
Abstract
BACKGROUND:
Health professionals could be at risk of having work-related accidents or health problems. The operating room (OR) is a place where physical, ergonomic, biological, and chemical risks may be present.
OBJECTIVE:
This study aims to characterize the OR of a hospital regarding occupational risks, particularly biological and chemical. It was also sought to verify if professionals’ training about occupational risks has some influence on their safety behaviors.
METHODS:
The research method was based on a Questionnaire applied to the 214 professionals working at the operating rooms of a hospital in northern Portugal.
RESULTS:
The results revealed the occurrence of 39% (95% CI [29.3%, 50.7%]) of accidents involving biological material, and 12% (95% CI [6.1%, 21.0%]) of accidents involving chemical material. Not all professionals have had training in occupational risks (64% and 47% reported having had training in biological risks and chemical risks, respectively). A non-statistically significant association was found between having had training in biological/chemical risks and having had an accident involving biological/chemical material (Fisher’s exact test, p > 0.05). A statistically significant association (X2 = 25.978, df = 3, p < 0.05) was found between the occurrence of accidents involving biological material and the professional category.
CONCLUSIONS:
This study allows to characterize the main biological and chemical risks in operating rooms according to the perceptions of professional.
Introduction
Motivation
Healthcare workers face a wide range of occupational risks on a daily basis. Although it is possible to avoid or reduce workers’ exposure to the risks, the number of non-fatal work-related accidents and illness among healthcare workers is the highest in all industry sectors and have increased over the past decade [1]. The different professionals working in an operating room (OR) are exposed simultaneously to biological, chemical, physical, ergonomic, and psychosocial risks [2]. The risks expose OR professionals to the occurrence of serious occupational accidents with serious personal and institutional repercussions. According to van den Berg-Dijkmeijer [3], health effects on OR professionals are (allergic) skin disorders, musculoskeletal complaints, and infectious diseases. Such risks can have consequences with different levels of severity that, in the limit, can lead to the death of the professional [4]. A study about the risks in operating rooms developed in Nigeria revealed that chemical, biological, and organizational risks are not those that professionals face more often, but show a higher level of severity [5].
The operating room is, therefore a complex operational structure with a combination of several risk factors, thus defining itself as a high-risk area. Besides that, the OR is one of the most expensive workplaces in a hospital, so its optimization at different levels is a priority [6].
Objectives
The main objective of this work was to characterize the OR of a hospital regarding the occupational risks that the different professionals face, particularly biological and chemical risks. It was also sought to verify if the training that professionals have about the risks they face, has some influence on the behaviors they adopt in terms of occupational safety.
Operating rooms
Characterization of operating rooms
The OR are services of great differentiation and transversal use by the various surgical specialties. Here can be performed scheduled or urgent surgical interventions. Examinations and other procedures that require a high level of asepsis and/or anesthesia care may also be performed [7]. The operating rooms are part of the Operating Theater (OT) which is a service with great technical requirements, at the level of both the facilities and procedures and the technicians who execute those [8]. The surgical team working in OR is generally composed of one main surgeon, two assistant surgeons, one anesthesiologist, one instrumentalist nurse, one circulating nurse, and one anesthetist nurse. Physicians and/or nurses in training can also be present [7].
Occupational risks in operating rooms
The hospital professionals operate using different instruments and objects that can be dangerous. Examples are the different types of puncture-sharp materials, gases for medical use, radiation equipment, pharmaceuticals, and hygiene products, among others [9]. Other examples of occupational risks in the operating rooms are slips/trips/falls, sharp injuries, and infections due to blood exposure [10]. According to Memon et al. [11], occupational risks can include musculoskeletal disorders, psychosocial stress, radiation exposure, communicable diseases, and sharps injuries.
The occupational risks for OR nurses have been classified in the following categories [12]: accident (e.g., injuries caused by falling objects; slips, trips, and falls on wet floors; stabs and cuts from sharp objects; burns and scalds from hot sterilizing equipment; electrical shock; acute back pain resulting from awkward postures or overexertion when handling heavy patients); physical (e.g., exposure to radiation from x-ray and radioisotope sources); chemical (e.g., exposure to anesthetic drugs; skin defatting, irritation, and dermatoses; irritation of the eyes, nose, and throat; chronic poisoning; latex allergy caused by the use of latex gloves); biological (e.g., infections due to the exposure to blood, body fluids or tissue specimens; nosocomial disease as result of a prick from a syringe needle; palm and finger herpes; spontaneous miscarriages); ergonomic, psychosocial and organizational factors (e.g., fatigue and lower back pain; stress caused by the feeling of heavy responsibility; stress, strained family relations, and burnout due to shift and night work, overtime work, and contact with sick patients; problems of interpersonal relations with surgeons and other members of the operating team; post-traumatic stress syndrome caused by the exposure to severely traumatized patients or severely violent patients).
