
Abstract
OBJECTIVES:
To investigate the effect of wearing hard hats on the lower cervical and upper thoracic region using surface electromyography (sEMG) and possible link to work-related musculoskeletal disorder (WRMSD).
METHODS:
Twenty study subjects wore sEMG sensors placed on the upper trapezius muscle on their dominant side to assess muscle activity while wearing different hard hats. Study subjects were asked to don six different hard hats and assume varied neck postures. A repeated-measures design was used to analyze the results for difference and similarities in muscle activity.
RESULTS:
There was a small, significant effect of wearing a hard hat on muscle loading in the upper trapezius (p = 0.038). Post-hoc analyses revealed the only statistically significant difference was between wearing no hard hat at all and wearing head protection (without accessories) in the flexed posture (p = 0.006).
CONCLUSION:
The results demonstrated that there was little difference in lower cervical and upper thoracic muscle activity while donning hard hat and assuming various neck postures. Wearing a sample of commonly used hard hats in this study does not appear to substantially increase muscle activity that would cause fatigue in the lower cervical and upper thoracic region among young, healthy volunteer subjects.
Introduction
The global burden of neck pain ranks fourth in the cause of disability-adjusted life years [1]. Investigators estimated the approximately 300 million people suffered neck pain world-wide in 2015. Data comparing 2005 to 2015 estimates of neck pain revealed that the prevalence had increased 21% over the period studied [1]. Neck and upper back pain are ubiquitous problem with an annual prevalence among workers ranging from 27% in Norway to 48% in Canada [2]. The point-prevalence of neck pain can range from 5% to 51% at any point in time depending on the worker population and industry [2]. This high prevalence for neck (cervical) and upper back (thoracic) (CT) back pain can be attributed to several factors including the use of personal protective equipment including hard hats (head protection) and other head-donned equipment [3]. The added weight to the head potentially causes increased muscle activity, strain and resulting fatigue of the CT musculature. When the cranium is loaded with additionally beyond usual weight of the head (4.5 to 5 kg), the supporting musculature may react with increased activity to manage the added load. Furthermore, neck posture can greatly influence muscle activity needed to support the load away from the neutral position. Postural deviation from neutral be strenuous and neck muscles can become fatigued, causing misalignment of the spine and an increased risk of cervical CT work-related musculoskeletal disorders (WMSDs) [4].
The effect of head protection weight on the neck has been studied in military settings due to heavy equipment commonly attached to the helmets for example, those worn by military helicopter personnel [3–5]. Researchers found a 70% prevalence of neck pain among Royal Canadian Air Force helicopter aircrew [5]. To offset the added weight anterior to the gravity line due to attached optics, a counterbalance weight is often applied to the posterior of the helmet [3–5]. Evaluation of three helmet designs with specialized optics were evaluated using EMG sensors. Investigators confirmed significant increases in muscle activity in the cervical thoracic region when donning helmets and assuming various postures and performing vigilance tasks [5]. The use of such head-worn equipment changes the head’s center of gravity, compensatory muscle activity and postural alteration from neutral. Biomechanical deviations from neutral potentially result in fatigue and WMSD risk [3–5]. However, the head protection weights experienced by military helicopter personnel are generally heavier than would be seen in other industries and represent a small proportion of workers wearing helmets.
Hard hats are commonly worn in construction industries and other sectors where overhead hazards are present. There are an estimated 7.2 million construction workers with approximately 263,000 job opening at US construction sites in the US [6]. In Europe, the construction industry directly employs an estimated 11 million workers [7]. Hard hats are often outfitted with additional equipment related to the work, such as headlamps, hearing protectors, or visors. While these hard hat accessories may offer safety and comfort benefits, they also contribute to the overall weight of the head protection. No studies were found in the literature that had investigated lighter weight and more commonly worn head protection in the form of hard hats with and without accessories and their potential contribution to the development of WMSDs of the CT region. The aim of this study was to examine the muscle activity in response to donning three different hard hats and moving head into two positions away from neutral to assess potential contribution to development of WRMSDs.
