
Abstract
BACKGROUND:
The incidence of stroke is growing in various parts of the world and the condition most commonly affects the adult population.
OBJECTIVES:
The purpose of the study is to provide a narrative review of papers published in the last 11 years in English and in Polish and focusing on demographic characteristics of individuals returning to work after stroke, return to work rates, length of time post stroke to return to work as well as health conditions, or personal and environmental factors associated with return to work after stroke. The study also presents the situation regarding return to work after stroke in Poland in comparison to other countries.
METHODS:
The narrative review covers Polish and foreign literature published between 2007 and 2018. The number of records initially identified through English databases search amounted to 4,912. Five records were additionally identified through other sources (Polish databases). Ultimately 26 (21 foreign, 5 Polish) refereed publications were selected to be reviewed in this study, based on their relevance in terms of specific inclusion/exclusion criteria.
RESULTS:
The appraisal of Polish and English-language literature shows that stroke survivors’ ability to return to work varies; in our country the rate being 43% and outside of Poland reaching the rate of 74.7%. Average time frames for return to work for stroke survivors include from 3 to 6 months, from 12 to 18 months and up to 3 years post stroke. One of the most frequently reported positive factors in the English-language literature is individually tailored vocational rehabilitation. There is a scarcity of studies related to return to work after stroke in Poland.
CONCLUSIONS:
The findings from studies included in this narrative review may suggest a need to improve the situation in Poland with regard to measures related to return to work after stroke, including vocational rehabilitation which is insufficiently available in Poland.
Introduction
Stroke is one of the most frequent and the most serious consequences of cardiovascular diseases affecting the public, and it is the main cause of disability [1]. It is recognized that stroke occurs commonly both in developed and in developing countries [2]. In spite of the considerable progress in primary prevention, diagnostic procedures and treatment systems, stroke is the second or third most common cause of death, and projections suggest the situation will not change by 2020 [3]. The incidence of stroke is growing in different parts of the world and the condition most commonly affects the working-age population – one in four patients is less than 60 years old [4, 5]. Clinical outcomes, in particular neuropsychological consequences, may adversely affect patients’ ability to resume employment, and have a major impact on the patients, their families and their health-related spending [5]. Failure to return to work after stroke leads to negative consequences for the person affected by the condition as well as for society, as it is associated with additional economic burden [4, 5]. For example, it has been estimated that the total economic cost of stroke affecting Great Britain exceeds £8.9 billion per year, and a significant part of these costs is related to loss of employment and payment of benefits (£2.2 billion) [6]. On the other hand, in Sweden, work absences, earlier retirement, and years of work (productivity) lost due to stroke-related deaths accounted for 21% of the total cost of stroke [7]. In the USA, the direct medical cost of stroke amounts to 18.8 billion USD annually, and the estimated per-capita cost of post-stroke care totals $7,657.60 [8]. According to recent reports, the indirect costs of ischemic stroke together with work absences, in the USA amounted to 1.384 billion dollars; this will account for 53% of the total ischemic stroke related costs between 2005–2050. It has also been pointed out that the indirect costs will continue to increase, particularly in the case of the African-American and Hispanic populations, due to the growing wages of these two groups in the US population [9, 10]. In Poland, the total cost of treatment administered to one patient with stroke amounts to approximately 60,000 PLN [11]. According to a 2013 report published by the Institute of Healthcare Organization, stroke related costs in Poland include over 1,000,000 days of sick leave, an expenditure of 704,050,000 PLN related to treatment and rehabilitation, and an expenditure of 679,000,000 PLN related to rehabilitation benefits, pensions, and costs of sick leave [12].
In addition to its economic importance, work is associated with benefits of critical importance for an individual’s health and well-being. An important source of income, work is also necessary for active involvement in society and for satisfying essential psychosocial needs; it helps develop and maintain one’s identity and social status [6]. High unemployment rates in a country are associated with a higher mortality rate, poorer mental and physical condition of the population, and greater use of health-care resources [6, 13]. Research has suggested that work is beneficial for health and that lack of work may be a risk factor for stroke [14, 15]. Return to work is of great importance for stroke survivors, even in the case of individuals who were not employed before stroke [6]. Moreover, involvement in work after stroke is a significant factor related to life satisfaction. This is particularly true in the case of young men who are reported to be 2.5 times more likely to be dissatisfied with life if they do not resume work after stroke [16, 17].
