
Abstract
BACKGROUND:
Orthopedic and obstetrician-gynecologist (OB/GYN) surgeons have risks for musculoskeletal disorders (MSD) during work in the operating room (OR). Risks for MSD have not been identified as a result of work outside the OR or during non-work tasks.
OBJECTIVE:
The purpose of the study was to determine risk factors for MSD in an orthopedic and OB/GYN surgeon.
METHODS:
A case study format and mixed method design were used to gather data by using the Rapid Upper Limb Assessment (RULA) to measure MSD risks in the OR; the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) to measure surgeons’ upper extremity disability; observation of surgeon office hours; and semi-structured interviews to gather qualitative data.
RESULTS:
Both surgeons had risks for MSD during occupational performance outside of work, with some risks similar to those experienced at work. Both surgeons had MSD risks during work inside and outside the OR. Both surgeons experienced MSD symptoms exacerbated by work and non-work tasks.
CONCLUSIONS:
Identifying and reducing MSD risk should include a comprehensive analysis of occupational performance for orthopedic and OB/GYN surgeons.
Background
Introduction
Musculoskeletal disorders (MSD) are defined as injuries to the musculoskeletal and nervous system as a result of risk factors including overexertion, repetitive motion, awkward or sustained postures, localized pressure, and vibration [1]. These risk factors are typically reduced by altering standing positions, modifying equipment design, and optimizing appropriate breaks [1]. In 2015, MSD accounted for 31% of the total cases of nonfatal occupational injuries requiring days off of work among all workers, making MSD one of the leading causes of absenteeism in the workplace [2].
In a systematic review, Long, Bogossian, and Johnston [3] found prevalence rates of 45%, 40%, and 35%, respectively, for MSD of the neck, shoulder, and upper back among midwives, nurses, and doctors. Risk factors for MSD in surgeons, doctors, and dentists included prolonged static postures, repetition, awkward and cramped positions, inadequate training, and age [4]. Ruitenburg, Frings-Dresen, and Sluiter [5] found that, unlike hospital doctors, surgeons who worked in sustained postures were affected by fatigue. Similarly, Cavanagh, Brake, Kearns, and Hong [6] found dynamic and static postural stresses lead to fatigue and disability in surgical practice. Researchers reported that laparoscopic surgeons lacked proper knowledge regarding how their techniques and postures may be contributing to their overuse injuries [7].
Although researchers have described MSD risks for surgeons within the operating room (OR), risks for MSD have not been fully identified during work outside the OR or during non-work activities for orthopedic or obstetrician-gynecologist (OB/GYN) surgeons. Orthopedic surgeons correct problems that arise in the skeleton, including the ligaments and tendons [8]. OB/GYN surgeons perform surgical operations focusing on disorders associated with the female reproductive system [9]. The purpose of this study was to identify MSD risks for an orthopedic and an OB/GYN surgeon. The research question was: What are the risk factors for the development of MSD for an OB/GYN and orthopedic surgeon as a result of work in and outside of the OR, and occupations outside of work? A more comprehensive analysis of risk factors across roles and contexts can provide opportunities for surgeons to understand the scope of MSD risk and opportunities to modify these risks.
Literature review
Gender and age have been described in relationship to MSD risk factors in surgeons. Franasiak et al. [10] found that female gynecologic surgeons who performed minimally invasive surgery (MIS) had more physical strain than did their male counterparts. Females reported more shoulder discomfort and received treatment for upper extremities more often than did males [11]. Younger vaginal surgeons and dentists had a higher frequency of work-related MSD [12, 13] than older dentists and vaginal surgeons; however, orthopedic surgeons’ rate of MSD increased with age [14].
Findings on the impact of years of experience on MSD occurrence have been varied [10, 13–16]. After 21 years of experience, orthopedic surgeons had more work-related injuries [15]. AlQahtani et al. [14] also found that more than 10 years’ experience was associated with MSD of more body regions. Conversely, surgeons performing laparoscopic procedures had fewer symptoms as they gained experience [16, 17]; inexperienced vaginal and gynecologic surgeons who performed MIS were at higher risk for work-related MSD [10, 13]. Similarly, Lee et al. [18] found that muscle activity from the trapezius was greater when surgeons were new to laparoscopy. Related to experience, training in OR ergonomics has either not been shown to reduce MSD [10, 19] or has been inconclusive in its impact on MSD risk [20].
Researchers have shown that the physical OR environment can influence MSD occurrence. Cutner, Stavroulis, and Zolfaghari [21] found that fixed equipment in older ORs resulted in awkward positions, restricted movement, and safety hazards. In contrast, surgeons had fewer MSD symptoms when OR tables were at pubic height; repositioning the monitor achieved more neutral head, neck, and spine for surgeons [16]. Singh et al. [22] found that chairs that dispersed pressure reduced discomfort during vaginal surgery, and some chairs were preferred by surgeons. A patient’s positioning often determined the surgeon’s placement in the OR, leading to increased MSD risk [23, 24]. Surgical tools causing non-neutral wrist position increased MSD risk [25]. Size of surgeons’ hands influenced surgeons’ choice of tool handle size [26], and surgeons using laparoscopic tools showed increased muscle exertion [18]. Redesigned hammers reduced risk for injury and improved performance for orthopedic surgeons [27].
