
Abstract
BACKGROUND:
Many ophthalmic lens manufacturers are currently marketing blue-blocking filters, which they claim will reduce symptoms of Digital Eye Strain (DES). However, there is limited evidence to support the proposal that DES results from the blue light emitted by electronic screens.
OBJECTIVE:
This investigation compared the effect of blue-blocking filters on DES symptoms with a no-filter lens, using a double-blind methodology.
METHODS:
Twenty-four subjects were required to perform a 20-minute reading task from a tablet computer. They wore either lenses containing a blue-blocking filter (TheraBlue 1.67 or TheraBlue polycarbonate) or a CR-39 control lens which did not include a filter. Immediately following each session, subjects completed a questionnaire to quantify symptoms of DES.
RESULTS:
While a significant increase in symptoms was observed immediately following the near vision task (p = 0.00001), no significant difference in symptoms was found between the 3 lens conditions (p = 0.74).
CONCLUSIONS:
There is little evidence at this time to support the use of blue-blocking filters as a clinical treatment for DES. Management of other ocular factors, as well as the creation of an optimal environment for screen viewing, are more likely to provide greater success in minimizing symptoms.
Introduction
We currently live in a society where electronic devices are deeply embedded into daily life. 90% of families in the United States own at least one computer (such as a smartphone, desktop, laptop or tablet computer), while the typical (median) American family has 5 or more of these devices [1]. Additionally, screens are used widely in the workplace, at school and in the case of portable devices, anywhere. Therefore, it is critical to understand why between 40 and 60% of individuals experience visual and/or ocular symptoms while viewing electronic displays for a prolonged period of time [2, 3]. These symptoms may include tired eyes, ocular irritation, burning, eye strain, redness, dryness, blurred or double vision, and are collectively termed Digital Eye Strain (DES) [4]. Although the symptoms are typically transient and disappear soon after computer operation ceases, some individuals do experience ocular discomfort for a sustained period after prolonged viewing of a digital screen.
Recently, attention has been drawn to the potentially damaging effect of blue light being emitted from electronic displays [5–7]. Indeed, blue light contributes more than one-third of the emission spectrum of an Apple iPhone 7 (Apple Inc., Cupertino, CA) [8]. However, this output is many times smaller than the magnitude of blue light being emitted by the sun, which has an average daylight luminance around 100,000 lux [9, 10].
Blue light plays an important role in normal human physiology, being responsible for regulation of the circadian rhythm and sleep cycle [11]. In addition, short-wavelength radiation enhances attention, mood, and performance [12]. However, short wavelength, visible light can be harmful to the eye. For example, blue light may be responsible for the phototoxicity of light sensitive cells in the retina [13, 14]. Furthermore, increased exposure to the short wavelength spectrum has previously been associated with the development of age-related macular degeneration, and may damage the retinal pigment epithelium cells within the posterior segment of the eye [15, 16]. Certain groups may be particularly susceptible to blue light damage, such as children (because of the transparency of their crystalline lens) and those individuals whose natural crystalline lens has been removed (typically following cataract extraction). With increasing age (especially in individuals over 50 years old), the crystalline lens gains a yellow or brownish tint, which reduces the transmission of blue light to the retina [17].
While it has been proposed that DES may be caused by prolonged exposure to the blue light emitted from digital screens, the evidence to support such a claim is minimal. Nevertheless, many ophthalmic lens manufacturers market blue-blocking filters as a treatment paradigm for DES. In one test of their efficacy, Cheng et al. [18] examined the effect of low-, medium-, and high-density blue filters (in the form of wraparound goggles) worn during computer work in groups of dry eye and normal subjects. Unfortunately, the transmission characteristics of the 3 filters was not provided. The authors observed a significant reduction in symptoms in the dry eye group, but not in the non-dry eye subjects. This significant effect was seen for all filter densities. However, the study did not include a control condition, and so a placebo effect, whereby the subjects were aware that they were receiving treatment, cannot be ruled out. Further, the wraparound goggles may have reduced tear evaporation in the dry eye subjects, thus increasing ocular comfort.