In view of the above, work absence due to illness constitutes an important issue from the viewpoint of public health, and a failure to return to work after stroke significantly contributes to this problem [18, 19]. Incapacity for work, in addition to such consequences as isolation and poorer quality of life in individuals affected by stroke, may lead to social and economic problems to be faced by governments [20, 21]. In some cases stroke leads to a complete change in life style, linked with early retirement and disablement benefits. For other individuals, particularly those with families to support, this option presents disadvantages [22, 23]. Due to this, failure to return to work after stroke is frequently perceived as a serious concern which should be investigated in detail. An appraisal of the literature related to this subject matter and published in English and Polish will provide readers of these languages with an understanding of what is known and has been reported in those parts of the world concerning demographic characteristics of people returning to work after stroke, return to work rates, length of time post stroke to return to work as well as health conditions, or personal and environmental factors relating to return to work for the stroke population, as a means of determining critical issues which need to be addressed for stroke survivors desiring to return to work.
The purpose of the study is to provide a narrative review of papers published in the last 11 years in English and in Polish and focusing on demographic characteristics of people returning to work after stroke, on return to work rates, length of time post stroke to return to work as well as related health conditions, or personal and environmental factors associated with return to work after stroke. The study was also designed to present the situation regarding return to work after stroke in Poland in comparison to other countries.
Methods
The search was carried out, in the period from May 2017 to November 2018, in the following databases: Medline (PubMed), Science Direct, Web of Science, Termedia, and Polska Bibliografia Lekarska. The following MeSH (medical subject headings) search terms were defined, to be used in combination, for the English-language databases: stroke, return to work, engagement in work. The terms selected for the search in the Polish-language databases were their respective equivalents, i.e. udar mózgu, powrót do pracy, aktywność zawodowa. Subsequently in order to narrow down the search, the terms “related factors” and “adult population” (czynniki związane, wiek produkcyjny, respectively) were used in combination as additional terms (in all fields).
Inclusion and exclusion criteria
A detailed search was carried out, and filters were applied to limit the search for relevant peer-reviewed articles (research study, systematic review, case study) in English between 2009 and 2018 and in Polish between 2007 and 2018. The starting point for the analysis of articles in English was the systematic review by Daniel et al. from 2009 which included all reports related to return to work after stroke published from 1962 to 2008 [24]. Daniel et al. used a combination of terms for stroke (stroke or cerebrovascular disease) and younger adults (young or adult or middle age) with terms describing social consequences (social and consequence or participation or outcome) or return to work (work or employment and return). The present study reviewed articles in English published from 2009 to 2018. The following inclusion criteria were adopted: full-text article, first stroke, one-sided stroke, return to work in a new occupation or a job performed before the stroke, age 18–65 years. Exclusion criteria: second or another stroke, incapacity benefits received prior to stroke onset. The articles were taken into account if they met the above criteria and if they focused on demographic characteristics of people returning to work after stroke, return to work rates, length of time post stroke to return to work as well as health conditions, personal and environmental factors determining return to work after stroke. Studies which were disregarded included duplicates, articles written in other languages than English and Polish or focusing on detailed effects of rehabilitation and the level of performance, as well as non-peer-reviewed short papers, conference proceedings, posters, and research protocols. Although one of the English-language publications generally mentions rehabilitation, yet the authors do not analyse its effects in detail, and mainly focus on occupational therapy and vocational rehabilitation, as expressed by the keywords and conclusions of the relevant article, that is why the study was taken into account here [25]. Ultimately 21 English-language publications from outside Poland were reviewed and are discussed in the present study (Fig. 1). Although our study is a narrative review, we have provided an adapted version of the PRISMA diagram [26] in Fig. 1 as an illustration of the identification, screening, and inclusion/exclusion process for clarification.