Biological and chemical risks
Accidents involving exposure to contaminated organic fluids have received special attention from occupational safety and health services. The main sources of biological risk are personal contact with patients and the handling of biological products: blood and its components, feces, urine, exudates, secretions, and vomiting, as well as materials contaminated by them [13]. The main biological agents are viruses, bacteria, parasites, fungi, and genetically modified organisms. The possible routes of entry of biological agents are respiratory, digestive, skin and mucous membranes, and the percutaneous route, which manifests itself through lesions produced by sharp and/or perforating objects, in addition to needle sticks and/or bites [14]. For most studies addressing biological accidents, the diseases of greater impact on workers’ health are caused by blood-borne pathogens such as Hepatitis B virus, Hepatitis C virus and human immunodeficiency virus [15].
According to Memon et al. [11], surgical smoke produced by the use of electrocautery or lasers systems is inevitable in modern surgery and potentially harmful to surgical professionals with long-term exposure.
The exposure to airborne aerosols and cleaning liquids can provoke eye, nose, and throat irritation [12]. Other chemical hazards in the operating room are anesthetic gases, soaps, detergents, disinfectants, and latex allergy caused by using natural latex gloves.
Physical, ergonomic and psychosocial risks
The physical risks in hospitals are represented by ionizing and non-ionizing radiation, thermal environment, lighting, noise and vibrations that can contribute to the occurrence of different occupational diseases and accidents.
Actually, the lack of ergonomics not only leads to disturbances in the workflow, but also to physical impairment and potential hazards for all persons in the OR [6]. OR professionals are considered to face several known risk factors for musculoskeletal disorders, such as long-term static postures and heavy loads. For example, nurses experienced prolonged and static postures while holding hooks, often with raised arms [16]. In a study involving surgeons working in German hospitals, most of them (95%) stood while operating. The common working posture was considered to be uncomfortable or painful by 84% of surgeons. Stress, strained family relations, and burnout, among others, are some of the possible psychosocial risks for OR professionals [12]. It is known that the presence of depressive symptoms predicts future musculoskeletal disorders but not vice versa [11].
Personal protective equipment
Personal Protective Equipment (PPE) used to protect workers from biological agents is mainly gloves, clothing, respiratory protective equipment and eye protection [17]. Gloves are a barrier to direct contact with biological and chemical agents. Facial or surgical masks do not protect against small airborne particles (aerosols). To this end, there are particulate respirators that provide different levels of protection. The plastic apron or waterproof gown should be worn to protect the gown/uniform during procedures that produce splashes or aerosols of body fluids, secretions or excretions, and should be removed as soon as the contaminating contact is terminated [13]. The gowns, uniforms and operative fields used in the OR have the function of protecting both the user and the patient against infectious agents, isolating distinct parts of the body from the contact with biological agents. From a chemical protection point of view, the purpose of protective clothing is to prevent chemicals from coming into direct contact with the skin. Regarding the protective footwear, the requirement is that it should be impermeable or should have an impermeable coverage for chemical substances, according to the European standard EN-13832-3:2006, while for biological agents there is no specific standard of footwear [18]. Relating to eye protection, splashes and aggression by gases/dust in suspension do not require special care in the choice of glasses. Interventions with high risk of blood splashes in the face oblige to the use of face masks with a visor, or to the use of masks concomitantly with goggles. The surgical cap should be placed so that it completely covers the hair and facial hair, avoiding the dispersion of particles into the atmosphere and the hair loss on the clothing or surgical fields. Uncovered hair houses microorganisms in proportion to their length, curl and oiliness [19].
Materials and methods
The present work constitutes a descriptive, analytical and cross-sectional study.
The study was conducted during the year of 2016 in a northern Portuguese hospital, more precisely in its operating theater. Ethical approval was granted by hospital administration.
