
Abstract
BACKGROUND:
For maternal and infant benefits, cradle, cross-cradle and football hold positions have been recommended and widely utilized by mothers during breastfeeding (BF) tasks. There is paucity of data on the biomechanical costs of these BF positions.
OBJECTIVE:
This study evaluated the trunk lean angles and electromyographic (EMG) activities of the trunk muscles during these BF positions.
METHODS:
In this experimental study, 25 nulliparous females carried a 6-kg weighing infant, while simulating BF tasks in each of the three BF hold positions for five minutes respectively. During each task, forward and lateral trunk lean angles were measured with a single inclinometer. Activities of the right and left erector spinae (ES) and external oblique (EO) muscles were also measured via surface electromyography. One-way analysis of variance was used to analyze data at a significance level of 0.05.
RESULTS:
Cross-cradle position resulted in significantly higher anterior trunk lean and right ES and EO muscle activities. Conversely, cradle position significantly elicited highest activities in the left ES and EO muscles. Left trunk lean angles were highest during the football position.
CONCLUSION:
Football BF position may pose less risk of BF-related musculoskeletal disorders in nursing mothers, as compared to the cradle and cross-cradle BF positions.
Introduction
Nursing an infant is physically demanding and may pose significant challenges on the mother [1, 2]. Breastfeeding (BF) is a universal practice and an integral part of natural childcare processes with numerous biological and emotional influences on maternal and infant health [3–5]. To maximize its benefits, World Health Organization [6] recommends two years BF including exclusive BF for the first 6 months postpartum and more than 8 times BF per day in the first 3 months of an infant’s life. Regardless of its outstanding benefits, BF poses remarkable energetic cost [7, 8] and physical stress [5] on the mother.
Nipple discomfort [9, 10], reduced bone mineral density [11] and musculoskeletal pain [1, 12–16] are among the common BF-related physical challenges experienced by mothers. During the postpartum period, nipple discomfort is commonly attributed to suboptimal positioning and attachment of the infant [10] while reduced bone mineral density has been associated with postpartum hormonal changes, inadequate dietary calcium and vitamin D intake, changes in physical activity, increased number of pregnancies, and duration and frequency of lactation [11]. In essence, nipple discomfort as well as musculoskeletal pain has been generally associated with inappropriate breastfeeding mechanics.
Breastfeeding mechanics, including latching (attachment to the breast during breastfeeding) and positioning are considered important for successful and effective breastfeeding [17, 18], prevention of breastfeeding problems [19–21] and increased maternal compliance with BF recommendations [22]. Consequentially, proper latch and position are recommended for maximum infant and maternal benefits of BF practices [23]. Recommended BF positions include cradle (Fig. 1), cross-cradle (Fig. 2), football (Fig. 3) and side-lying positions [24–28]. The first three positions are performed in upright sitting postures and have been widely utilized in various populations [13, 15].Despite reported maternal compliance in the utilization of these BF positions, prevalence of breastfeeding-related musculoskeletal pain has been identified in nursing mothers [13–15, 29]. BF-related low back, neck, shoulder and thigh pains were reported among lactating mothers in Thailand [13, 14]. In a Nigerian-based study [15], nursing mothers reported BF position-related musculoskeletal pains across various body segments (back, neck and upper limb joints), with the neck and shoulder identified as the commonest affected body regions. Despite these complaints, the aforementioned BF positions are still regarded as ergonomically suitable positions for mothers. Irrespective of the reported benefits of these recommended BF positions, their biomechanical costs and musculoskeletal implications on the mother have not been studied. As a result, guidelines relative to the roles of these BF positions in the occurrence and/or exacerbation of BF-related musculoskeletal disorders have not yet been established. This study therefore aims at evaluating the trunk lean angles and electromyographic (EMG) activities of the trunk muscles in response to the cradle, cross-cradle and football BF positions.

Cradle hold.

Cross-cradle hold.

Football hold.
This was a randomized crossover experimental study with repeated measures design. This study was approved by by the University of Nigeria health research ethics committee and was conducted in the kinesiology laboratory of the Department of Medical Rehabilitation, University of Nigeria, Enugu, Nigeria.
