% and 14% reporting pain the neck or shoulders “always or often” at BL, T1 and T2, respectively. The proportion of participants reporting suffering from lower back pain “always or often” decreased (although not reaching significance) in the intervention group from BL to T1 and T2 (14%, 0% and 0%, respectively), but not in the control group.
Proportion of participants bothered by musculoskeletal pain “always or often” at baseline, T1 and T2
Thirty six of 46 participants remained in this study from baseline to second follow-up, constituting a 78% study retention rate. Complete data at all three time points was available for 38% of the participants. The workshops were attended by 20 out of 30 participants in the intervention group at baseline.
Researchers were unable to evaluate the number of participants that read the weekly information email or watched the informative YouTube videos. The post-evaluation survey revealed that 69% of respondents enjoyed the weekly emails and 37.5% ranked emails as the most useful component of the intervention. Anecdotally, researchers received feedback that participants found the emails and video links informative and useful in conveying Move More Sit Less messages in a format that was easily accessible and comprehendible.
Eighty-one percent said the program had helped them to change their sit and stand behaviour and the vast majority (80%) also thought they would keep using the strategies from the program. Almost all the respondents (94%) would recommend this program to a colleague.
Below is an overview of recurring themes related to job satisfaction, work performance and overall health. These themes were consistent throughout the three assessments.
Pre-program participant intentions and expectations
Overall, participants had high expectations of the program and had ambitious standing intentions. A handful of employees were aware of some of the health benefits of standing more and had built their own standing workstation arrangements utilising non-approved methods, however they were dissatisfied with the ergonomic limitations of these standing only workstations and were more appreciative of the variable height nature of the sit-stand desks.
Program likes and dislikes
Overall, participants’ response and attitude toward the program were very positive. The self-report survey reported that ninety-four percent of respondents would recommend this program to a colleague, indicating that the participants found the co-designed program beneficial and worthwhile.
Participants cited having variety and options as key benefits of the program. They also reported that the program helped them stand more and the intervention components reminded them to sit less. Additionally, participants reported that the program encouraged them to think about incidental activity and ways to be more active at work.
Participants cited the repetition of the online and smartphone survey as a barrier, as some participants found the task repetitive. A small number of participants reported that they experienced back strain and/or difficulty in manually raising the height adjustable desk.
Work performance and Job satisfaction
Participants in both the control and intervention groups expressed concern of restructuring as a factor that had affected job satisfaction and work performance. Other changes such as change in roles or physical desk or office location were also cited as a barrier to work performance. The themes related to job satisfaction, work performance and overall health were consistent throughout the three assessments.
Sitting and physical activity
There was a recurring theme of frustration due to the inaccessibility of stairs for use in the building. Particularly employees who work with team members across different levels mentioned they would like to use the stairs as an opportunity to increase incidental physical activity.
Discussion
This was a 13-week evaluation of a Move More, Sit Less intervention. The co-designed intervention was shown to be effective in increasing the proportion of the work day spent standing and stepping, and reducing the proportion of sitting during work. The proportion of the workday spent standing doubled from 14% to 28% and this effect was sustained at 13 weeks of the intervention. The change equates to about 67 minutes more standing per workday. The reduction in sitting was on average 80 minutes per 8-hour work day. These results are similar to previous research aiming to reduce sitting time; where a recent review found an average reduction in sitting time of 77 minutes per 8-hour workday [15].
While standing may only make small contributions to daily physical activity levels and better health outcomes, when in the standing posture, the barrier to move around, change positions and go for a short walk is likely reduced. Additionally, previous research has shown that breaking up prolonged sitting is beneficial [25]. Time substitution modelling studies demonstrate that replacing sitting for standing, light and more intense physical activity confers health benefits such as lower cardiovascular disease risk [26] and premature mortality [27]).
Although stepping only increased by 10 minutes per day in the intervention group, this could contribute to achieving the recommended weekly volume of 150 minutes of physical activity per week [28] if the stepping was of moderate to vigorous level, such as brisk walking or stair climbing. One reason for the relatively small change in stepping could be that there were few ‘natural’ opportunities to increase stepping during work time. At this workplace, the stairs between floors were not accessible, which was viewed as a barrier to movement by the participants. The distance between desks and amenities was not large, and apart from the height adjustable desks, no other changes to the physical office layout were made, hence there were no additional distances to travel to get to the printer, bin or toilet. The co-designed intervention was primarily focused on sitting less, through the provision of sit-stand desks and desktop based application prompting employees to stand at regular intervals while at their desk. The move more portion (stepping), on the other hand, was only included in the workshop and weekly emails, hence the exposure was more diluted.