The operating theater includes six operating rooms. These rooms have a direct connection with the room where the material to be used is prepared, with the anesthesia room, with the disinfection room of the surgical staff, and with the cleaning room, all being part of the restricted area of the OT. In this area, it is compulsory to use clothing appropriate to the OT (including cap and mask).
The target population of this study consisted of 214 professionals, belonging to the direct and indirect collaborators of the surgical suite of the referred hospital, namely, doctors of various surgical specialties, anesthesiologists, nurses, radiology technicians and operational assistants.
According to the previously defined objectives, a questionnaire was used to collect the necessary information. The data collection method used was a questionnaire, given this is an efficient method for collecting a large volume of information in short periods of time [20]. The questionnaire was developed based on another one used in a similar work, by Perdigoto [4]. However, some issues have been redefined and others have been deleted in order to meet the stated objectives. This adaptation resulted in a questionnaire consisting of four sections. Section 1 consists of questions aiming at characterizing the sample: professional category, demographic data, whether professional had specific training in biological, chemical, ergonomic, and physical risks, as well as prophylaxis of hepatitis B. This section ends with a question about whether the usual activity causes anxiety or stress to the professional. Section 2 contains a single question related to the occurrence of occupational accidents involving biological materials. However, this question is subdivided into several sub-sections which address, for example, the level at which the exposure occurred (e.g. mucosa, percutaneous, other), the object and the biological material involved, as well as the activity that the professional was carrying out at the moment, the use of personal protective equipment (PPE), and the behaviors taken after the accident. Section 3 has a question related to the occurrence of occupational accidents with chemical materials. Like the previous question, this also is divided into several sub-sections similar to the described for the previous question. Lastly, the fourth section of the questionnaire consists of a single question relating to the number of working days lost due to the last accident, involving biological/chemical material.
The questionnaire was pre-tested with ten professionals selected by convenience. After this, the questionnaire was able to be applied to all elements of the study population, allowing the collection of various types of information, namely on the occurrence of accidents with biological and chemical materials, information on the main risk factors for such accidents, and also on its consequences. The questionnaires were given to the representatives of the different groups of professionals to make them reach their collaborators, appealing to them to collaborate in the fulfillment of the questionnaires, with the certainty that moral and ethical issues were safeguarded, namely the anonymity of the subjects, and confidentiality of the data.
The data collected was firstly organized in an Excel database. The statistical analysis of these data was performed using the statistical software IBM® SPSS® Statistics, version 25.0.
The statistical procedures were chosen according to the nature of the variables involved. Fisher, t-Student, and Chi-square statistical tests were applied. The decision rule used was to detect significant statistical evidence for probability values (p-value) less than 0.05 (p < 0.05).
Results
The results are divided into two subsections: descriptive statistics concerning the summary statistics and characterization of the participants in the questionnaire; statistical tests to evaluate comparisons and/or associations between variables.
Descriptive statistics
The total number of respondents was 86 professionals from a total of 214, representing 40% of the target population. Half of the participants were nurses (n = 43, 50%), followed by surgeons and anesthesiologists (n = 19, 22%, for both), and by operational assistants (n = 5, 6%). Most of the participants were females (n = 58, 72%).
The majority of the professionals had no training on chemical and physical risks (53% for both types of risk), unlike, most of the professionals had training in biological and ergonomic risks (64% and 55%, respectively). The distribution of respondents according to having had training on the different occupational risks is illustrated in Fig. 1.