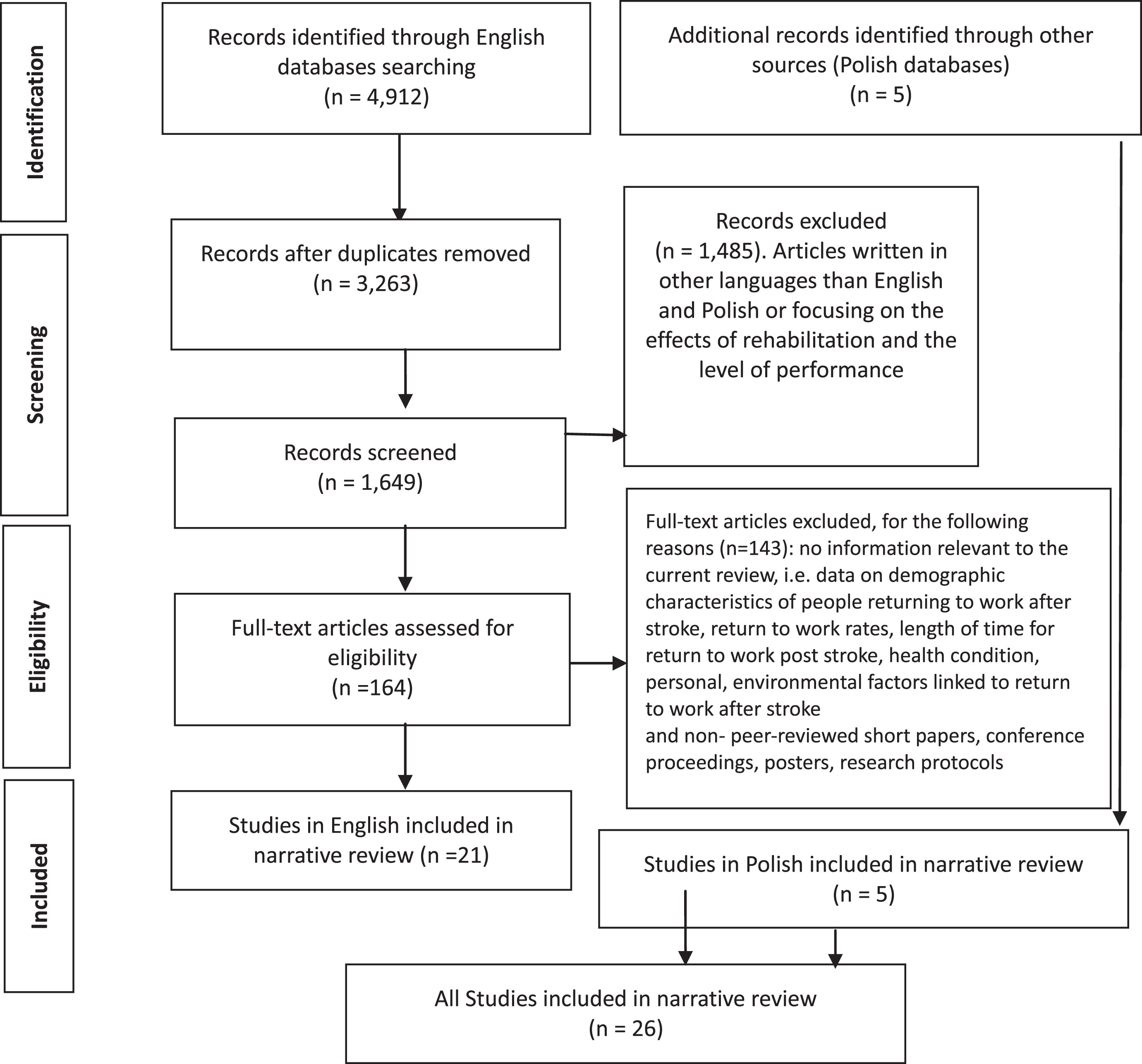
Flow diagram adapted from PRISMA guidelines [26].
Due to the fact that the search of English-language databases identified only one case study from Poland, i.e. an article by Marcinkiewicz and Walusiak-Skorupa [27] describing return to work after stroke in Poland, an additional search was conducted in Polish-language databases (Termedia and Polska Bibliografia Lekarska). The search took into account the most recent eleven years, from 2007 to 2018, and was based on the same inclusion/exclusion criteria, as described above, with two exceptions. As only five articles were identified in the Polish databases, and one of them exceeded the age criterion - mean age of 69 years [28], and the other one took into account rehabilitation effects [29], in order to achieve the purpose of this study, all five articles were reviewed and are discussed in the present study (Fig. 1).