Methods
Subjects
Twenty college students were recruited without regard to age or gender using an Institutional Review Board approved script. Before testing, all 20 participants were confirmed to be in good health with no prior neck injury or back pain present. Six subjects were later excluded due to issues with their EMG data. Subjects provided informed consent prior to the start of the study. Each subject was given a small, nominal payment for participation.
Experimental design
A repeated measures design was used to assess the effect of hard hat weight and neck posture on muscle activity in the CT trapezius. Muscle loading was assessed using sEMG while wearing three different head protection weights (none, head protection only, and head protection with accessories) at two different neck postures (neutral and 20 degree flexion). Each subject was assessed under each of the six head protection weight and neck posture conditions.
Measurement procedures
Participants were weighed to estimate head and neck weight as 7.9% of their total body weight, as originally described by Dempster in 1955 [8]. A Delsys Trigno© Wireless sEMG system (Delsys, USA) was used to measure muscle loading in the upper trapezius muscles of the CT region. One Trigno Mini sensor was applied to the surface of the skin above the upper trapezius muscle on the dominant hand side of the participant. The sensor placement was oriented parallel to the direction of the upper muscle fibers of the trapezius and placed approximately three to five centimeters (depending on the size of the subject) distal and superior from the C7 spinous process. A reference electrode was placed over the clavicle on the same side of the body. The sEMG electrodes were worn throughout the duration of the experiment. Subjects were prepared for the sensor attachment using an alcohol pad to clean the site and a safety razor was used, when necessary, to remove excessive hair that could prevent the sensor electrode from contacting the skin.
A hook providing a point of resistance was fastened to a stationary setup on a table. The hook setup was height adjustable +/–15 cm from the table top. A sling was attached to the end of the hook via a steel cable. The sling was fashioned from a hard hat suspension, which was fully adjustable to fit tightly and provide support below the occipital bone during neck extension. Participants were seated in front of the stationary hook set up in a height adjustable chair. The heights were adjusted for each participant so that they would have a flexed, chin-to-chest posture while wearing the sling that was attached to the hook. The hook setup, sling, and chair system provided resistance and isolation for isometric neck extension.
Subjects were asked to extend their neck as hard as possible against the resistance of the hook system for five seconds, three times with a five second rest period in between extensions. Subjects were instructed to relax in between each extension. The sEMG signal recorded during this process provided the subjects’ maximum voluntary contraction (MVC) reference value for sEMG signal normalization.
Participants were then placed in each of the six head protection weight and neck posture conditions. Twenty-degree neck flexion was determined via a goniometer. Subjects were instructed to sit naturally in an adjustable chair. The center of the goniometer was aligned over the external auditory meatus. The proximal arm of the goniometer was perpendicular to the ground while the distal arm was aligned with the alar rim of the nose. Subjects were instructed to lower their chin until the distal arm reached the appropriate 20 degree flexion position on the goniometer. This positioning occurred once for each 20 degree of flexion position for all subjects. Once a subject was situated in each condition, a five second sEMG measure was taken, until the subject had been measured in each of the six head protection weight and neck posture condition. All subjects received all conditions in a random order to minimize ordering effects, such as learning or fatigue.
The head protection used in this study were four-point ratchet suspension hard hats (3M, USA), which weighed 340 grams. The weighted head protection was equipped with hearing protection in the form of earmuffs, a face shield bracket, a personal cooling unit, and a LED headlamp. The muffs used were Peltor X-Series Cap-Mounted earmuffs (3 M, USA) with a total weighing 226 grams. The face shield was a Safety Shield (MCR, USA) with an aluminum bracket. The total weight of this shield bracket was 158 grams. The headlamp was a Headlamp model XML L2 (Boruit, China) which weighed 430 grams. The personal air-cooling unit was Workflow Hardhat Cooling System (Workflow Industrial Products, USA) which weighed 907 grams. The weight of the entire weighted head protection was 2.06 kilograms. The weighted head protection provided a worst-case scenario in terms of head protection weight for comparison with the much lighter head protection without accessories. Typical head protection accessory usage varies by industry and situation, but the total hard hat weight would not likely exceed that of our weighted head protection.