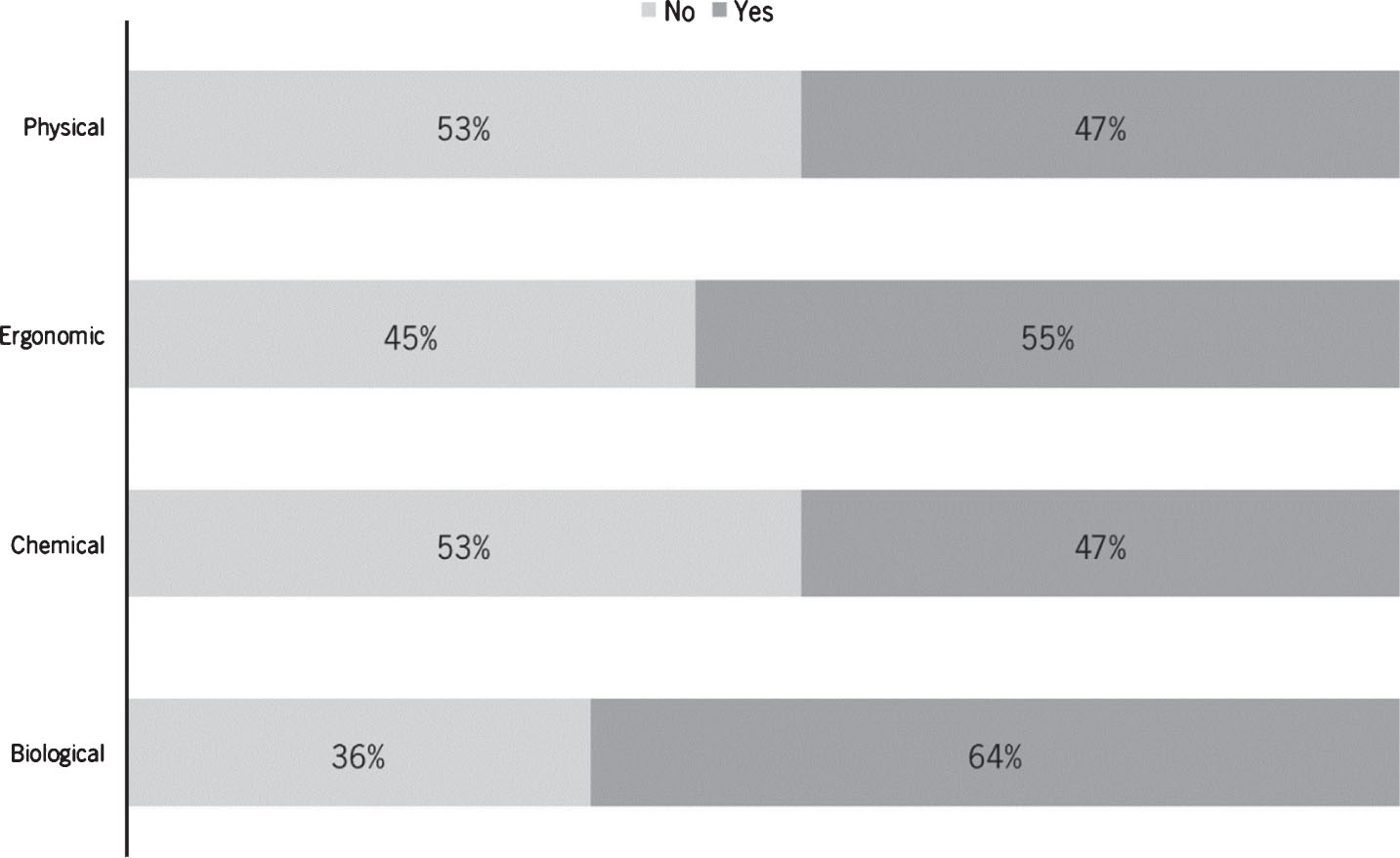
Distribution of respondents in what concerns “have had training on the different occupational risks”.
In relation to the time elapsed since the training in biological risks, professionals report having done it, on average, 61 months ago, with a standard deviation of 58 months (minimum - 12 months, maximum - 336 months). Training on chemical risks had been done on average 59 months ago, with a standard deviation of 59 months (minimum - 6 months; maximum - 336 months).
It was found that most participants were vaccinated against hepatitis B (89%).
The answers to the questions “have you had an accident with biological material in the OR?” and “have you had an accident with chemical material in the OR?” were as follows: 39% reported having had at least one biological accident and 12% reported having had at least one chemical accident (Fig. 2).

Distribution of respondents according to has had occupational accidents involving biological or chemical material.
It was found that accidents involving biological material were more common than accidents with chemical material.
Information about the context in which the accident occurred
Concerning the level at which exposure to biological material occurred, according to Table 2, it is observed that the majority of professionals reported the percutaneous level (n = 27, 84%), followed by the mucosa (n = 4, 13%).
Information about the level at which the accident occurred
In relation to the object involved in the accident, most of the participants reported the needle (n = 24, 75%), and a smaller percentage reported the scalpel blade (n = 4, 13%). The remains 13% referred “other”. The answers to the question “what were you doing when the accident occurred?” can be seen in Table 3. The majority reported that they were operating (n = 11, 36%).
Information about what was the professional’s activity when the accident occurred
Figure 3 shows the professionals’ responses regarding the PPE that they were using when the accident occurred. The most frequent were: surgical cap, mask, and surgical gloves.