Subsequently, Lin et al. [19] evaluated the effect of blue-blocking lenses on both symptoms of DES and critical fusion frequency (i.e., the rate of alternation above which the observer is unable to detect that a stimulus is flickering [20]) following a 2-hour computer task. Critical fusion frequency has previously been associated with eye fatigue [21, 22], although as yet, no underlying mechanism has been elucidated linking them. During the trial period, subjects were required either to “view videos or engage in games”. Unfortunately, no specific details of the task, such as viewing distance, cognitive demand or the duration spent on each of the two assignments, i.e., passive viewing versus performing a more active task were described. The authors determined that the “high blocking filter”, which blocked around 60% of the blue light, produced a significantly higher post-task change in critical fusion frequency, when compared with either a low blocking blue filter (which blocked approximately 24%) or control lenses that blocked approximately 3.2% of blue light. Indeed, based on the critical fusion frequency findings, the authors reported that subjects wearing high blocking filters had less fatigue after the 2-hour task than before they started the trial. With regard to reports of subjective symptoms, the high-blocking filters produced a significant reduction in 3 specific symptoms, namely pain, heaviness and itchy eyes, but not in other previously noted DES symptoms such as tired eyes [3]. An additional concern with this study was that the various filter conditions were performed on different groups of subjects, and so the reduced symptoms observed in the high blocking filter group may have been a consequence of those particular individuals, rather than being due to the effect of the filters. Accordingly, the aim of the present investigation was to compare the effect of blue-blocking filters on DES symptoms with a no-filter lens using a double-blind methodology.
Methods
The experiment was carried out on 24 subjects (5 male, 19 female) between 16 and 17 years of age (mean age = 16.1 years; SD = 0.50 years). All were students at Midwood High School, Brooklyn, NY. Using data from a previous study [24], the estimated effect size divided by the standard deviation of the effect gave a value of 1.76. Taking α and β values of 0.05 (2-tailed) and 0.1, respectively, this indicated a sample size of 21 subjects [25]. Accordingly, the sample of 24 subjects used here should be adequate.
All subjects had best corrected visual acuity of at least 20/20 in each eye either unaided, or with their habitual contact lens correction. Because of the need to wear the experimental glasses, subjects could not wear a spectacle refractive correction during the study. None had strabismus or manifest ocular disease. The study followed the tenets of the Declaration of Helsinki. Since all of the subjects were under 18 years of age, informed written consent was obtained from the parent or legal guardian after an explanation of the nature and possible consequences of the study, with informed assent being obtained from the subjects. The protocol was approved by the Institutional Review Board at the SUNY State College of Optometry.
Prior to each session, subjects viewed a distant visual acuity chart at a distance of 5m for a continuous 5-minute period to minimize the effect of any previous near-visual activities [26, 27]. After this period of distance fixation, they performed a cognitively-demanding reading task for a 20-minute period. Subjects were required to read material aloud (to ensure compliance) from a tablet computer (Apple iPad Mini –model A1432: Apple Inc, Cupertino, CA) at a viewing distance of 33cm. This is a common reading distance for handheld devices [28, 29]. The computer was supported on a reading stand to maintain a constant gaze angle of approximately 40° downgaze. The reading material comprised paragraphs of unrelated words produced by copying the first and last word of each line from a number of fiction novels. Subjects were allowed to scroll through the text as required. The computer text was displayed using Microsoft Word software (Microsoft Inc., Redmond, WA, USA). The text was single spaced, black, Times New Roman font of approximately 90% contrast. The vertical height of a lower case letter without ascenders or descenders was approximately 1 mm (equivalent to 0.7M [30]). This reading task has been used in previously published studies from our laboratory, and shown to be sufficiently demanding to produce symptoms after relatively short tasks [31, 32].
Before, and immediately after the reading task, subjects were asked to complete a questionnaire regarding symptoms experienced during the reading task [33]. This questionnaire has been used in previous studies, and shown to be repeatable [24], with a repeatability coefficient [34, 35] of 13.46. This latter number indicates the value below which the absolute differences between two measurements would lie with 0.95 probability [36]. Post-task symptoms were reported on a scale from 0 (none) to 10 (very severe), with a score of five representing a moderate response. The total symptom score was quantified on a scale from 0 to 100. The questions are shown in Table 1.
Questionnaire administered to subjects immediately following the reading task. The questionnaire is taken from Hayes et al. [33]
Questionnaire administered to subjects immediately following the reading task. The questionnaire is taken from Hayes et al. [33]
Did you experience any of the following symptoms either during or immediately after the task? If no, please circle zero for each question. If yes, please rate the intensity of the symptom on a scale from 1 (very mild) to 10 (very severe), with 5 being a moderate response.
Subjects were required to attend for 3 sessions, with the trials being separated by a period of at least 24 hours. During each session, subjects wore one of 3 pairs of plano powered spectacles, each of which was mounted in an identical frame. All of the lenses incorporated an anti-reflection coating to minimize reflections from the anterior surface of the lens, as well as to equate the appearance of the 3 pairs of spectacles. The lenses were made from the following materials; (i) TheraBlue 1.67, (ii) TheraBlue polycarbonate and (iii) CR-39 [35]. The two TheraBlue materials (Luzerne Optical Laboratories Ltd., Wilkes-Barre, PA) are clear lenses which include blue-blocking filters. The manufacturer’s website (www.luzerneoptical.com/therablue-uv-hev-lenses.html) claims that the TheraBlue 1.67 lens blocks 98% of 415 nm, 41% of 430nm and 11% of 450 nm visible radiation, while the TheraBlue polycarbonate lens blocks 57% of 415 nm, 15% of 430 nm and 10% of 450 nm visible radiation. CR-39 is a widely-used, clear plastic lens material which transmits over 90% of wavelengths in the blue range (400–500 nm) [37]. This served as the control condition. Since all 3 pairs of glasses had an almost identical appearance, the blue-blocking material was not readily identifiable to either the experimenter (RTL) or the subjects. The order of the 3 trials was counterbalanced across subjects.