Participants
A preliminary power analysis showed that a sample size of twenty (20) participants will be needed for the analysis of variance at degree of freedom (dfb)=1, to achieve 96% (0.96) power with a moderate to large effect size of 0.60 at an alpha level of 0.05 [30].Thus, 20 apparently healthy nulliparous females who were conveniently recruited from the undergraduate hostels of the University of Nigeria, Enugu, participated in this study. Participants were eligible for the study based on the criteria that they were (i) within the age range of 18–35 years in order to reduce the potential confounding effect of age on musculoskeletal assessments (ii) right handed (iii) had no previous history of upper limb and/or spinal disorders and (iv) had never breastfed an infant. Women with BF experiences were excluded from this study in order to eliminate the cofounding factor of survivor effect, which has been found to decrease the observed association between symptomatic disorders and physically demanding tasks [31]. All the participants gave written informed consents prior to enrollment into the study Participants were recruited between April – June, 2017.

Participant flow chart.
Preparatory phase
On enrollment, participants were familiarized with the experimental procedures through verbal explanations and pictorial demonstrations of the three breastfeeding hold positions until they were satisfactorily orientated. In order to eliminate fatigue and order effects during the experimental procedures, the researchers grouped the three trials (A, B and C) into different sequences which were labeled and put in a ballot box. Each participant randomly picked a paper from the ballot box and this determined the sequence of the experimental process (chart 1). For instance, if CAB is picked, that meant the participant will perform the trials in such order that C (FB hold) comes first, then A (C1 hold) and B (C2 hold). The skin overlying both parts of the external oblique (EO) and thoracic erector spinae (ES) muscles were shaved and wiped with alcohol swabs. These two muscles represented the lateral trunk flexors and extensors, respectively, and are ideal for surface electromyographic analysis. With an inter-electrode distance of 1 cm, pairs of silver- silver chloride surface electrodes were placed on the skin overlying the ES (5 cm lateral to the T9 spinous process) (Fig. 4) and EO (15 cm from the umbilicus) (Fig. 5) muscles [32].
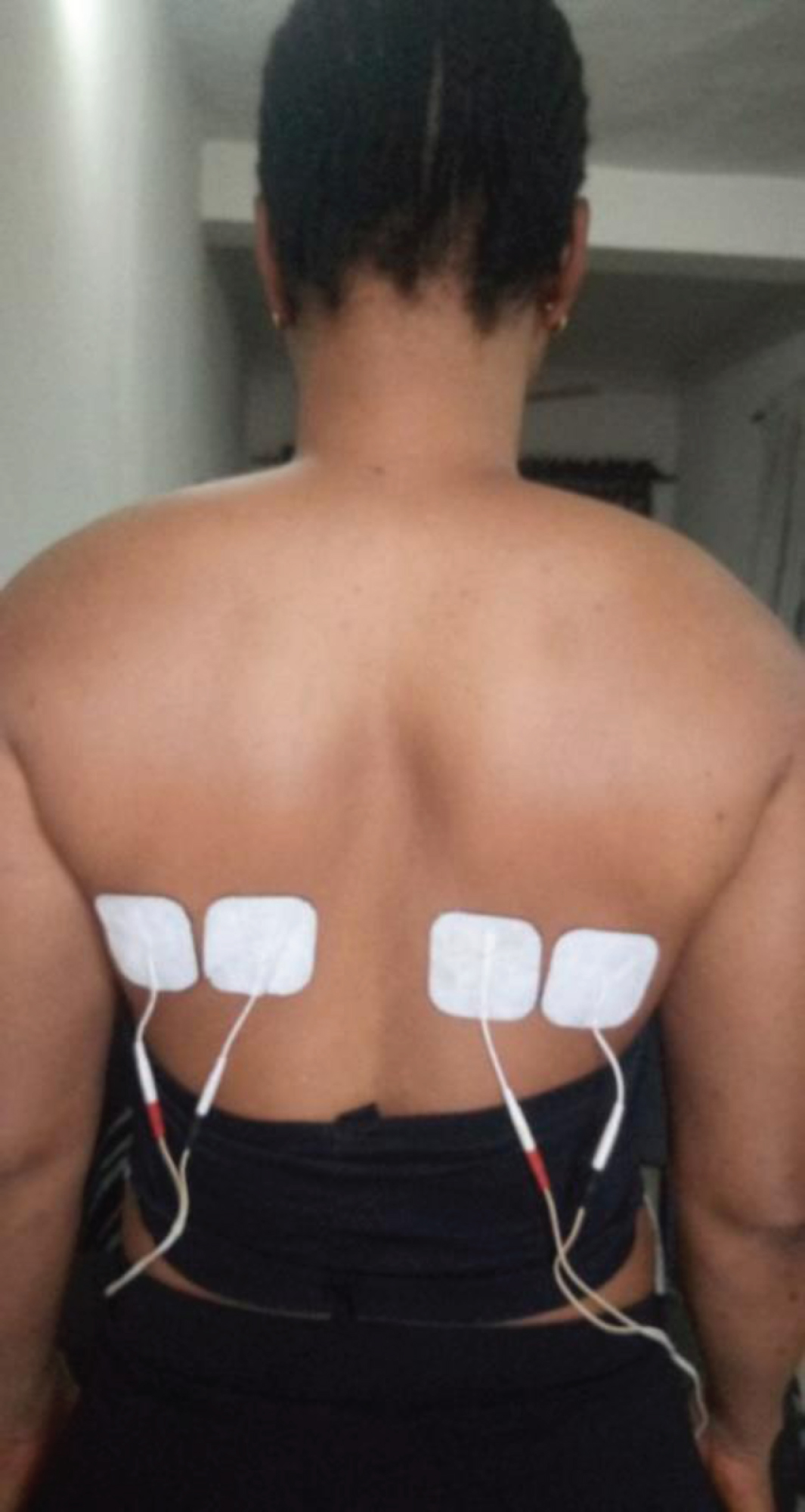
Electrode placement (right and left erector spinae muscles).
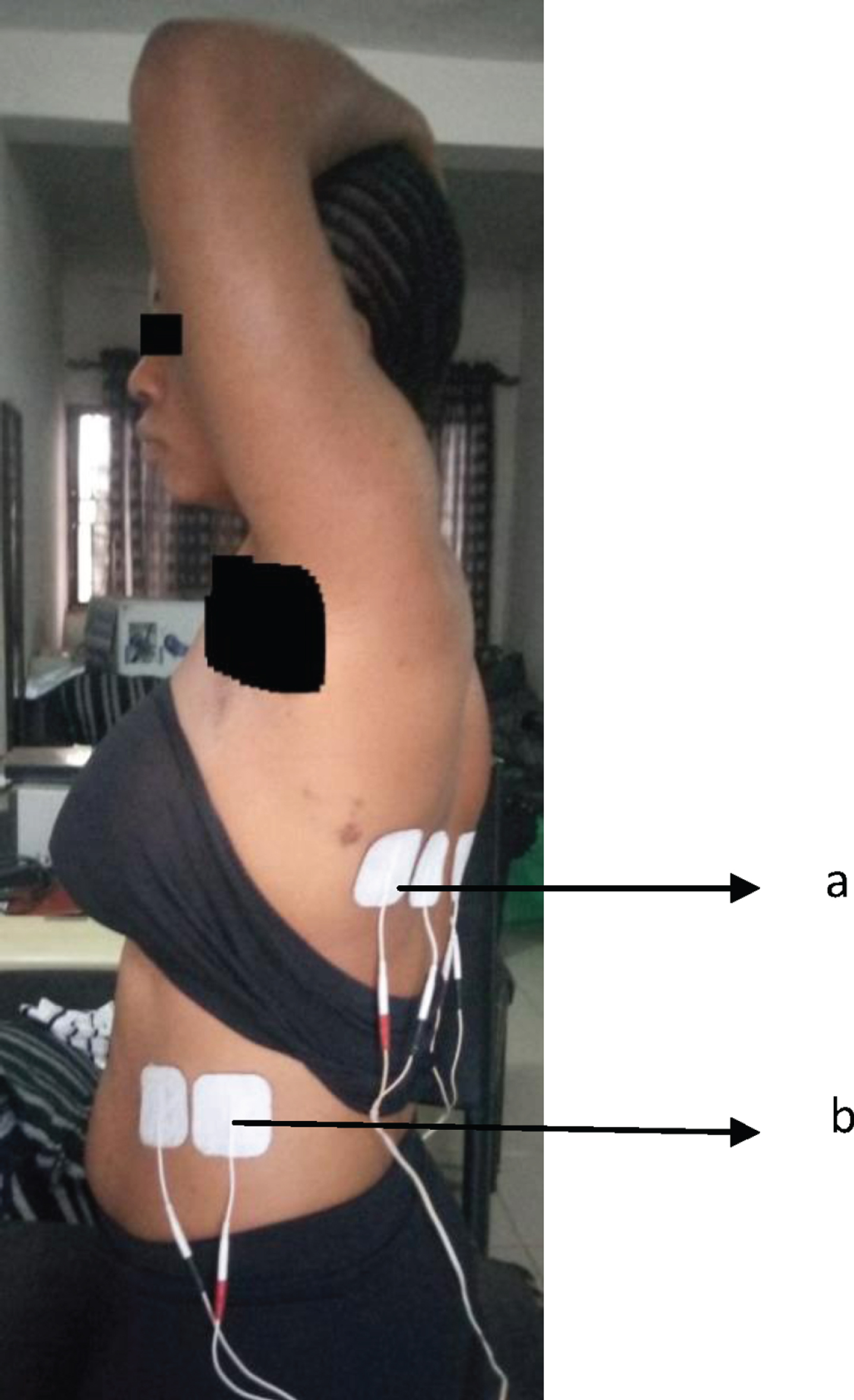
Electrode placement (a- left erector spinae muscles; b – left external oblique muscle).
Participants completed two sets of 3-min maximum voluntary contraction (MVC) tests for the right and left parts of each of the thoracic ES and EO muscles, with a 2-min rest period between trials. For the ES muscle, trunk extension from a prone lying position was manually resisted while trunk lateral flexion from a side lying position was resisted manually to test the EO muscles [33].
Experimental protocols