Answers concerning the PPE they were using when the accident occurred.
Regarding the behaviors adopted by professionals after accidents with biological material, the most frequently adopted procedures were: make local antisepsis (82%), to identify the patient, source of the problem (39%); perform medical examinations (32%); wash with soap and water (32%); perform exams to the patient (29%). Only 3% reported having done nothing.

Distribution of the main effects due to chemical accidents.
Figure 5 shows the professionals’ responses regarding the PPE they were using when the chemical accident occurred. Closed shoes (80%), the mask (80%) and the surgical cap (60%) were the most frequent PPE.
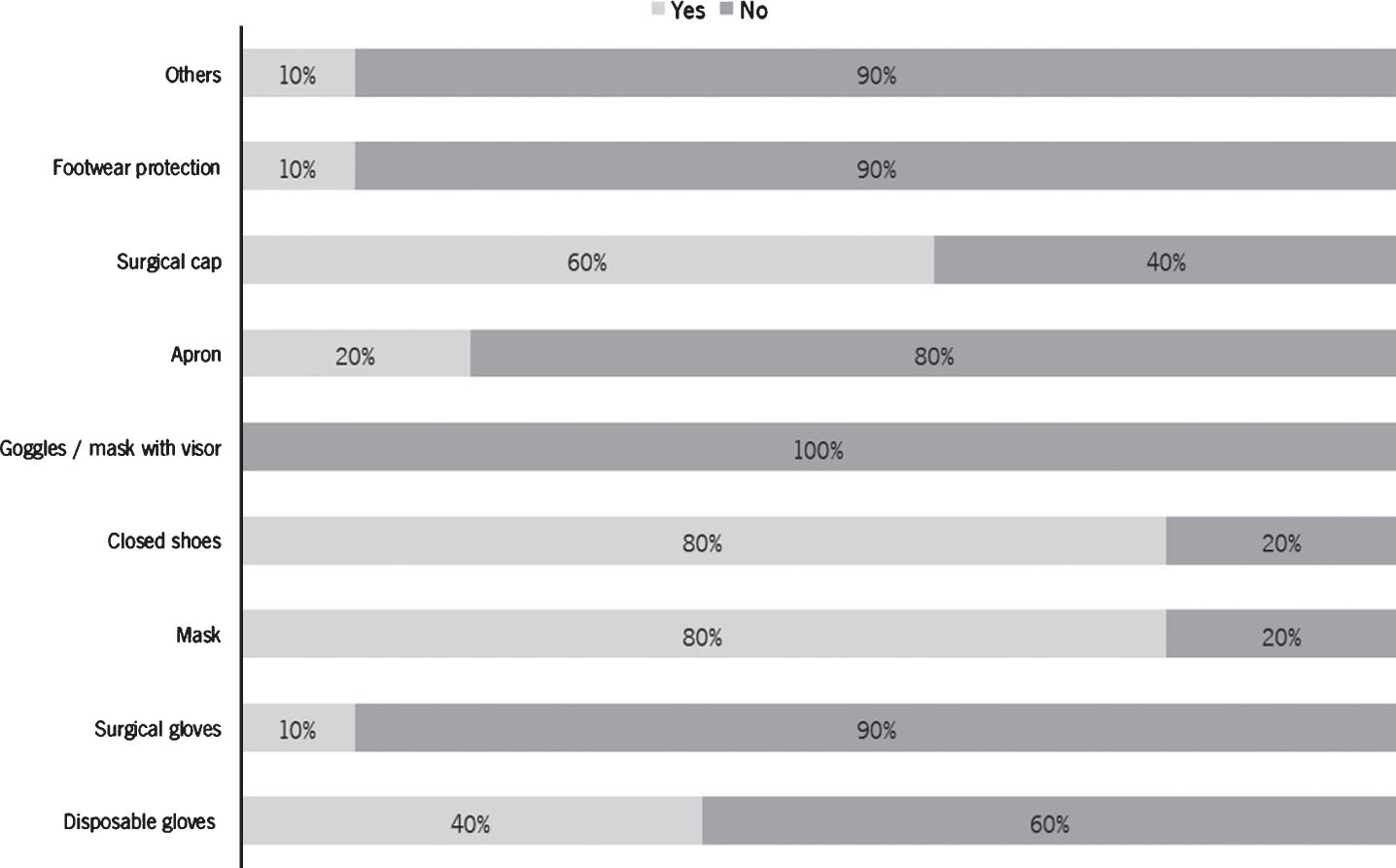
Distribution of respondents in what concerns the PPE they were using when the chemical accident occurred.