All data was saved onto a Microsoft Excel spreadsheet (Microsoft Inc., Redmond, WA, USA), and statistical testing (analysis of variance) was performed using this same software. A p-value<0.05 was taken as the criterion for statistical significance.
Mean pre- and post-task symptom scores are shown in Table 2. One-factor analysis of variance indicated no significant difference between the pre-task scores for the 3 testing conditions (F = 0.15; df = 2,71; p = 0.86). Two-factor (pre- versus post-task, testing condition) analysis of variance indicated that the task produced a significant change in symptoms (F = 20.59; df = 1,143; p = 0.00001), whereas the effect of the different lenses was not significant (F = 0.74; df = 2,143; p = 0.74). The mean change in symptoms following the sustained reading task (with respect to the pre-task value) is shown in Fig. 1.
Mean pre- and post-task symptom scores for the three lens conditions. Figures in parentheses indicate 1 standard error of the mean (SEM)
Mean pre- and post-task symptom scores for the three lens conditions. Figures in parentheses indicate 1 standard error of the mean (SEM)
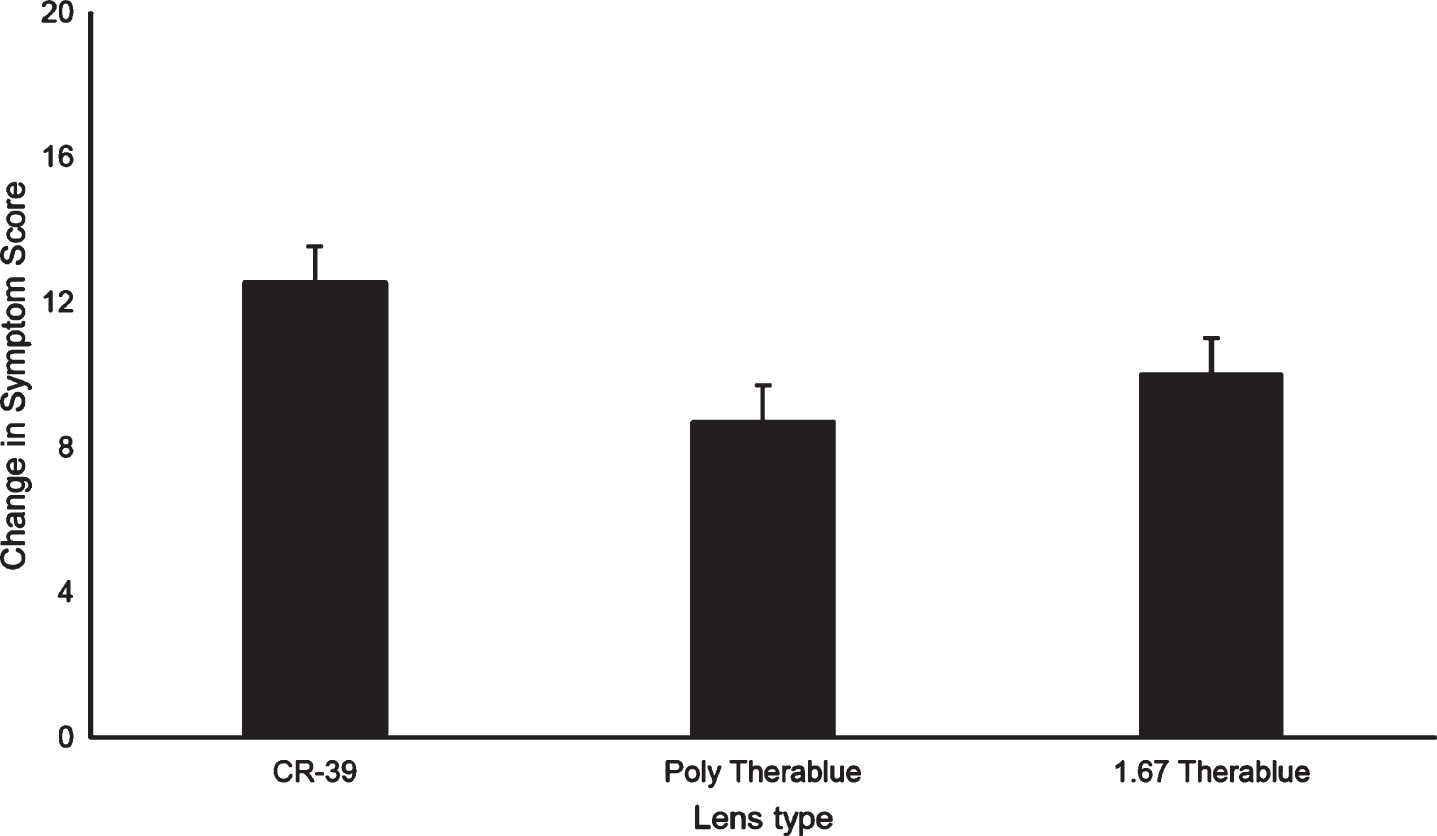
Mean post-task change in symptom score following a 20-minute reading task from a tablet computer for the 3 lens conditions. Error bars indicate 1 standard error of the mean (SEM).