In a relaxed supported sitting position, baseline EMG activities were recorded from the ES and EO muscles. Experimental orders were randomized by simple balloting so as to eliminate order and fatigue effects. For each experiment, participants sat upright on a chair with back support, hips and knees flexed at 90°, hips slightly abducted and feet supported on a low stool. The experiments consist of three trials, including:
2.2.3.1. Trial A: Cradle hold (C1).
A 6-kg simulated male infant (Jimmy) was positioned in right side lying (head towards participant’s left side) on a supporting pillow placed on the participant’s thigh. Jimmy’s head was supported in the participant’s left elbow with her (participant) left palm placed on his buttocks. Grasping the left breast with the left hand, the participant directs her nipples towards Jimmy’s mouth while maintaining eye contact with him (Fig 1).
2.2.3.2. Trial B: Cross-cradle hold (C2).
Maintaining similar starting positions as in C1, participant’s right hand supported Jimmy’s head while the left hand was used to grasp and direct the left breast into Jimmy’s mouth (Fig 2).
2.2.3.3Trial C: Football hold (FB).
While adopting an analogous sitting position (as in C1 and C2 holds), the participant tilted towards her right with a resultant space between the left border of her trunk and the left arm support of the chair. In the space provided, Jimmy was placed in supine lying with his lower limbs adequately supported on a pillow placed on the participant’s left thigh. Participant’s left hand served as additional support to Jimmy’s head while she leaned towards her left breast which was grasped by the right hand and directed towards Jimmy’s lips (Fig. 3).
Each BF hold trial was maintained for 5 mins with a 30-min rest period between trials.
