
Abstract
BACKGROUND:
The high stress culture and demands associated with long-haul truck driving place truckers at risk for mental health and sleep disorders, and thereby, increased risk for accidents, injuries, and fatality. Hours-of-service regulations have proven insufficient as a stand-alone intervention to protect the welfare of long-haul truckers, impacting those working in the industry and those sharing our nation’s roads. Interventions to increase mindfulness have been used across occupational and personal domains to improve sleep quality, mental health, awareness of the environment, and reaction time.
OBJECTIVE:
The purpose of this study was to examine the relationships between sleep, mental health, health care utilization, and mindfulness in long-haul truck drivers in the United States.
METHODS:
Participants (N = 140) were recruited to complete a web-based survey. Descriptive statistics, bivariate analysis, and regression analysis were used to examine variables of interest.
RESULTS:
Post-traumatic Stress Disorder (PTSD) symptomology and daytime sleepiness predicted mental health care utilization in the past year. Mindfulness was inversely correlated with PTSD symptomology, however in the full regression model, mindfulness failed to predict mental health care utilization.
CONCLUSIONS:
Occupational health professionals should utilize mindfulness screenings as an adjunctive component to traditional mental health screenings and refer drivers for advanced care as appropriate.
Keywords
Introduction
The transportation industry represents one of the largest occupations in the United States [1]. With over three million truck drivers in the United States, the occupational safety of these workers has substantial personal, economic, and community impact [1]. High work demands paired with low autonomy, chronic fatigue, and sleep impairment lead to substantial occupational health risks, including impaired mental health, physical health, and increased risk for accidents, injuries, and fatalities [2–4]. Specifically, sleep-related problems or disturbances have been reported in 17 to 58% of long-haul truckers, including obstructive sleep apnea, insomnia, and fatigue [5, 6]. The incidence is up to four times higher than the general population, plausibly related to increased incidence of obesity (>50%) and psychological distress (depression–26.9%) within the industry [1, 5–7, 1, 5–7].
Long-haul truck drivers are especially vulnerable to post-traumatic stress disorder (PTSD) from previous exposure to accidents, near misses, and a hostile work environment that accompanies the industry [5]. Whereas the incidence of PTSD in the long-haul trucking industry is not well established, the incidence of depression, anxiety, and stress are documented and are associated with poor sleep quality and insomnia, thus, compounding risks [6, 8]. In fact, both sleep disorders and excessive psychiatric stress result in concentration deficits and decreased vigilance, resulting in decreased awareness of the environment and increased risks of near misses, accidents, and injury [6].
To manage occupational hazards and in the interest of public safety, Federal regulations mandate truck drivers monitor their work hours, which limits shifts to 14-hour days with a ten-hour break in between shifts. However, these regulations do not prevent or ameliorate real occupational risks to truck drivers [9]. Truckers have occupational fatality rates 11x higher than the general population [2, 3], and truckers are consistently ranked in the top three occupations for non-fatal injuries and illnesses. For example, in 2016, 475,000 large truck crashes occurred, which resulted in 104,000 truckers who were injured and 3,864 who died [10].
In spite of trends that indicate the transportation industry has grown safer over time, research shows that current regulations are not adequate as a stand-alone intervention to protect the safety of long-haul truckers, or the public –those affected by their presence on United States’ roads [11]. Truckers need individualized interventions to help them effectively manage the hazards of the industry. Although non-traditional to the American way, the Eastern-Buddhist tradition of mindfulness may be key to managing the hazards of the industry [12–17]. Mindfulness refers to a non-judgmental awareness and attention to the present moment [12, 18]. Although relatively new to the American public, the concept and practice of mindfulness has been used in the occupational realm over the last decade [12–17]. A substantial body of evidence suggests that the practice of mindfulness may improve awareness of one’s environment, decreases attentional performance lapses, and improves cognitive function [17–19], which for truckers, can mean increased environmental monitoring and improved reaction time [20]. Further, the practice of mindfulness may also alleviate depression, anxiety, poor sleep quality, and fatigue- all common health hazards within the transportation industry [16, 22]. Because these health risks are also associated with increased risk for accident and injury, mindfulness may be particularly effective in improving the comprehensive health profile of the long-haul trucker, as its influence is far-reaching and plausibly synergistic [2, 23–25].