A systematic appraisal of the research reports was performed. The data collected related to the following items: publication date, study type, number of patients, demographics of importance (age, sex), time to follow-up (post-stroke), percentage of stroke survivors’ return back to work, length of time before returning to return to work, positive and negative prognostic factors for return to work. All the potential articles were screened by two independent reviewers, authors of the article. This was done with filters when using the search engines, and those reports which did not address the research question (i.e. failing to provide information about demographic characteristics of people returning to work after stroke, return to work rates, length of time to return to work post stroke as well as related health conditions, or personal and environmental factors associated with return to work after stroke) were excluded. Moreover, studies which were disregarded included duplicates, articles written in other languages than English and Polish or focusing on detailed effects of rehabilitation and the level of performance, as well as non-peer-reviewed short papers, conference proceedings, posters, and research protocols.
Results
The number of records initially identified through English databases search amounted to 4,912. Five records were additionally identified through other sources (Polish databases). After duplicates were removed, 3,263 records were left out. The number of records screened totalled at 1,649. As a result, 1,485 records were excluded (articles written in other languages than English and Polish or focusing on the effects of rehabilitation and the level of performance). Finally, 164 full-text articles were assessed for eligibility. Out of that latter number 143 full-text articles were excluded as they contained no information relevant to the current review, i.e. data on demographic characteristics of people returning to work after stroke, return to work rates, length of time for return to work post stroke, health condition, personal, environmental factors linked to return to work after stroke, and non- peer-reviewed short papers, conference proceedings, posters, research protocols. Consequently 26 studies were included in the narrative review (21 foreign, 5 Polish) (Table 1). They comprised one case study, one randomised controlled trial, seventeen cohort studies, four systematic reviews, and three meta-syntheses.
Return to work after stroke and related health conditions, personal and environmental factors, selected publications
Return to work after stroke and related health conditions, personal and environmental factors, selected publications
RTW – return to work, VR - vocational rehabilitation, NIHSS - National Institutes of Health Stroke Scale, PNF - proprioceptive neuromuscular facilitation, FIM - Functional Independence Measure.
Westerlind and colleagues indicated that the first quartile for return to work was within 2.7 months after stroke and the second quartile for return to work fell within 12.7 months. The mean time to return to work after stroke amounted to three years. Eighty-four subjects (48.3%) returned to work within one year following stroke in a group of individuals aged 63 or younger, following their first ever stroke, in Gothenburg, Sweden [4]. Skolarus et al. showed that the mean post-stroke interval for return to work was 90 days in Mexican Americans and non-Hispanic whites, in south Texas [30]. Similar length of time to return to work post stroke was reported by Hamy – an average of 101 days in a cohort of patients from Amiens, France, below 60 years of age [5]. On the other hand, Ntsiea et al. identified a period of 6 months, in the Gauteng province of South Africa (mean age 45 years) [31] and Langhammer et al. a period of 6 months and 12 months after specialized stroke rehabilitation in nine rehabilitation centres in seven countries (mean age 58.5 years) [32]. Doucet and colleagues found that the mean post-stroke interval for return to work was 19.2 months, in a group admitted after a first stroke to a rehabilitation facility in France (mean age 48 years) [33]. Balasooriya-Smeekens et al. reported that the length of time to return to work post stroke was in the range from 3 months to 2 years in a group of individuals (mean age of 44) participating in an online forum in the UK [34]. Matérne et al. on the other hand reported a far longer period for return to work, from 3 to 9 years, with an average of 5.83 in individuals aged 27–55, in Sweden [35]. Edwards et al. in a systematic review reported that return to work among stroke survivors, aged 37 – 55, was greater over time, with an increase in the median frequencies observed for periods between 0 and 6 months, as well as 1 year, 1.5 years and between 2 and 4 years after stroke [36]. Greatly varied length of time to return to work post stroke was also reported in a systematic review by Daniel et al., taking into account studies carried out at a follow-up of 3 months to 27 years, with a group of publications based on comparable methodologies showing that majority of individuals returned to work 6–12 months after stroke [24].
The time for return to work after stroke in the Polish-language literature was reported to comprise periods ranging from 5 months [27] to 4 years (mean age 64) [37] after stroke. However, the period of 5 months was related to one person only in age 41 years [27].