Inclinometer measurements
This was used to measure the trunk lean angles. For the antero-posterior measurements, the middle of the base of a universal inclinometer (model #19UI) was placed vertically over the spinous process of the second thoracic (T2) vertebrae, ensuring that the arm was at the zero point while participant was in a relaxed sitting position. On assumption of each BF hold position, the degrees of forward and posterior trunk lean were read off and recorded from the inclinometer.
Participants were then asked to return to the initial relaxed sitting position while inclinometer was re-positioned horizontally on the T2 spinous process. The participant then re-adopts the BF hold position, and the degrees of lateral trunk lean were measured and recorded from the inclinometer.
At the beginning of each BF trial, each of the specified trunk angles was measured twice and the average of the two values recorded for final analysis.
Electromyographic measurements
EMG signals were simultaneously recorded from both parts of the ES and EO muscles during each trial and were sent to a Myoplus2 system (Neurotrac System, Verity Medicals, Hampshire, UK), which amplified and sampled the EMG inputs at 1000 Hz. Using a Neurotrac software (version 5.0.117). The average EMG values were expressed as percentages of the MVC values prior to the statistical analyses.
Data analysis
Descriptive statistics of mean, standard deviation, frequency and percentage were used to summarize data. Subsequent to normality tests (Kolmogorov-Smirnov and Shapiro-Wilk tests) which confirmed that the data for most variables were normally distributed (p < 0.05) with few outliers, inferential statistics of one-way repeated measures analysis of variance (ANOVA) with Bonferroni post hoc analysis was used to test for statistical differences across trials. Alpha level was set at 0.05 and SPSS version 20.0 (SPSS, Chicago, IL, USA) was used for the statistical analyses.
Results
The general characteristics of the participants are presented on Table 1. Table 2 shows comparisons of the antero-posterior trunk components (antero-posterior lean angles and muscle activities of the erector spinae) across baseline and the three BF holds. Posterior trunk lean was absent in all the trials. There were significant (p < 0.05) differences in the anterior trunk lean angles and EMG activities of the erector spinae muscles across the BF hold positions.
General characteristics of the participants (n = 20)
General characteristics of the participants (n = 20)
Trunk antero-posterior lean angles and normalized electromyographic activities of the erector spinae muscles (Antero-posterior components)
*Indicates significance at p < 0.05.
Comparisons of the lateral trunk components (lateral lean angles and muscle activities of the external oblique) across baseline and the three BF holds are presented on Table 3. The results revealed significant (p < 0.05) differences in the right and left lateral trunk lean angles and EMG activities of both external oblique muscles across the BF hold positions.
Trunk lateral lean angles and normalized electromyographic activities of the external oblique muscles (Lateral components)
*Indicates significance at p < 0.05.
The Bonferroni post hoc results showing within subject comparisons of trunk lean angles and EMG activities of the trunk muscles across the three selected breastfeeding positions are presented on Table 4. Despite the marginal differences in the mean values of the study variables across the three BF positions, the statistically significant differences specifically existed in the forward trunk lean angles, RT EO and RT ES values of the C2 and C1 holds. Other within-subject comparisons did not reveal significant differences between the BF positions.
Bonferroni post hoc analysis showing within subject comparison values of trunk lean angles and EMG activities of the selected trunk muscles across the three selected breastfeeding positions (N = 20)
*Indicates significance at p = 0.05, RT = right, LT = left, ES = erector spinae, EO = external oblique. Values are presented as mean difference (p-value).
Trunk lean angles and electromyographic activities of the trunk muscles in response to cradle, cross-cradle and football BF positions were evaluated in this study. The main finding is that BF positions have differential effects on spinal angles and activities of the trunk muscles.