Data analysis
Data was processed and stored on a laboratory computer using Delsys EMG Works version 4.3 and Delsys EMG Analysis version 4.2.0.0, copyright Delsys Inc., Natick, MA, USA. Two members of the research team independently reviewed the raw sEMG signal from each subject’s MVC effort to determine whether the three maximal extensions were clearly distinguishable from the signal background noise. Six of the 20 subjects without three discernable and distinct efforts in the sEMG signal were excluded from further analysis in the study. This signal quality check ensured that each subject included in the analysis had a valid reference contraction for sEMG comparison of the different head protection weight and neck posture conditions.
The sEMG signal for each subject under each condition was normalized using the subject’s root-mean-squared MVC. This amplitude analysis provided the relative muscle loading of subjects under each condition in terms of a percent MVC. The mean percent MVC, measured in the five-second-measurement period for each subject, was recorded for each head protection weight and neck posture condition.
Statistical analyses of these data were performed using SAS software version 9.2, copyright, SAS Institute Inc., USA. Differences in mean muscle loading between the six head protection weight and neck posture conditions were analyzed using a repeated measures analysis of variance (ANOVA) model. Both head protection weight and neck posture were coded as within-subject variables, with no between subject variables included in the model. The null hypotheses for this analysis were: There was no significant effect of head protection weight on muscle loading in the upper trapezius. There was no significant effect of neck posture on muscle loading in the upper trapezius. There was no significant interaction between head protection weight and neck posture.
The assumption of sphericity was assessed using Mauchly’s Sphericity test. Because the assumption of sphericity was not fulfilled by the data nor following generally accepted transformations, the multivariate alternative Wilk’s lambda test was used instead. A post-hoc comparison of significant variables was accomplished using a Wilcoxon Signed-Rank test. The level of significance for each pair-wise comparison was adjusted to maintain a family-wise Type I error rate of 5% by using a Šidák correction according to the following formula: α (P–W) = 1–(1–0.05)1/m, where ‘α (P–W) ’ is the pair-wise level of significance and ‘m’ is the number of comparisons [9].
Results
A total of 20 subjects were recruited to participate in this study. Six of the original 20 subject’s data were removed, leaving 14 data sets remaining. Two members of the research team independently recommended the removal of the six subjects’ data sets after the MVC electromyograms failed to display three clearly discernable maximum muscle contractions. The remaining 14 subjects included in the study consisted of 7 female and 7 male subjects. The mean age of the 14 subjects was 24.4 years (range 21–33). Subjects average head and neck weight, estimated using 7.9% of their body weight, was 6.95 kgs (range 5.57–9.2) for males and 5.29 kgs (range 4.36–6.39) for females.
Head weight was increased by an average of 22.97% with the addition of the weighted head protection, which weighed 2.06 kilograms. With the addition of the hard hat only (340 grams), head weight increased by an average of 5.67%. A summary of the sample demographics is provided in Table 1.