Researchers have found that task demands can contribute to MSD risk factors. In comparison with hospital doctors, surgeons performed longer durations of standing and fine repetitive movements [5]. Surgeons also reported neck and arm pain along with difficulties coping with job demands [5]. High finger exertion associated with wrist postures was shown to lead to MSD in surgeons [28]. For doctors performing colonoscopies, Maciel et al. [28] found that sustained pincer grip was a risk for injury. In their study of gynecologists, Craven, Franasiak, Mosaly, and Gehrig [29] showed that surgeons often used near maximal intensity of exertion. In their investigation of workplace ergonomics, Maciel et al. [28] showed surgeons had a high potential for injury to the wrists, hands, and fingers during colonoscopy with clamped hands, static upper extremity postures, and forced wrist flexion and extension. Researchers have also shown a positive relationship between body mass index (BMI) of patients and reports of physical strain by surgeons using MIS through laparoscopy [10].
Researchers investigating MSD risk factors for surgeons have focused their assessments on the OR environment and surgeons’ tasks during procedures, yet risks can also arise from work tasks outside of the OR and non-work tasks. Utilizing a case study format, researchers of the current study expanded identification of risk factors for MSD in two surgeons by investigating demands of surgical procedures, surgical environment, work beyond surgical procedures, and occupations outside of work.
Method
Research design
This study took place in a community hospital for general care. The researchers studied one orthopedic surgeon and one OB/GYN surgeon using a case study, mixed method design to gather qualitative and quantitative data [30].
Participants
Surgeons met inclusion criteria if they performed orthopedic or obstetric/gynecologic surgery in the hospital setting. In a purposive sample, the researchers recruited one orthopedic surgeon and one OB/GYN surgeon to participate in the study. These surgeons had conversed with the primary investigator (PI) and other occupational therapy (OT) colleagues about MSD risk during work and were interested in formalizing study of risk factors. According to Portney and Watkins [31], purposive sampling can yield participants who are effective informants and who meet specific criteria for the study. The PI completed informed consent procedures with both surgeons and enrolled them in the study.
Measures
Rapid Upper Limb Assessment (RULA)
The RULA is used to measure exposure of a worker to ergonomic risk factors associated with upper extremity MSD [32]. Risk factor variables include posture (position) of the upper extremities, neck, trunk, and leg; muscle use (static or repetitive); force/load (objects used and categorized by weight: less than 4.4 lb, 4.4–22 lb, or more than 22 lb, and characterized by repetition, static use, or shocks with use); and repetition for the upper arm, lower arm, wrist, neck, trunk, and leg regions [32]. The RULA yields scores of MSD risk level on a four-point scale of exertion [32]. Scores and definitions of scores include: (a) acceptable if not maintained or repeated for long periods (score of one or two), (b) further investigation, change may be needed (score of three or four), (c) further investigation, change soon (score of five or six), and (d) investigate and implement change (score of seven). The body is divided into Section A, arm and wrist, and Section B, neck and trunk, and only one side of the body is evaluated at a time [32].
Researchers or clinicians should use published training materials to use and score the RULA [32]. OT students have successfully used the RULA to measure MSD risk factors in simulated observations; there were no differences in students’ scores when compared to those of clinicians [33]. The RULA has also been used for measurement of MSD risks during gynecologic and colonoscopy procedures [24, 29]. Although there are no normative data available, researchers have established construct validity and interrater reliability for the RULA [32]. The RULA was selected to measure MSD risk during surgery observations due to the access of the tool and training materials, psychometric properties, established use by OT, published use for measurement of MSD risk of other surgeons during operative procedures, and practical application for use in the OR [32, 33].
Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH)
The QuickDASH measures the “physical function and symptoms in persons with any or multiple MSD of the upper limb” through self-rating of items [34, p. 1038]. The QuickDASH has a Disability/Symptom section and two optional modules, Sports/Performing Arts and Work [34]. Each item is self-rated on a Likert scale with scores ranging from one to five. Raw scores are converted to final scores through established mathematical calculations; final scores range from 0–100 for the QuickDASH and each optional module. Lower scores indicate higher function, and higher scores indicate lower function [34].
The QuickDASH has been used extensively in clinical and research applications and has established psychometric properties [34–38]. Franchignoni et al. [39] reported 10.83 and 15.91 points as the minimal clinically important difference for the DASH and QuickDASH, respectively. Normative data for the DASH can be applied to the QuickDASH due to the similarity of construct validity and responsiveness of the two tools [40]. Normative data for the general US population for DASH Function/Symptom, DASH Optional Sports/Performing Arts Module, and DASH Optional Work Module have been es9lished as 10.1, 9.75, and 8.81, respectively [40]. The QuickDASH was selected to measure physical function and symptoms of upper extremity MSD of the participants in the study.
Interview
Researchers developed 13 open-ended interview questions to understand MSD risks across roles and occupational performance [41]. Questions were refined based on feedback from an expert panel of OT faculty (See Appendix).
Procedures
The study was approved as exempt by the Institutional Review Board (IRB) at the University of Indianapolis, and IRB at the hospital setting. Researchers trained for data collection by (a) completing a mock interview with the PI, (b) rating and scoring MSD risks on the RULA while viewing a video of a total hip arthroplasty, (c) reviewing procedures for surgery observation, and (d) reviewing scoring and normative data for the QuickDASH. Training for data collection enhanced researchers’ understanding of the data for analyses.
Data collection
The PI, a registered occupational therapist and certified hand therapist, and one student researcher used the RULA to measure MSD risk for each surgeon during (a) a right total knee arthroplasty (TKA), (b) revision of a right TKA, and (c) a laparoscopic assisted vaginal hysterectomy with salpingectomy. Following the surgery observation, the researchers collaborated to determine a single RULA score. During the surgical procedures, the researchers also recorded field notes of observations of surgical instruments and other objects used by surgeons, types of grip or pinch used for holding instruments, and presence or absence of rest.