Compared to C1 and FB holds, the C2 hold elicited the highest anterior trunk lean angle and muscle activities in the right ES and EO muscles although the differences were exclusively significant between the latter and C1 hold positions. C2 position is characterized by supporting the infant with the upper limb contralateral to the side where the infant is positioned (i.e. the right upper limb in this study) while the ipsilateral upper limb supports the nursing breast. This maneuver requires increased trunk flexion to reach out fully and firmly support the infant’s buttocks or trunk. This may explain for the higher anterior trunk lean angle, as compared to the cradle and football positions. Tyler et al. [34] reported that arm reaching movements performed in sitting resulted in trunk torque flexion movements. Previous studies have associated upper limb reaching tasks with simultaneous trunk motions [34–36]. These simultaneous trunk motions are typically attributed to static or dynamic postural disturbances in response to voluntary movements [35, 37–39]. Static disturbances result from changes in gravitational torques, locations of the body segments, centre of mass and muscle activities to enable gravitational equilibrium while dynamic disturbances are sequel to the interactive effect of various body segment motions and require muscle activity for adequate counteraction-related destabilizing forces [34]. Nevertheless, C2 hold, similar to other BF holds, is predominantly characterized by static rather than dynamic postural disturbances. The effects of these postural changes inherent of the C2 hold is evident from the results of the present study which showed that reaching movement of the right upper limb during the this BF position was associated with increased activities in the right trunk muscles, as compared to the other BF positions. Logically, it may be suggested that in the same vein, a right cross-cradle BF position involving left upper limb reaching movement may possibly result in associated trunk motion with increased activities in the ipsilateral (left) trunk muscles.
These associated trunk muscle activities were also evident during the cradle position which elicited increased activities in the left trunk muscles. The left cradle position adopted in this study required a reaching movement of the left upper limb to achieve support of the infant. However, the cradle position elicited lesser trunk lean angles, compared to the cross-cradle position. Despite the fact that both BF positions relatively involved reaching movements of the upper limbs, the contralateral upper limb which performed the reaching movement in the cross-cradle position covered a longer linear distance in reaching the infant’s buttocks, as compared to the left upper limb in the cradle hold.
These findings imply that cradle and cross-cradle positions required increased trunk muscle activities to elicit postural control in response to the reaching movements of the respective upper limbs which offered infant support. Prolonged adoption of these two BF positions may predispose nursing mothers to breastfeeding-related musculoskeletal disorders as a result of postural imbalances and associated muscle fatigue in the trunk muscles. Prolonged static work postures, particularly in awkward patterns, are among major factors implicated in the development of Work-related musculoskeletal disorders [40]. Safe maternal practices during utilization of these BF positions are necessary as studies have shown high preferences for the cradle and cross-cradle positions [15, 29]. It is thus recommended that mothers should alternate the adoption of right and left-sided holds while utilizing each of the cradle and cross-cradle positions. Also alternating between the cradle and cross-cradle positions between and within BF sessions may also be a strategy to reduce the risk of BF-related musculoskeletal disorders.
The present study revealed that the football position significantly resulted in increased left lateral trunk lean angle, compared to the cradle and cross-cradle positions. Although not statistically significant across the groups, this finding may be attributed to the lateral trunk motion associated with the movement of the contralateral upper limb as it supports the nursing breast (the left breast in this study) while directing it into the infant’s mouth. However, it was inferred from the results that the left trunk lean associated with the FB position seemed rather insufficient to elicit increased activities in the left trunk muscles (particularly the external obliques). Rather, the external obliques showed significantly decreased activities during the FB position, as compared to the cradle and cradle positions. Biomechanically, this trend in the study findings is controversial and may require further analysis of these biomechanical parameters during BF tasks to explain for this discrepancy. This discrepancy in the present study’s findings may be attributed to the fact that trunk lean angles and EMG activities of the trunk muscles were not measured simultaneously for better outcomes of the relationship(s) among these variables during BF. Further studies should however involve simultaneous and dynamic biomechanical analysis, rather than static measurements solely.
Conclusion
The cradle, cross-cradle and football BF positions result in biomechanical and postural alterations of the trunk which may predispose women to BF-related musculoskeletal injuries. However, the football position is the most biomechanically efficient, as compared to the cradle and cross-cradle positions. Alternating BF positions should be considered in addition to postural training to emphasize appropriate back care principles during BF tasks. Further studies are required for evaluation of specific musculoskeletal injuries that may be associated with each Bf position relative to relevant maternal characteristics.
Conflict of interest
None to report.
Footnotes
Acknowledgment
We appreciate all the study participants for their consent and participation in this study.