Sample demographics
Sample demographics
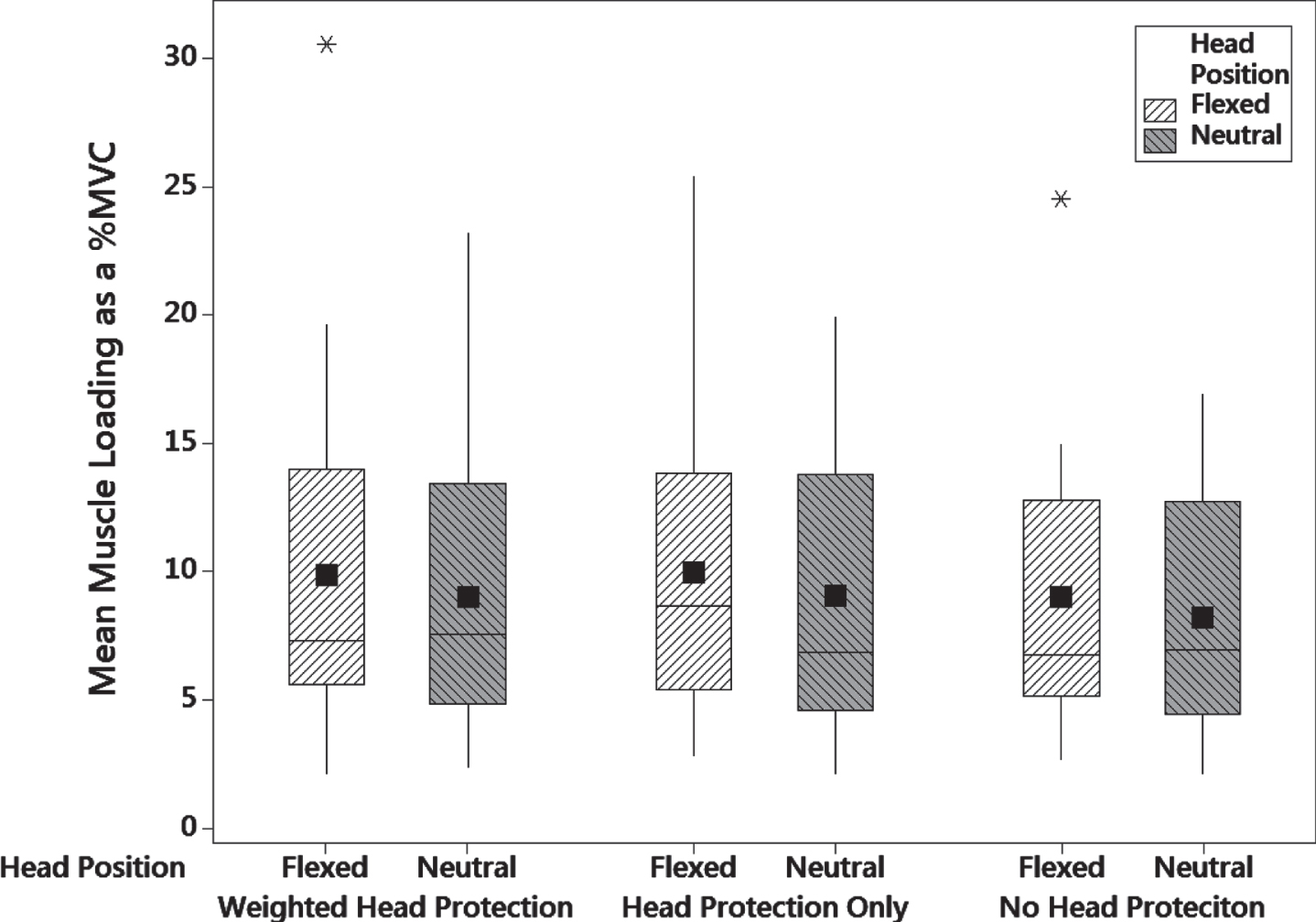
The mean percent MVC for the six head protection weights and neck posture combinations are provided in Table 2. A comparison of the subjects’ mean muscle loading measured under the six different head protection weight and neck posture conditions is provided in Fig. 1.
Mean muscle loading associated with different head protection weight and neck posture conditions
a% MVC is the percentage of maximum voluntary isometric muscle contraction.
% MVC of subject head protection weight and neck posture.
Because the assumption of sphereicity was not met for these data nor was sphereicity adequately improved by transformation, the non-parametric alternative Wilk’s Lambda multivariate test was performed. The effect of head protection weight on muscle loading in the upper trapezius was small but significant (Λ= 0.58, p = 0.038). The effect of neck posture on muscle loading was not statistically significant (Λ= 0.89, p = 0.167). The nonparametric Wilcoxon Signed-Rank test was used to compare the muscle loading associated with individual head protection weights and neck postures. Six conditions were compared, resulting in a pair-wise level of significance of α= 0.009. The only significant post-hoc difference at this level was the head protection only when compared the head weight only without head protection in the flexed posture (p = 0.006). The post-hoc comparison results are provided in Table 3. There was no significant interaction between the head protection weight and neck posture (p = 0.983).