The PI and one student researcher conducted a single semi-structured interview with each surgeon lasting 22 minutes for the first surgeon and 28 minutes for the second, which was audiotaped and transcribed, and also recorded handwritten notes during the interview. The interview included questions related to demographics, hours of occupations, roles, work and home demands, risk factors, musculoskeletal symptoms, technology use, and daily routine (See Appendix). The PI recorded field notes of occupational performance during the orthopedic surgeon’s office hours. Researchers used OSHA [1] to define and quantify MSD risks in field notes of office hour observation; established risks by OSHA also guided researchers’ identification of MSD risk in transcripts of interviews. These risks included overexertion, repetitive motion, awkward or sustained postures, localized pressure, and vibration [1]. Lastly, surgeons completed the QuickDASH at the end of a typical work week and mailed the document to the researchers.
Data analysis
Final RULA score for each surgeon was calculated using established procedures to determine exposure level to risk factors of MSD. The researchers analyzed, organized, and interpreted the transcribed data of each interview through open coding [30, 42]. Open coding was accomplished by each researcher first independently reading transcripts and field notes to identify terms and descriptions related to MSD risk; researchers then collaborated to ensure comprehensive descriptions of MSD risk. To enhance interpretive validity, surgeons completed member checking and approved analyses [43, 44]. Based on surgeons’ descriptions of time spent in the OR, work outside of the OR, and in non-work activities, researchers calculated percentage time spent for a single week (168 hours) during each. Researchers scored the QuickDASH and compared scores to the normative data.
While completing data collection and analysis, researchers implemented the process of triangulation, in which multiple methods were used to tabulate and analyze risk factors for MSD for the surgeons which increased the validity and trustworthiness of the data analysis [30]. The goal of the mixed methods design was to provide a comprehensive understanding of risk factors for MSD through triangulating the data [30]. To support the validity of findings and document the thought process of all decisions in the data interpretation process, researchers completed an audit trail [31].
Results
Case 1: Orthopedic surgeon
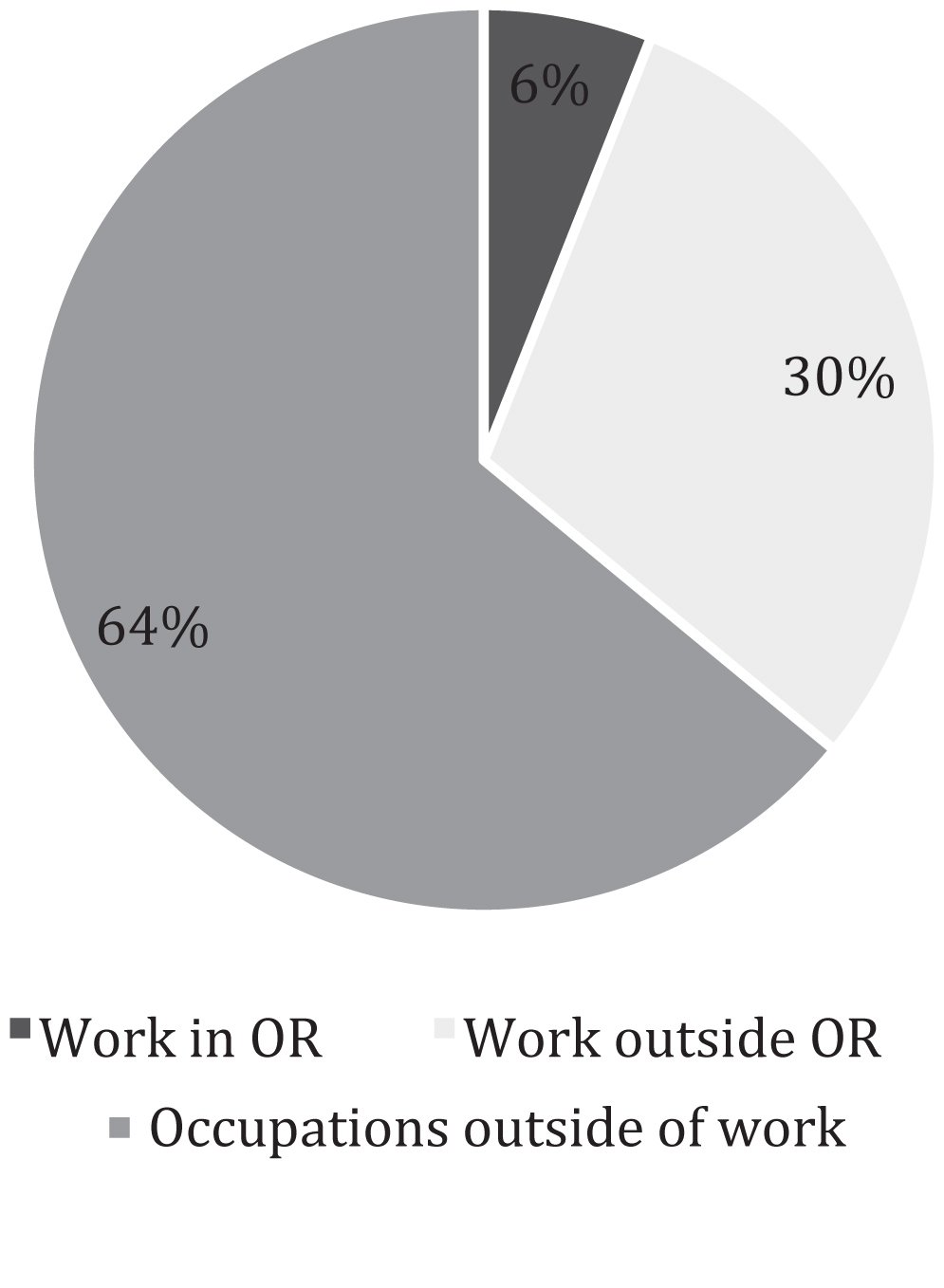
The orthopedic surgeon was 40 years old and had 13 years of experience. Occupations of the orthopedic surgeon included home management, care of pets, child rearing, volunteer participation, leisure participation, rest and sleep, and work. His roles included parent, home manager, pet owner, spouse, coach, woodworker, cook, and surgeon. Risk factors identified included repetitive movement, awkward and sustained postures, vibration, positioning, lack of rest, and sustained and repetitive grip and pinch. Percentage of weekly time use for occupations outside of work, and work in and outside of the OR showed a greater percentage of time was spent in occupations outside of work (Fig. 1).