The results of the present investigation are consistent with the findings of Palavets and Rosenfield [23], namely that blue-blocking filters do not produce a significant reduction in DES symptoms. It should be noted that the filter used in the previous investigation was bright yellow and blocked 99% of blue light, which is markedly different from most current, commercially-available filters. The TheraBlue filters used here were more typical, appearing clear (and therefore indistinguishable from the CR-39 control lenses), while only blocking around 10% of the mid-blue range (around 450 nm).
Additionally, there is no clear physiological mechanism linking blue light with symptoms of eye strain. Wavelengths around 470 nm inhibit the production of melatonin, a hormone which regulates the body’s circadian rhythm, and so blue light exposure in the evening may interfere with the ability to go to sleep. It is for this reason that digital screen time should be avoided in the 1-2 hours before bedtime [38]. Further, extremely high levels of blue exposure may be associated with damage to the posterior segment of the eye [5–7], and have been linked with conditions such as age-related macular degeneration [39]. However, with regard to DES, Lawrenson et al. [40] concluded that there is currently “a lack of high quality evidence” to support using blue-blocking filters to improve visual performance or alleviate eye fatigue. Simply because digital screens emit larger percentages of blue light, and the observation of a high rate of symptoms with these electronic devices, does not prove causation. In considering the visual symptoms that arise from fluorescent lighting, Wilkins and Wilkinson [41] noted that a tint which removed short wavelengths would reduce the modulation of the lamp. They cited 4 cases where a tint that removed 90% of light between 400 and 500 nm produced increased comfort, but all these cases related to conditions other than DES, namely visual discomfort, agoraphobia, photosensitive epilepsy and post-traumatic light sensitivity. Interestingly, Viola et al. [42] reported that the use of blue-enriched, white fluorescent lighting (17,000K) in an office setting produced improved alertness, positive mood, ability to concentrate, ability to think clearly and decreased evening fatigue, when compared with white fluorescent lighting (4,000K).
Limitations of the present study include the relatively short task duration (20 minutes), and that only a single test distance and gaze angle were adopted. Nevertheless, the task demands were sufficient to produce a significant change in symptoms. It would also be valuable to determine an objective measurement of DES, rather than using a subjective questionnaire, but current work from our laboratory does not support the proposal that changes in critical fusion frequency can be used as an objective measure of eyestrain or other symptoms of DES [43]. Additionally, the reported symptom symptoms may have been affected by activities conducted before the start of the experimental session. While a 5-minute “wash-out” period was allowed before the start of each trial, it is possible that this was not long enough to remove all the effects of earlier visual tasks.
It appears likely that DES results from issues such as the environmental conditions and ergonomics, or the demands placed on ocular accommodation and vergence to create a clear and single image of the electronic display. Sheedy et al. categorized DES symptoms as either being external, such as ocular burning, irritation, dryness and tearing, or internal, including eyestrain, headache, eye ache, diplopia and blur. External symptoms were produced by problems with the anterior ocular surface and tear layer, whereas internal symptoms were caused by refractive, accommodative or vergence anomalies [44]. These authors proposed that the underlying problem could be identified by the location and/or description of the presenting symptoms.
In summary, it remains unclear why blue wavelengths should produce symptoms during the sustained viewing of a digital screen positioned at a near viewing distance. Furthermore, there is no current direct evidence to support the use of blue-blocking filters as a treatment for DES. Individuals suffering from these symptoms should receive a complete ocular evaluation, including refractive error, binocular vision, oculomotor and ocular surface assessments to determine the health of the eye. In addition, they should be counselled regarding appropriate ergonomics and environmental issues when viewing electronic devices for a sustained period of time. Factors such as appropriate viewing distances and gaze angles, the need for frequent breaks and avoidance of glare and screen reflections should also be emphasized.
Conflict of interest
None of the authors has a financial interest in any of the products tested in this study.