Although mindfulness has been studied in various populations and within occupational contexts, to our knowledge, it has not been examined among long-haul truck drivers. The purpose of this paper is to describe the results from our study, which examined the associations of mindfulness, sleep, and post-traumatic stress in long-haul truck drivers in the United States. From our results and the current state of literature, we will present the implications of mindfulness in the context of occupational health.
Methods
A convenience sample of participants (N = 140) were recruited through occupational health clinics, a trucking industry marketing company, and word of mouth. Inclusion criteria included: 1) Being employed as a long-haul truck driver; 2) self-report of a current commercial driver’s license; 2) being 18 years of age or older; and 4) having the ability to read and comprehend the English language. Potential participants were provided information about the study, including the purpose of the study, description of procedures, and disclosure of any risks or benefits involved. Upon interest, participants could click a web-based link to begin study procedures. The web-based Qualtrics survey collected no identifying data and incorporated the following instruments: (a) Demographic Survey; (b) Epworth Sleepiness Scale; (c) Karolinska Sleepiness Scale; (d) Mindfulness Attention Scale; (e) Mental Health Issues and Treatment Survey; and (f) PTSD Scale-Civilian Version. Instrument selection was guided by the Transactional Theory of Stress and Coping and based off previous literature review [26]. The entire survey consisted of 75 questions and took approximately thirty minutes to complete. No compensation or incentives were provided. The institutional review board of the University of Alabama at Birmingham approved this study.
Instruments
Demographic survey
This instrument assessed participants’ basic demographic information including gender, race, and age.
Epworth Sleepiness Scale
The Epworth Sleepiness Scale measured the participant’s propensity for daytime sleepiness, and was selected based on previously established reliability among long-haul truck drivers [27]. Item responses on the eight item scale range from 0 to 3, with a total possible score of 24 points. Higher scores indicate greater likelihood of dozing off inappropriately during regular daytime activities, such as watching TV, reading, or sitting in traffic [28].
Karolinska Sleepiness Scale
The Karolinska Sleepiness Scale measured the participant’s current psychophysical state between alert and asleep. A score of one indicates extreme alertness while a score of nine indicates being so sleepy that one cannot stay awake [29]. A limitation of the scale is that it measures subjective alertness over the last ten minutes [29]. The scale was selected based on previous validity with ECG markers of sleep, and strong associations between sleepiness and performance measures [27, 29].
Mindfulness Attention Scale
The Mindfulness Attention and Awareness Scale measured mindful disposition, or open awareness of and attention to the present moment [30]. Item responses range from 1 to 6, with higher scores indicating more mindfulness. The average of item scores indicate the participant’s mindful disposition [31]. The scale was selected based on previously established validity and reliability among the general population [30].
PTSD Scale-Civilian version
The PSTD Scale-Civilian version measured symptomology reflective of the diagnostic criteria for PTSD [32]. Item responses range from 1 to 5, with a total possible score between 17 and 85. Higher scores indicate a greater troublesome effect from a past stressful experience [32]. The scale was selected based on established reliability and validity among the general population [33].
Mental Health Issues and Treatment Survey
This instrument assessed participants’ experience of anxiety, depression, and loneliness, and asked if participants were currently or had ever undergone treatment for these conditions.
Analysis
Participant characteristics were tabulated and descriptive statistics computed for variables of interest. The relationships between participant characteristics (age, years as a commercial truck driver, hours of sleep per night, sleepiness, mindfulness disposition, and PTSD symptomology) were explored using bivariate correlations. Regression analysis was then used to examine the multivariable influence of participant characteristics on the number of times participants sought professional treatment for feelings of upset or distress within the past twelve months. IBM SPSS v. 24 was used to conduct all statistical analysis.
Results
Most participants were female (70%), Caucasian (90%), and middle-aged (mean age of 37 years; median age of 47.5 years) (See Table 1). Almost 14% of our participants (13.6%) experienced symptoms of depression and 10% reported feelings of anxiety or loneliness. Of those participants experiencing emotional distress (26.6 %), most (68.4–92.9%) were not currently receiving treatment (Fig. 1).
Participant Demographics
Participant Demographics
Note. Individual item completion varied.