Percentage of workers who return to work
Fukuzawa et al. showed that only 24 (16%) out of the 150 Japanese patients (mean age 51 years) discharged from a support facility for people with disabilities, returned to work after stroke [38]. Doucet and colleagues reported 32% return-to-work rate in a group of patients (mean age 48 years) admitted after a first stroke to a rehabilitation facility in France [33]. Skolarus et al. studied a group of stroke survivors representing two ethnic groups and reported that 40% of the subjects who had been working at the time of stroke returned to work; generally, however in the case of Mexican Americans the return-to-work rate was lower than in Non-Hispanic Whites (31% vs 50%) [30]. Balasooriya-Smeekens et al. report that in a group of individuals (mean age of 44) participating in an online forum in the UK, between 2004 and 2011, the percentage of workers who returned to work was in the range from 1.7% to 48.3%. [34]. On the other hand, according to Langhammer et al., the relevant rate varied from 7% to 43% in a group of individuals (mean age of 58.5 years) who had participated in a specialized stroke rehabilitation program in nine rehabilitation centres in seven countries [32], and Ntsiea et al. reported that only 20% of workers returned to work following a general stroke care program without workplace intervention, while 60% of the subjects (mean age 45 years) returned to work following workplace intervention, in the Gauteng province of South Africa [31]. Hamy found that 63% of patients aged less than 60 returned to work, in a cohort of patients from Amiens, France [5]. Westerlind and colleagues in a follow-up study carried out in Gothenburg, Sweden showed that 130 (74.7%) out of the 174 individuals aged 63 or less, with first ever stroke in 2009–2010, were back at work six years after stroke [4]. Edwards et al. in a systematic review showed that return to work rates among stroke survivors, aged 37 – 55, reported by studies from 2000–2016, were in the range from 41% to 66% [36]. On the other hand, a systematic review performed by Daniel et al. and taking into account studies from 1962–2008 reported return to work rates among stroke survivors aged less than 65 years to vary between 0% and 100% with a mean of 44% [24].
In the Polish-language literature only three publications were found to report the relevant statistics. Return to work following hospital rehabilitation post stroke was investigated by Czajkowska et al. who reported 11% rate in a group of patients with mean age of 69 [28], and by Tasiemski et al. who found that 24% of the patients (mean age 64) resumed work [37]. The highest rate was reported by Nadulska who found that following rehabilitation in specialist facilities 43% out of the 50 individuals aged 34–65, returned to work after stroke [29].
Personal factors and stroke sequelae and return to work
The most commonly recognized personal factors and stroke sequelae which make return to work more difficult include existing serious functional deficits [4, 39], cognitive (memory and attention) impairments, speech impairments, fatigability, as well as personality changes [25, 40–43]. Researchers also have pointed to unspecified etiology of stroke, longer duration of stay in hospital, higher initial NIHSS scores, higher Rankin scales scores at discharge, the patients’ depressive state long after their stroke and mental breakdown [4, 32], advanced age (60 years or older), lower education level (less than 10 years) [32], sick leave prior to the stroke [4].
In the Polish-language literature it has been suggested that personal factors and stroke sequelae posing hindrance in return to work are depression, mental breakdown [29], permanent disability and dependence on others in daily life [44].
Conversely, the most important factors enabling return to work include mild consequences of stroke: good balance, ability to walk and to use upper extremities [40], as well as the lower degree of disability assessed with the modified Rankin Scale, scores related to cognitive function and motor function on NIHSS [4, 36], as well as greater degree of independence in activities of daily living [36, 38]. Morris examined factors impacting return to work after stroke in young adults, and suggested that successful resumption of work is linked with individual factors such as absence of aphasia, higher functioning on discharge from hospital, lack of apraxia, no psychological disorders, preserved cognitive abilities, low alcohol intake prior to stroke as well as being male and not being black [6]. Skolarus and colleagues also discussed ethnic differences in return to work. Mexican Americans were less likely to return to work due to greater neurological deficits and lower level of education, compared to non- Hispanic whites [30].