Percentage Time Use in Single Week for Orthopedic Surgeon. Note: Operating room (OR).
The orthopedic surgeon’s description of occupational performance outside of work revealed MSD risks. Volunteer and leisure participation included transporting children to sports activities and using upper extremities repetitively: “I coach baseball and soccer, always, sometimes softball... I throw at least an hour solid of batting practice about once or twice a week... I probably throw on average 200–400 pitches with those kids” (Lines 28–33).
The orthopedic surgeon recognized that the risk factor of vibration with woodworking tools at home was similar to that experienced in his job as an orthopedic surgeon: “I do woodworking on the side as well and I may spend four to five hours probably per week ... which includes use of similar vibratory tools... two years ago I would get up around four and... work in my woodshop until 6 a.m. and then go into work and then probably come home and... if I had the time, do some more stuff at night” (Lines 99–102). In reference to woodworking, the surgeon described being “pretty good about being ergonomic” (Line 92). He was aware that his woodworking resulted in muscular fatigue, reporting that his hands got tired when carving wood. In addition to woodworking, care of pets by the orthopedic surgeon could increase MSD risk during lifting and carrying loads: “I... fed the chickens last night, and so I carried a 40-pound bag of chicken feed 250 feet... up and down a hill... [I had to] fill buckets [with chicken feed]” (Lines 46–48).
The surgeon described some occupations he no longer performed that involved MSD risks of vibration and sustained grip, and produced MSD symptoms of upper extremity numbness and tingling. For example, lawn care, as a part of home management, was described as a leisure activity. “I actually enjoy mowing the grass... when I get the chance to, but it’s a three-and-a-half-hour process, so I don’t do it any longer” (Lines 70–71). The orthopedic surgeon also described current and past MSD that was influenced by occupations outside of work. The surgeon monitored arthritis symptoms in his right hand, and believed they resulted from sustained and repetitive pinching during IADL, such as meal preparation which he described as an enjoyable leisure activity. The orthopedic surgeon’s primary concern was his lower back pain that he believed could be from inadequate rest and sleep due to work demands. However, the surgeon was frequently involved in other IADLs at home that he recognized could also contribute to the pain.
On the QuickDASH, the orthopedic surgeon rated himself as having mild difficulty with heavy household chores, recreational activities, and sleep. In contrast, he rated himself as having severe difficulty with bathing his back and rated his social participation as slightly limited. The orthopedic surgeon identified participation in baseball and woodworking on the Sports and Performing Arts modules of the QuickDASH with a score of 25, reflecting disability greater than the normative value of 9.25 (Fig. 2). He scored 20.45 on the QuickDASH with the normative value of 10.10 (Fig. 2).
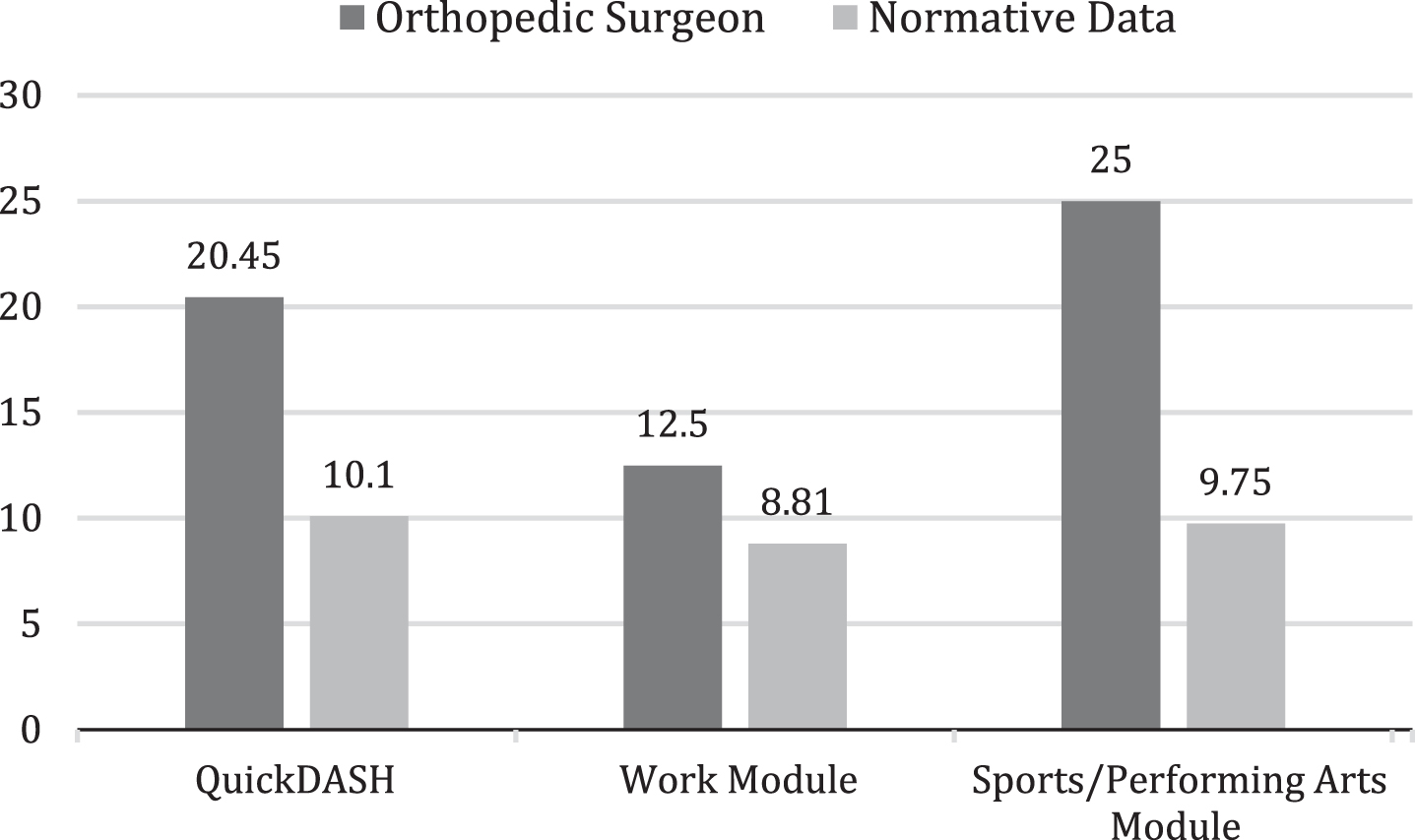
Comparison of Orthopedic Surgeon Scores of QuickDASH to Normative Data.