Post-hoc comparisons for head protection weight and neck posture conditions
Post-hoc comparisons for head protection weight and neck posture conditions
aComparison was significant at the 0.009 pair-wise significance level using a Wilcoxon Signed-Rank test.
The mean percent MVC in the CT trapezius observed under each head protection weight and neck posture condition ranged from 8.23% to 9.99%, which was very close to the range reported by Thuresson and colleagues in a study of military helicopter personnel [2]. Another military study found up to a 29% increase in neck muscle activity when evaluating helicopter pilots in differing postures and performing vigilance tasks [5]. While Thuresson and colleagues observed a range of 7% to 10% MVC while subjects were placed in different helmet equipment and posture conditions [3]. Another study of muscle neck muscle activity of helicopter crews found sustained muscle activation around 10% MVC during actual flight missions [10]. This high level of agreement between the studies is interesting because the head protection weights employed in their experiments were heavier than the hard hat weights used in the present study. Our use of college students not accustomed to wearing head protection compared to experienced military personnel who regularly used head protection may explain this similar muscle activation among the participants in this study despite being exposed to a lighter weight. Additionally, the higher fitness level among military personnel may also have contributed to this finding.
The results of the hard hat weight and neck posture analysis in our study showed a small but significant effect of head protection on muscle activity in the CT trapezius. After performing a post-hoc analysis of the individual pair-wise differences between the six different head protection weight and neck posture combinations, it was determined that the only statistically significant difference was between wearing no head protection at all and wearing only the head protection (without accessories) in the flexed neck posture. The mean difference in percent MVC between these conditions in the flexed neck posture was only 0.96% (Table 3). In contrast, applying heavier head protection weight to the head has been shown in previous studies to cause a higher level of muscle activation in the CT upper trapezius [2, 11]. In both studies, subjects wore helmets equipped with night vision goggles (NVG) with and without counter weights (CW) [2, 11]. The authors found that there was significantly higher muscle activation in the upper neck when wearing the helmet with NVG with and without CW compared to wearing the helmet alone (p = 0.027 and p = 0.011, respectively) [3, 11].
Neck posture did not have a significant effect on muscle activity in the present study, which is also in contrast to previous reports. However, our study subjects maintained modest postural deviation for only five seconds and did not hold flexed position for an extended period as commonly seen in construction work and mining. Thuresson et al. and Dibblee et al. found that neck posture influenced muscle activation, particularly when the neck was in flexion and rotated [3, 5]. Muscle activation was significantly greater than neutral postures in the rotated position regardless of the amount of weight applied to the head [3]. Dibblee and colleagues positioned subjects into various postures with head and neck rotation and found that prone positioning without assisted support of head and helmet resulted in the highest muscle activity, the seated position yielded the lowest values [5]. One potential reason for the discrepancy between our results and those presented by Thuresson and colleagues was the inclusion of neck rotation [3]. Further, the head protection weight in our study ranged only from 340 grams to 2.06 kg, as compared to 1.45 to 2.52 kg used in the previous study [3].
Lastly, in prior studies performed on military helicopter personnel using NVG on head protection, the weight was situated on the front portion of the helmet. The placement of the NVG increases the overall helmet weight, as well as causing a forward shift in the head’s center of gravity in relation to the axis of the cervical spine [11]. In the present study, the weight placed onto the weighted head protection was relatively balanced and the load moments were not assessed. Had this weight been substantially heavier on any particular side, a higher level of muscle activation would likely have been required, especially in the flexed posture.