Barriers and facilitators/supports for return to work
The most frequently recognized barriers for return to work after stroke resulted from a lack of stroke-related knowledge among employers, and consequently a lack of understanding and support from them [34, 45] and on the other hand a lack of support provided to the employer and problems with financing and integrating this support into the existing provision of services [39]. Some researchers also emphasized problems resulting from significant costs of accommodating for stroke survivors’ needs at the workplace [40] and from a lack of family [33]. Furthermore, the authors mentioned heavy physical work [40, 45] and work-related stress [41] as barriers for return to work.
The most important factors enabling return to work, include good interpersonal relations between the stroke survivor, employer and colleagues [6, 45], acceptance of stroke-related impairments, reinforcement of social support for stroke survivors at the work place, motivation for returning to work [41–43, 46] as well as the employers’ ability to accommodate for the stroke survivor’s needs at the work place [40]. The authors also pointed out that the type of job performed also determined return to work [6, 40]; more specifically blue collar (manual) workers resumed work earlier, while white collar (office) workers more often returned to work after a longer period of time from stroke [6]. Other factors linked with re-engagement in work included higher socioeconomic status, full-time employment before stroke [6], positive attitude toward work [6, 34], social support [6, 47], early involvement of an occupational physician [33, 43] as well as counselling and support provided by stroke specialists to employers [39], and good communication between healthcare professionals and employers [42]. The researchers also established that patients who resumed driving were far more likely to engage in work [5, 33].
The facilitators for a return to work, identified by the Polish authors include rehabilitation based on modern kinesitherapeutic methods, i.e. proprioceptive neuromuscular facilitation and neuro-developmental treatment (Bobath concept) [29] as well as follow-up examinations of subjects returning to work – a holistic assessment of health predispositions from the viewpoint of the previous duties at work [27].
Environmental factors and return to work
The main environmental factors preventing stroke survivors from resuming activity include: need for long-distance mobility, inconvenient environmental conditions such as bad weather and wheelchairs making it difficult to communicate with colleagues or to perform heavy physical work [45]. The environmental factors linked with re-engagement in work include personal adapted equipment, accessible environments, transport services, access to education and information [40, 45] as well as environmental workplace adaptations [42, 46], and adjustments such as phased working and flexible work [42].
Return to work and vocational rehabilitation
The related studies present a variety of objectives and requirements for vocational rehabilitation post-stroke. Matérne and co-authors point out that the purpose of specially designed rehabilitation is to enable patients to take active part in the entire process, and that the related effects should be strengthened by the support from rehabilitation personnel, employers, and colleagues. Furthermore, well-planned vocational rehabilitation process fosters a patient’s partnership with the employer, keeps up his/her motivation and increases awareness of abilities that facilitate or hinder return to work [35]. Sinclair and colleagues, in a study investigating the related issues in a selected region of England, assessed patients’ access to vocational rehabilitation after stroke in the relevant county. They reported that the needs of patients with mild stroke were not sufficiently satisfied, and the fact is linked with a general perception that vocational rehabilitation is “unimportant” because of other priorities connected with recovery. In their conclusions the authors emphasize that early vocational rehabilitation should be provided by an integrated, cross-sector multi-disciplinary team with adequate training and a good knowledge of guidelines and best practices. It is also necessary to apply integrated commissioning of services to be delivered by health and other sectors [48]. Other authors also emphasise importance of workplace procedures strengthening effects of vocational interventions, and facilitating return to work post-stroke, such as workability assessments, workplace visits [31] and assistance provided by an occupational health specialist at the workplace [5].
Consistently with the above, it has also been suggested that stroke survivors’ chances for return to work are increased by adequately planned post-stroke rehabilitation phase while lack of or insufficient duration of vocational rehabilitation produces adverse effects [5]. Likewise, Soeker et al. pointed out that engaging in rehabilitation, combined with physiotherapy intervention and specific vocational rehabilitation, facilitated the patients’ post-stroke resumption of their worker roles. An important aspect of the above is linked with that fact that by engaging in rehabilitation, patients are encouraged to live their lives as normally as possible as a result of which ultimately they consider returning to work [25]. On the other hand, a better understanding of risk factors for no return to work is necessary to introduce more customized, and consequently, more effective, vocational rehabilitation, as pointed out by Westerlind et al. [4].