Risks for MSD during surgical procedures resulted from: (a) the type and location of surgical procedure for the patient, (b) surgeon hand dominance, (c) patient characteristics, and (d) surgical instruments used. For example, the orthopedic surgeon preferred a right THA rather than a left due to improved ability to use his dominant hand and reduced exertion needed for a right THA: “I have to move [into] position on a left hip more” (Lines 174–176). Revision of total joints was more demanding because of awkward postures and longer duration of standing. Larger patients with more scar tissue required more muscle power and torque with surgical instruments. The orthopedic surgeon commented on “surgeons’ disease” recognizing sustained neck flexion during operative procedures (Line 187). Neck position influenced MSD symptoms: “if I put my shoulder back [and] lean my head far back my arms go to sleep” (Lines 185–186).
Risks for MSD were also increased because of surgical instruments. Drills and bone saws caused vibration and required sustained gripping; gripping was also needed for hammers and chisels. The surgeon frequently changed tools or parts of tools, necessitating repetitive gripping and pinching. Forceful pinching was also observed as the surgeon removed small pieces of bone and soft tissue. The orthopedic surgeon often used his left hand as a stabilizer and occasionally utilized his right hand as a hammer, demonstrating risk for mechanical compression.
The orthopedic surgeon completed consecutive surgeries using neighboring ORs with no breaks between procedures. Pauses in surgical procedures were rarely observed, however, were noted one time when lab results were delayed; mixing of cement during TKA required a two-minute pause during the procedure. The orthopedic surgeon occasionally rested upper extremities on patients during operative procedures.
Score for the RULA for the orthopedic surgeon was a seven, the highest score, defined as indicating a need to assess and implement a change. The score was reached prior to the end of the surgical procedure, indicating MSD risk greater than the tool measured. Highest MSD risk as quantified by the RULA included lower arm, neck, and wrist twist, with an addition of neck position for the orthopedic surgeon. The surgeon’s score on the QuickDASH work module exceeded the normative value of 8.81, showing disability of the upper extremities (Fig. 2).
Descriptions and observations of work outside of the OR showed MSD risks that included awkward and sustained postures, repetition, and infrequent rest. Work tasks included examining scheduled patients, documenting operative procedures and office visits, using the computer to review patient charts, and fulfilling scheduled on-call hours at the hospital. The orthopedic surgeon spent “15–20 minutes of documentation per person,” (Lines 62; 64-65), primarily using a hands-free dictaphone. Documentation required “2 to 3 hours of computer work at home” (Lines 55-56; 121–123) each work night, 6 hours on a tablet with a keyboard attached at work, and another hour on his cell phone.
The orthopedic surgeon recognized MSD risk especially during work outside the OR. He described his worst posture occurred during patient examinations. During examinations, he placed his laptop on his thighs, requiring neck flexion to view his laptop screen, and used a rolling stool with no back support. He lifted and palpated extremities of patients from a seated position, causing end-range extremes of neck position, excessive hip flexion, and reversal of normal spinal curvatures. Despite lower back and neck pain, the surgeon used these postures to create a more informal atmosphere with his patients. Outside of examination rooms, the orthopedic surgeon demonstrated sustained and awkward flexed postures of the neck and back to use his computer and cell phone; during these same tasks, additional MSD risk of mechanical compression to the posterior elbow, and volar forearm and wrist were observed.
Case 2: OB/GYN surgeon
The OB/GYN surgeon was 43 years old and had 16 years of experience. Occupations of the OB/GYN included child rearing, care of pets, home management, meal preparation, leisure participation, rest and sleep, and work. Her roles included parent, home manager, pet owner, spouse, gardener, and surgeon. Risk factors identified included repetitive movement, sustained and awkward postures, positioning, lack of rest, and sustained and repetitive grip and pinch. Percentage of weekly time use for occupations outside of work, and work in and outside of the OR showed a greater percentage of time was spent in occupations outside of work (Fig. 3).
Percentage Time Use in Single Week for Obstetrician/Gynecologist Surgeon. Note: Operating room (OR).