Study limitations
The findings of this study should be considered in light of several methodological and sample limitations. Subjects were limited to a small, convenience sample of college students ranging from 21 to 33 years of age. Additional demographic factors such as fitness level and experience wearing head protection were not considered. This study was a pilot study designed to estimate the effect size of head protection on muscle loading in the neck relevant to industries where hard hat usage is common. Given that the results were largely not statistically significant, this may in part be due to underpowered statistics and the effect sizes reported here can be used to inform future investigations. However, the absolute differences between hard hat weight and neck postures were quite modest and generally within 1% MVC.
In addition, only one muscle and one type of posture were assessed. Workers who wear hard hats must do so while in a wide variation of body and neck postures for short to extended periods of time. Industries such as construction and mining require workers to use multiple dynamic head positions and extreme neck movements while wearing hard hats. Furthermore, the only muscle examined in this study was the upper trapezius due to equipment and logistic limitations. Evaluation of additional para spinal CT muscles in a variety of neck postures would allow for a further understanding of the muscle loading associated with wearing head protection typically used in industry.
Subjects in the present study were not exposed to any additional ergonomic risk factors including whole body vibration (WBV), which can be commonly encountered in industries that use head protection. However, the presence of WBV may increase the risk of neck pain and development of WMSDs, although the association is less clear than between low back pain and WBV [12]. Further, working in a “twisted” position while being exposed to WBV has been associated with increased muscle load in the neck and shoulders [12]. The present study was limited to two neck postures, not including any sort of rotation or WBV. Postural deviation in flexion was modest at best. Ranges of motion greater than 20 degrees from neutral are likely to result in increased muscle fiber recruiting and overall activity. Thus, it would be inappropriate to discount the potential for head protection to increase WMSD risk in the presence of these additional risk factors.
Study strengths
A main strength of this study was the focus on hard hats typically worn by industrial workers. Further, employing the use of typical (head protection only) and worst-case (head protection loaded with a number of accessories) weights provides a range of results that should encompass the large variety actual head protection weights seen in industry, especially given the variety of hard hat and accessory configurations that are available to workers.
Another benefit of this study was the inclusion of both male and female participants. Prior studies involving military helmets were limited only to male participants. However, in industry today you will find both male and female workers. This is important because of the difference between male and females as it relates to ergonomic risk factors. Anthropometric and physiological factors may make women more prone to WSMDs in the work place [13]. When exposed to identical industrial work tasks, women as compared to men had higher muscle activation and WMSD risk levels [13].
Finally, the use of a repeated measures design was advantageous because it allowed for each subject to act as their own control. By designing the study to obviate the between-subjects variability inherent in ergonomic exposure measurements, the effect of different head protection and neck posture conditions was isolated. A typical ANOVA, for instance, would have required a much larger sample due to the inclusion of both between- and within-subject variability.
Conclusion
The aim of this study was to determine whether neck posture, hard hat weight, or both in combination could contribute to the development of WMSDs in the CT region. The results demonstrated that there was small difference in CT muscle activity under different head protection weight and neck posture conditions. Because there was little difference in muscle activity when head protection was applied to the head as compared to the head alone, in either posture, the evidence from this study does not support an increased risk of WMSDs associated with wearing commonly used head protection in similar conditions used in this study. Although there was a small, significant effect of hard hat weight, post-hoc analysis revealed that it was only due to a slight difference (less than 1% MVC) between the mean muscle activity with and without head protection in the flexed posture only.
Given that a worst-case scenario hard hat weight was applied to male and female subjects with little prior experience wearing head protection, the results of this study suggest that hard hats typically encountered in industry and worn by experienced workers would not likely increase muscle activation in the CT trapezius by a significant amount, on average. Further research is needed to determine if this holds under additional neck postures such as rotation and extension and in the presence of other ergonomic risk factors such as whole body vibration and/or sustained posture deviations common in industries where hard hats are donned.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This study was supported in part by support from the National Institute for Occupational Safety and Health Training Project Grant (grant no. TOH008630) and a Montana Tech internal grant (grant no. BDG026). The contents of this publication are solely the responsibility of the authors and do not represent official views of any funding organization or agency.