Return to work and quality of life after stroke
A study by Nadulska shows that 43% of the subjects after stroke report improved quality of life after return to work. Factors which, according to the study participants, contribute to the ability to return to work and consequently to improved quality of life most importantly include a decreased need for orthopaedic aids [29]. The same study confirms adverse effects of stroke on the patients’ economic, social and vocational status, which is closely linked to quality of life [29]. Also Morris in a systematic review, established that return to work in young adults is related to higher quality of life [6]. Tasiemski and colleagues compared research findings related to quality of life after stroke in Poland, Israel and Sweden and showed that in all these countries loss of employment was among factors adversely affecting quality of life. Furthermore, there was a significant difference in the stroke survivors’ satisfaction related to their financial situation. Notably, in the Polish study 12% of the subjects were satisfied compared to the Israeli study which reported 47% satisfaction rate in the relevant group. The authors conclude that the ability to return to work is one of the most important factors determining quality of life after stroke [37]. Czajkowska and co-authors argue that improved quality of life after stroke is associated with the expected return to one’s previous job, or with chances to reengage in work after acquiring new qualifications [28]. Jabłońska and co-authors emphasize that, in most cases, decreased quality of life is associated with stroke consequences causing permanent disability and resulting in partial or complete dependence on others in daily life, and leading to lower involvement in work, in one’s family, and in the community [44].
Discussion
Based on the appraisal of Polish-language studies published between 2007–2018 it can be concluded that, in contrast to English-language literature related to this subject matter, there is a scarcity of studies related to return to work after stroke in Poland [27–29, 44]. The search produced only five records in the Polish databases compared to 3,263 records in the English databases (after duplicates removed). This difference shows that the system of vocational rehabilitation in Poland is poorly developed, and this may explain the scarcity of related research. Hence, there is a need for immediate action to ensure this type of rehabilitation to Polish patients with stroke.
Length of time to return to work post stroke
The mean timing for return to work after stroke varies in the English-language literature, comprising periods of 3 to 6 months post stroke, 12 to 18 months post stroke, and up to 3 years after stroke [6, 4]. In Poland return to work post stroke was only investigated by one study which reported a period of four years [37]. No general conclusions may be drawn from one case study which reported the subject’s return to work after 5 months [27].
Percentage of workers who return to work
The appraisal of the Polish-language literature shows that stroke survivors’ ability to return to work is varied, reaching the rate of up to 43% (this does not take into account the 100% value from the case study by Marcinkiewicz and Walusiak-Skorupa [27] (since it is related to one person only). By contrast, in the English-language literature, the most frequently reported values are up to 74.7%. The review study by Daniel et al. reports a value of 100% but in relation to only six people aged 30–65 years, with undetermined level of disability, and unknown length of time before they returned to work after stroke [24].
The above data and the current information related to the labour market and very low unemployment rates in Poland, clearly show that efforts should be taken to facilitate return to work post-stroke to all the individuals showing related potential.
Factors linked to return to work post stroke
The English-language publications point to a large number of factors linked to return to work after stroke. Compared to these, the Polish authors discuss a far lower number of the related factors, which may result from a relative scarcity of studies investigating the issue, as well as a failure to use specific tools in determining the relevant predictors. The Polish authors mainly focus on return to work in relation to quality of life [28, 44] and personal factors such as depression, mental breakdown [29] and permanent disability [44], disregarding environmental factors as well as the relation between vocational rehabilitation and return to work. The Polish researchers emphasise that the ability to return to work is one of the most important factors determining quality of life after stroke [37]. However, there seems to be a disturbingly significant difference in stroke survivors’ satisfaction related to their financial status. A comparison of findings reported by a Polish study and an Israeli study (satisfaction rate in Poland nearly four times lower) [37] provides evidence on the one hand suggesting that the Polish welfare system is imperfect and on the other hand reflecting differences in the standard of living.
A study conducted by Polish researchers [29] presents findings on adverse effects of stroke in the patients’ economic, social and vocational status which are consistent with those reported by authors from other countries [4, 6]. More specifically the Polish authors have concluded that even if the patients’ intellectual capacities are intact post-stroke, many of them experience motor dysfunctions which lead to mental breakdown and to withdrawal from various areas of social, vocational and family life. They also emphasize the significance of such problems as post-stroke disability and forced retirement from work as well as a necessity to use orthopaedic equipment; on the other hand, they highlight the importance of rehabilitation based on modern kinesitherapeutic methods as a factor favourably affecting return to work after stroke [29]. Conversely, the English-language literature emphasizes the importance of vocational rehabilitation [4, 48], which is overlooked in Polish-language publications.