In this study, the percentage reporting musculoskeletal pain ‘often or always’ seemed to decrease in 3 out of the 4 bodily areas measured, including the lower back. Although this change did not reach significance, potentially due to the small number of participants reporting musculoskeletal pain, this is convergent with previous research. Some previous studies have found a positive effect on lower back pain [29–31] and shoulder, upper and lower back pain [32], which has been explained by postural variability being linked to decreased short-term discomfort at the end of the day; while other studies including sit-stand desks have not reported these positive effects. A recent systematic review concluded that working at a sit-stand desk is likely to reduce overall bodily and lower back discomfort, compared to working at a sitting-only desk, but the small number of studies and mixed findings prevent a definitive conclusion [33]. The potential for injury trade-offs as a result of switching to sit-stand workstations from sitting-only desks also are unclear [33].
ActiGraph accelerometers have traditionally been worn on the hip to establish volume and intensity of physical activity. Whilst using cutpoints for accelerometer counts works well for identifying moderate to vigorous physical activity (MVPA), it is less accurate for distinguishing between sitting, standing, and light activity [34]. The more recent models of ActiGraph (GT3X+ and later versions), have been found to produce highly valid inclinometer data when worn on the thigh [17]. The high-resolution output can be very important; for example, by understanding the temporal patterns of posture, researchers can target interventions to times of day when they are most needed. Understanding these levels and patterns in different populations may identify at-risk groups (those with low physical activity and high sedentary time), and daily times where there is most scope to increase physical activity or reduce sedentary time. In this study there was a tendency for the intervention participants to stand more in the morning and first half of the workday, and sit more during the second half of the workday. This information can be valuable when designing customized interventions to target sitting reduction and could include more frequent prompts in the afternoon.
This study found mixed results of an intervention effect on perceptions of work performance. Intervention participants reported increased ability to focus and quality of work at both follow-ups, whereas control participants showed a reduction in these self-reported indicators of work performance. While not significant, self-report results suggest upward trends for other work performance related perceptions in the intervention group including higher ratings of looking forward to going to work every day, being able to concentrate on work, and efficiency at work. These results are consistent with previous research finding equivocal evidence about productivity impacts of sit-stand workstations [33]. For example, one sit-stand workstation study reported no changes in objective productivity indicators among customer care call centre workers [9], while another study in office staff of a health promotion unit found improved perceptions of productivity after using a sit-stand desk at work [6].
The intervention was well received by the participants and they reported that the intervention suited them well and they liked the different aspects of the intervention. The participants also reported that they had the intention to sustain the Move More Sit Less aspects during work. Future programs of this nature would benefit from identifying and promoting a divisional workplace champion, as it has been suggested that the implementation and sustainability of a program depends on champions invested and interested in the program to drive change and distribute information and enthusiasm [35, 36].
Despite the variances in work styles, management and organizational cultures in the workplace, many studies follow a standard intervention formula. Sitting research has evolved beyond the initial controlled settings of universities and health related occupations. Progress in this field of research will result from studies being conducted in real-world, diverse work places. There is therefore a need to implement and evaluate programs to determine their effectiveness in different settings, as well as to inform the resource requirements to implement, evaluate and validate tailored programs to reduce sedentary behavior. It is important to involve staff and management in program design to facilitate program implementation and adherence [7]. Taking a top-down only approach may result in the program missing the mark [10].
Strengths and limitations
This study has a number of novel concepts; the use of objective thigh-worn Actigraph inclinometer data to measure sitting, standing and stepping; the inclinometer data management and the rigorous analyses used to assess the effect of a co-designed intervention on standing and sitting in the workplace. Previously, objectively measured sedentary activity, as specified by accelerometer activity level cut-points has frequently been used as a proxy for sitting time. Methods that employ postural allocation, such as inclinometers worn on the thigh are more reliable at determining differences in occupational sitting and standing time [17, 37]. Studies using Actigraph inclinometer data to evaluate these types of interventions have, as far as we know, not previously been reported. Another strength is the worksite, which is not a health or educational setting.
Limitations include the small, single-workplace non-randomised sample, limiting the generalizability to other settings and workplaces, as well as participants being allocated to the intervention group only if they belonged to a department that had funds to purchase sit-stand desks. There was also a risk of cross-contamination between the control and intervention groups, as although the intervention and group participants were working in different departments, the office is open-plan and the research team had no control over information sharing across the groups. Although the psychometrics of the self-report measures were overall good to excellent, there is the inherent risk of potential biases, such as recall and social desirability when using self-report measures.
Conclusions
This study demonstrates a high acceptability of a co-designed Move More, Sit Less intervention in public-sector office workers receiving height adjustable desks combined with emails, workshops and site-visits. The intervention was effective in reducing objectively measured sitting time and increasing standing and stepping time and was also associated with positive perceptions of the workplace and participants’ work performance. The co-design of this pilot study was unique, and provides insights into how workplace Move More, Sit Less programs can be tailored to suit the needs of individual workplaces. Future research and workplace health interventions would benefit from a co-design to assure culturally acceptable components and a higher acceptability.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This study was funded by The National Heart Foundation NSW Division, Australia.
Thanks to participants and managers from the Partner Organization.