Although MSD risks were not explicit in her descriptions, the OB/GYN surgeon recognized that home management tasks had similar demands on her body as did work demands. Her descriptions show evidence that insufficient rest, lifting, and sustained postures were possible risks for MSD. The OB/GYN surgeon described that “yard work and... deeper cleaning activities [at home] where I’m...bending and squatting down and lifting...probably affect me in similar areas to where my work does (Lines 247–248). Her description of time spent on child rearing that included transporting children, yard work, and home management, in combination with hours spent working, contributed to prolonged exertion and insufficient rest: “And I don’t know if that’s because I’m already sore from the work activities so those things just exacerbate it ... . I certainly would say the majority of my physical stress is at work” (Lines 250-251). Hours of activity beyond work expanded task demands for the OB/GYN: “I spend 3 hours in the evening and an hour in the mornings so... during the week and on weekends it could be around 8 hours a day” (Line 52–54) doing leisure activities. Depending on her method of task performance, care of pets could yield MSD risks: “I have two dogs and a rabbit” that need “corralled or cleaned up after. ... [I least enjoy] real dirty stuff like cleaning out the rabbit cage” (Lines 36, 38, 62-63).
On the QuickDASH, the OB/GYN surgeon rated herself as having mild difficulty with heavy household chores, recreational activities, and sleep. The OB/GYN surgeon also reported mild difficulty with opening a tight or new jar and slight limitation in performing daily activities outside of work. No sports or performing arts activities for the OB/GYN were reported. The OB/GYN surgeon scored 13.64 on the QuickDASH with the normative value of 10.10 (Fig. 4).

Comparison of Obstetrician/Gynecologist Surgeon Scores of QuickDASH to Normative Data
MSD risks were evident from descriptions and observations of surgical procedures, and included sustained and repetitive grip and pinch, awkward postures, and high exertion. The OB/GYN surgeon reported that surgical task demands resulted from: (a) the type and location of surgical procedure for the patient, (b) surgeon hand dominance, (c) types of instruments used, and (d) hand use needed to use instruments. She preferred to be perpendicular to the patient’s left side to direct surgical instruments with her dominant right hand. She described vaginal surgeries as “pot luck ... [depending] on the size and... width of the patient’s pelvis and vaginal area...I might be doing lots of pulling and torque” (Lines 160–163). Sustained pistol grip with frequent use of trigger by the right dominant hand was observed during laparoscopy. Additionally, vaginal procedures demanded sustained asymmetric postures of the head, neck, and trunk as well as high exertion for repetitive gripping and pinching with end-range extremes of wrist and forearm positions.
The OB/GYN surgeon described greater task demands when patients were large, had excessive scar, and a history of trauma: “I notice a huge difference in a patient that is more difficult so...the obese patient where just getting into the belly is a much more strenuous activity and I’m having to put a lot more torque on instruments...and patients that have a lot of scar tissue or prior damage [are more work on me]” (Lines 261–265). Researchers observed high exertion with sustained grips and pinches on surgical instruments during the surgical procedure of a large patient with a history of prior surgeries.
The OB/GYN surgeon frequently rested both upper extremities on her patient during laparoscopy; rest breaks were a few seconds in duration. Prior to the end of the surgical procedure observed by the researchers, the RULA score for the OB/GYN surgeon was a seven, the highest score possible, defined as a need to assess and implement a change. Highest MSD risk to the body, as quantified by the RULA, included lower arm, neck, wrist twist, and trunk position. The OB/GYN surgeon exceeded the QuickDASH work module normative value of 8.81, showing disability of the upper extremities (Fig. 4). Although not a surgical procedure, the OB/GYN surgeon described vaginal delivery as “...physically demanding [because of] being in a certain position and having to use my hands and forearms in ways that make me very sore sometimes” (Lines 105–108).
For the OB/GYN surgeon, work outside of the OR included using technology to review patient charts and document operative procedures and office visits. Descriptions of this work revealed MSD risks of sustained upper extremity postures, repetitive digital flexion, and infrequent rest breaks. Her descriptions of the work also revealed that task demands were greater when using a laptop instead of a desktop computer. She preferred an external mouse for comfort and had difficulties using her dominant hand and forearm during documentation: “...well my laptop I would be on 8 hours, 3 full days a week and then after hours I try and get on a desktop because I find the mouse to be a lot more comfortable...I struggle with my dominant hand and forearm so [it helps] if I can get off the laptop” (Lines 162–164). MSD risks were not described but could be possible when the OB/GYN used other technology, depending on performance. She reported using tablets for documentation three days a week for 3 hours a day, and also used her cell phone during work. The OB/GYN surgeon used a documentation template and dictated 60–70% of her operative cases hands-free. After work hours she used a desktop computer, and estimated spending 10–15 hours weekly using technology when not at work.
The OB/GYN’s work schedule influenced MSD risk depending on the intensity, volume, and types of scheduled surgical and emergent procedures she completed on a weekly basis. She described a typical weekly operative schedule as 3 or 4 elective hysterectomies that also included variability because of unpredictable vaginal deliveries, Caeserean sections, emergency laparoscopy for ectopic pregnancy, and dilation and curettage (D and C) for miscarriage. In regards to annual schedule, task demands in the OR increased during the last quarter of the year because of greater numbers of scheduled elective surgeries which reduced rest and increased demands on the body. MSD risk also was influenced by fulfilling on call hours as she completed deliveries and emergent procedures, as well as documentation using technology. These risks included lack of rest, repetition, high exertion, and awkward postures, depending on the circumstances. When asked about fulfilling on call hours she described: “I am on call one night a week and every 6th weekend...and every other week those calls are in house [in hospital] ... from 5 p.m. to 7 a.m ... .” (Lines 66–68). Time use while on call varied: “...we may get woken up to...see a patient or go take care of something” [, answer] pages, sleep is very broke... [, and] there are certain nights where I just get a lot of charting done” (Lines 72–74, 85).