These differences between the Polish-language literature and the English-language literature may be linked with the poor level of vocational rehabilitation in Poland, due to the fact that its importance has been overlooked/underestimated by the relevant authorities. This may partly result from the fact that in recent decades Poland had very high unemployment rates. Today the situation is greatly improved, therefore the demand for employees is considerably increased. Therefore, it would be beneficial to provide better access to post-stroke vocational rehabilitation in Poland. Effective operations in this area as well as improved return-to-work rates will ultimately lead to reduced burden to the state budget required for healthcare and welfare benefits. Return to work will also enable individuals with stroke to resume their roles in the society and to be more involved in the community and family life. Implementation of a uniform approach to vocational rehabilitation would provide an opportunity to reduce the disproportions in the numbers of people returning to work.
The current narrative review shows that issues related to vocational rehabilitation and return to work post-stroke have been thoroughly investigated in the English-language literature, and they are regularly monitored. On the other hand in Poland, even though problems related to vocational rehabilitation are known, they tend to be underestimated and overlooked. The present narrative review should provide encouragement for more comprehensive research designed to investigate various aspects of and factors related to Polish stroke survivors’ return to work. The authors of this study are currently working on detailed analyses focusing on return to work post-stroke in selected regions of Poland.
Strengths and limitations
The main limitation of the current study is linked with the fact that a comprehensive comparison of findings reported in Polish and English-language literature was not feasible due to the large difference in the number of publications qualified for the review. Furthermore, compared to the English-language studies, the quality of methodology applied in the Polish-language publications was less advanced, yet they were taken into account here, being the only related publications in our country. The latter fact also explains why, as an exception, we included in the review two Polish-language studies which did not meet all inclusion criteria, one of these applied different age criterion and the other took into account rehabilitation effects. By excluding these two studies, we would only have been able to take into account 3 Polish-language publications, one of these being a case study. Another limitation of this study lies in the fact that we applied a method of narrative review rather than systematic review, and given the diversity of the publications taken into account, the conclusions from this assessment should be considered as preliminary. On the other hand, the importance and strength of our narrative review is linked with the fact that this is the first review presenting return to work post-stroke in Poland, by comparison to other countries. The study may provide an impulse for creating a methodologically consistent database related to return to work post-stroke in Poland.
Conclusions
In summary, medical professionals in Poland should pay attention to the current situation connected with return to work since the ability to resume work is one of the major determinants affecting quality of life post stroke and because identification of factors enabling return to work after stroke may lead to immense benefits not only for employees with stroke, but also for employers and society as a whole. It is necessary to emphasize the importance of vocational rehabilitation, as a factor of great significance in efforts to enable stroke survivors’ return to work. There is a need for further efforts to raise awareness of stroke related consequences, and for measures introducing effective mechanisms for providing support to stroke survivors and enabling them to resume work. The English-language literature identifies a large variety of factors determining whether or not stroke survivors return to work. Return-to-work rates up to 74.7% seem to reflect effectiveness of vocational rehabilitation process, which may be recognised as a model to follow. Further research in countries with higher return-to-work rates should aim at defining uniform guidelines for post-stroke vocational rehabilitation; this would ultimately facilitate implementation of vocational rehabilitation in countries with lower rates in this area.
In view of the lack of more accurate research results, our findings effectively provide insight into the situation related to return to work after stroke in Poland compared to other countries and such determinants as positive/negative health conditions, as well as personal and environmental factors associated with return to work after stroke.
This narrative review on the one hand confirms the fact that return to work is a complex issue with a variety of aspects which are well-known from English-language literature and on the other hand reflects the insufficient awareness of the problems connected with return to work post-stroke in Poland as well as broadly understood vocational rehabilitation which in Poland seems to be underestimated. It is necessary to conduct further high-quality in-depth research related to this problem in Poland which would require estimation of the minimum size of population sample, detailed stroke-related inclusion criteria, detailed definitions related to return to work and the type of job, as well as participation in and the duration of rehabilitation.
Conflict of interest
None to report.