Regarding the behaviors adopted by professionals after the accidents with chemical material, the most frequently adopted were: to identify the product that caused the problem (50%); wash with running water (50%); do nothing (30%); leave the place (20%). No one reported having performed medical examinations or washed with soap and water.
Only two situations revealed a statistically significant association between variables. One of them was training in biological hazards/wash hands with soap and water after an accident with biological material, and the other was the professional category of surgeon/occurrence of accident involving biological material. Table 4 resumes the results achieved.
Summary of the statistical tests applied
Summary of the statistical tests applied
†The behavior that revealed association was washing hands with soap and water; *Significant at 5%; df: degrees of freedom.
In this study, it was found that participants reported having more accidents involving biological material (39%) than accidents involving chemicals (12%).
The fact that about 11% of respondents are not vaccinated against hepatitis B is worrisome given that according to some authors [21, 22] vaccination is the main strategy to prevent the labor transmission of hepatitis B virus. In addition, antibody levels decrease over time, which leads us to conclude that even professionals who have been vaccinated may not currently be protected from hepatitis B virus being, in this case, necessary to administer them a booster vaccine [22].
The average time elapsed since professionals had training, in both biological and chemical risks, was about 5 years. There was no statistically significant association between has had training and the occurrence of biological or chemical accidents, nor with the use of PPE. The statistically significant association detected between the professional category of surgeon and occurrence of accident involving biological material is according to Perdigoto [4] that points out surgeons as the professionals’ group suffering more accidents in the OR.
It was found that the occurrence of accidents (biological and chemical) is not dependent on factors such as seniority or age. This is in line with the study by Kasatpibal et al. [9] which covered more than 2000 operating room nurses, in which age was not identified as a risk factor for accidents. There was a statistically significant association between has had training in biological risks and certain behaviors adopted after an accident with biological material, namely washing with soap and water.
Most of the accidents occurred in the surgical context and at the percutaneous level (84%). The needle was the object most involved (75%), and blood was the biological material most often implicated (94%). Such results are in agreement with other studies that, generally, see a greater risk in the piercing-sharps objects, which are manifested mainly by the skin and mucous membranes [14, 23]. Although professionals understand the importance of using the appropriate PPE to their work, there have been gaps in the use of PPE, namely protection of footwear, apron, glasses or mask and even gloves. Not wearing PPE is a potential risk factor for biological accidents [9]. According to a study developed by Nagao et al. [24], there is poor awareness of protective equipment (double gloving, face shield/ goggles).
It is relevant to mention that the information collected from the respondents may have been impaired by their memory since some of them verified that they no longer remembered all the required data.
The results of this study highlight that much remains to be done with regard to occupational safety and health of OR professionals. Especially in what concerns to the awareness that everyone should be protected against hepatitis B virus and the importance of using the appropriate PPE in each situation. Insisting on more frequent training of these professionals about occupational risks and good practices can contribute to this awareness.
Conclusions
This study allowed us to characterize the main biological and chemical risks in the OR of a hospital, according to the perceptions of its professionals. It was also intended to understand if the training that professionals had in biological and chemical risks has influence on their work behaviors, in terms of safety. The analysis of the results allowed to verify that in the OR the accidents of biological nature are more expressive, can have serious consequences. It was found a statistically significant association between “training in biological risks” and “wash hands with soap and water after an accident with biological material”, and between “professional category of surgeon” and “occurrence of accident involving biological material”. Although vaccination is not legally enforced, it is recommended that strategies be defined so that all OT collaborators can benefit from the vaccination schedule and consequent immunity to the hepatitis B virus. It is important to encourage the correct and appropriate use of PPE in the workplace, which could prevent and protect individuals from accidental occurrences. It is suggested that health professionals and the Institution itself be more involved in risk prevention and, mainly, in promoting a safe working environment.
A more exhaustive, in situ, characterization centered on the type of risk, is suggested so that more specific and frequent training programs can be designed and developed, constituting a more effective preventive measure for the reduction of occupational accidents in the OR.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This work has been supported by FCT – Fundação para a Ciência e Tecnologia within the Project Scope: UID/CEC/00319/2019.