The OB/GYN surgeon shared that she currently experienced MSD, and that task demands and rest influenced her symptoms. She described having received treatment for lateral epicondylitis of her dominant right upper extremity, indicating that work tasks exacerbated her symptoms. “[After the most demanding operative tasks, I will be hurting] in my right arm and neck and trapezius area” (Line 240). Work outside the OR also made her symptoms worse: “I can’t even say that it’s just surgery that aggravates it [my symptoms] because I feel like the computer stuff can aggravate it just as much” (Lines 189-190). She also described foot and leg pain, as well as, bunions that were “definitely more painful after standing for prolonged periods of time” (Lines 181-182). Additionally, the OB/GYN stated that her “neck pain is almost always on the right” (Lines 183-184). She reported that rest improved her symptoms: “... if I have a prolonged period of time off... at least two-three days then when I go back on Monday it’s much better” (Lines 188-189).
Beyond rest, strategies used by the OB/GYN to reduce her symptoms included attempting to use her nondominant hand and wearing quality shoes. Ergonomic changes to her office work area included use of mobile tables, but she described these “to be a little cumbersome and I haven’t really taken to using [those]” (Lines 166-167). Because she recognized reduced musculoskeletal discomfort in her upper extremities when she used a desktop computer during documentation or chart review, she avoided laptop, cell phone, or tablet, when possible. The OB/GYN surgeon described modifications outside of the OR that she hoped would reduce task demands as she recognized a “limited modification ability in the OR” so it was important to make changes outside the OR (Lines 257-258).
Risks for MSD in the OR were similar to those reported by other researchers. Similar to findings of Ruitenberg et al. [5] and Cavanaugh et al. [6] both surgeons in the current study showed MSD risk due to repetitive tasks, and dynamic and static postures. Additionally, both surgeons used tools that required wrist positions deviating from neutral position, shown by Yu et al. [25] to increase risk for MSD. Consistent with Craven et al. [29] and Batham and Yasobant [12], surgeons also worked with high exertion due to patient size, type of procedure, and number of cases scheduled under time-frames. Similar to Maciel et al. [28] both surgeons attempted to reposition themselves during surgery to reduce awkward postures when able. The RULA confirmed MSD risk during operative procedures in the current study, consistent with Craven et al. [29], however highest scores were obtained before procedures were finished. This finding suggests alternate or additional instruments are needed to measure MSD risk for orthopedic and OB/GYN surgeons in the OR.
In contrast to Maciel et al. [28], neither surgeon intentionally scheduled rest breaks during or between cases to reduce MSD risk, although brief opportunities to correct postures were observed during delays. Gutierrez-Diez et al. [45] recommended that breaks should be up to 5 min for every 2 hours of surgical intervention, however it is unclear if the surgeons in the current study would be able to include these scheduled breaks. Both surgeons rested upper extremities on patients during procedures, a finding not reported in the literature. Although surgeons rested upper extremities, it is unclear if they were aware that this strategy could be a method of achieving rest breaks during operative procedures. Lack of rest breaks during physically strenuous work have been shown to lead to neck and arm pain, symptoms that were reported by both surgeons and findings that are in accordance with Ruitenburg et al. [5]. Moreover, the OB/GYN surgeon in the current study stated that rest made her symptoms decrease, supporting the recommendation for regular rest breaks described by Maciel et al. [28].
Patient size and type of procedure were examples of increased physical exertion required of surgeons in the current study. Franasiak et al. [10] found a positive relationship between BMI of the patient and physical strain reported by surgeons who performed laparoscopic procedures. It is possible that the orthopedic surgeon in this study frequently operated on a patient who was overweight or obese during TKA and THA procedures, as Suleiman et al. [46] found that 90% and 77% of patients with TKA and THA, respectively, were overweight or obese. The OB/GYN in the current study described that performing vaginal delivery produced the most musculoskeletal symptoms because the positioning required her to use her upper body in sustained postures with high exertion. Although researchers have reported MSD risk factors for OB/GYNs during laparoscopic procedures, risk factors resulting from vaginal deliveries have not been reported [29].
Both surgeons in the current study demonstrated similar MSD risks of awkward and sustained postures, and repetition during work outside the OR as in the OR, a finding not reported in the literature. More work hours were spent outside the OR with greater flexibility for reducing MSD risk by making modifications in task performance and to the environment. Opportunities for modifications outside of the OR included improving posture to neutral positions by altering heights of work surfaces or moving closer to patients, and reducing loads on upper extremities during patient examinations. In addition, the orthopedic surgeon could use a more neutral stance with reduced head and neck flexion during use of the computer. It could have been that the OB/GYN surgeon’s use of mobile tables during patient examinations would reduce MSD risk, but this could not be confirmed. Sleep postures and documentation during on call work for the OB/GYN could have also produced MSD risk but these were not observed. The identification of repetitive movements and awkward and sustained postures during work outside of the OR in the current study provides additional depth to MSD risk factor research for surgeons, and is similar to findings by Zeb et al. [4] for other professions including surgeons, doctors, and dentists. Because surgeons had more control over, and more opportunities for modifications outside of the OR, these modifications are even more important for decreasing the cumulative impact of MSD risk factors [15].
Both surgeons occupied multiple roles outside of work that could increase MSD risk. Outside of work the orthopedic surgeon described occupations that had risks for MSD, including using vibratory tools for woodworking, lifting loads while caring for pets, and throwing a softball repetitively during volunteer activities. The OB/GYN lifted loads and used awkward and sustained postures during home management and care of pets outside of work. Reducing risks during these occupations would likely be more feasible and reduce the cumulative effect of MSD risk for both surgeons.
Data from the Centers for Disease Control indicated that among individuals with MSD conditions, activities of daily living (ADL) were self-reported as the most difficult to perform compared to other occupations [47]. This finding was similar to surgeons’ reports in the current study, as the orthopedic surgeon reported that his most difficult task was washing his back. Moreover, ADL and IADL participation could contribute to MSD symptoms, but could have been perceived by the surgeons in the current study to be work-related [47, 48]. A study by Sacouche et al. [48] indicated that hospital workers whose occupation of work entailed the IADL of home establishment (laundry) were affected by MSD with risk factors of repetitive movements, awkward postures, and exertion in IADLs, which could occur in the surgeons’ roles outside of work.
Researchers have not used the QuickDASH to measure upper extremity function in surgeons, yet both surgeons had disability greater than the normative value for the work module. Surgeons in the current study more often attributed MSD symptoms and decreased work performance to demands of work, however, roles and tasks outside of work also increased MSD risk.
The surgeons identified tasks that had potential to make them symptomatic or already had caused symptoms, but did not describe MSD risks, nor the value of reducing MSD risk, in all occupations. Similar to findings of Franasiak et al. [10], the surgeons within the current study showed initiative to reduce some risk factors for MSD, but these were few and limited to work tasks. Although one surgeon described making modifications to reduce risk factors for continuing work on the computer at home, it is unclear if the surgeon recognized this modification as a method that would also reduce risk factors for non-work. This lack of recognition is consistent with the literature, where researchers have not described modifications to reduce MSD risk during non-work tasks and tasks outside of the OR for surgeons. Similar to results of Miller et al. [7] it is possible the surgeons of the current study lacked the knowledge to reduce the MSD risk factors during work in the OR and outside the OR.
Limitations
Both surgeons showed additional MSD risks during surgical procedures after the highest RULA exposure level was achieved, demonstrating a ceiling effect for the RULA [31]. Rather than observe, researchers relied on surgeons’ self-reports of non-work activities, and a portion of work outside the OR to understand MSD risks. This could have produced inaccurate reports of MSD risk. Surgeons may have rated work performance on the QuickDASH based more on work in the OR, presenting a narrow view of work. Researchers conducted only one interview with each surgeon, limiting the opportunity to ask additional questions and obtain data. The case study design used in this study yielded a more comprehensive analysis of MSD risks for two surgeons, preventing generalization of the findings to other surgeons.
In the future, researchers who plan to study MSD risk for orthopedic and OB/GYN surgeons should replace or supplement the RULA in order to measure MSD risk more completely in the OR. Researchers should confirm that surgeons’ self-rating of work performance on the QuickDASH reflects work in and outside of the OR. Rather than rely on surgeons’ self-reports of MSD risks during work outside the OR, researchers should observe and quantify these risks. Likewise, researchers should observe occupational performance during home management, child care, leisure, and volunteer tasks to more accurately identify MSD risks outside of work. A comprehensive understanding of MSD risks provides a foundation for developing and implementing interventions to reduce risks for each surgeon based on unique occupational performance across contexts. Beyond MSD risk for surgeons, future research could also include identifying and quantifying MSD risks for other healthcare personnel in order to develop interventions at the organizational level to reduce MSD risks.
Conclusion
Researchers who have studied risk factors for MSD among surgeons have limited their data collection and analyses to work in the OR or have concluded that work tasks can explain MSD risk. Likewise, researchers have attributed MSD exacerbation to surgeons’ lack of modifying work performance in the OR. The findings of this study indicate that MSD risks occur during all aspects of work for surgeons and during occupations outside of work, filling a gap in the literature. Identifying risk factors across all occupations and all contexts yields a more comprehensive understanding of MSD risk.
Conflict of interest
None to report.
Footnotes
Appendix
Interview of Surgeons 1. Please describe the following: your age number of years working as a surgeon number of hours working weekly performing surgery number of hours working weekly beyond performing surgery Describe your roles beyond the role of surgeon. (For example, parent, spouse, friend, colleague, caregiver). Describe the musculoskeletal demands, if any, that are associated with these roles. Describe your activities during a typical non-work day. (For example, leisure, rest, sports, home maintenance). How much time do you spend on these activities? Describe what you most and least enjoy doing when you aren’t at work, and why. Do you perform non-work tasks that are similar to tasks performed during surgery? If yes, please describe. (For example, prolonged standing, fine motor, close visual work, awkward and/or sustained positions, use of tools.) Do these tasks produce musculoskeletal symptoms? If yes, please describe. Describe how non-work activities are different or the same now compared to 5 years ago. Tell us how work activities are different or the same now compared to 5 years ago. What kind of technology do you use at work when not completing surgical procedures? (For example, cell phone, laptop, tablet). How often and for how long do you use this technology? What kind of technology do you use when not at work? (For example, cell phone, laptop, tablet). How often and for how long do you use this technology? Do you currently have musculoskeletal symptoms? If yes, describe location and symptoms. What makes your symptoms better or worse? Describe your surgery schedule. (For example, how many and what types of surgeries are scheduled weekly? How many and what types of surgeries do you perform when on call?) Describe what you believe is most demanding on your body as a result of performing surgical procedures. Are there surgical procedures that are more or less demanding on your body than others? If yes, please describe. Describe what you believe is most demanding on your body as a result of non-work activities.
Acknowledgments
Authors thank fellow researchers Alex Baird, Hailey Brown, Samantha Farmer, Morgan Rhodes, and Annette Zajac for their contributions to the data collection and analysis, and to the writing of the manuscript draft. Researchers also thank Rachel Hummel, MOT, OTR for identifying the topic for research for the current study.