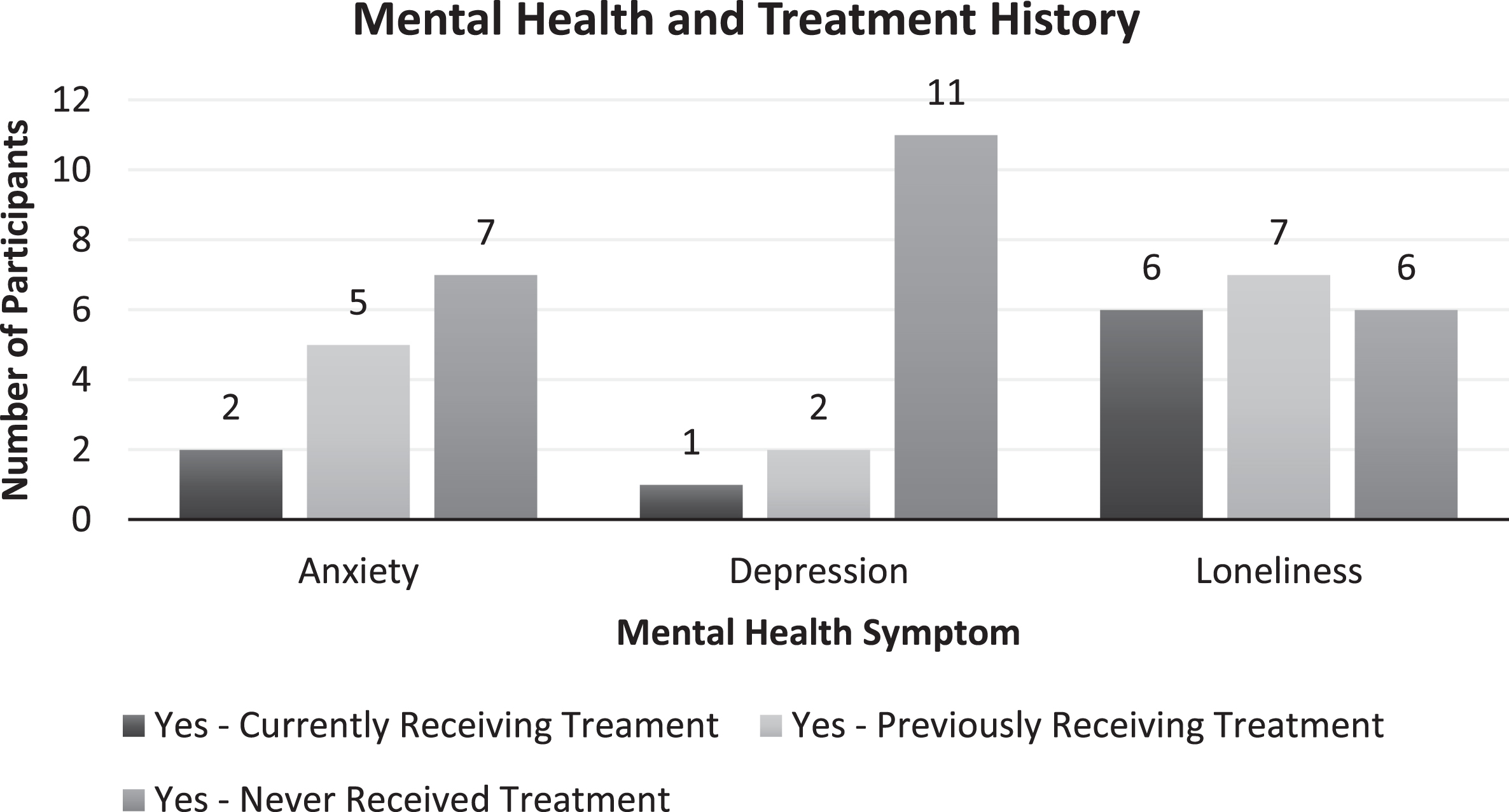
Mental Health and Treatment History.
Most participants (n = 67 or 92%) reported normal daytime sleepiness, with a mean score of 4.6+/–3.2 points on the Epworth Sleepiness Scale (ESS). The maximum range on the ESS is 0–24, and participants in our study scored from 1–17. The literature supports that adults without chronic sleep disorders score on average 4 points, with scores over 10 indicating excessive daytime sleepiness [28]. This indicates that most participants did not experience excessive daytime sleepiness. Only eight percent of participants (n = 5) scored greater than ten on the ESS, indicating excessive daytime sleepiness.
The mean participant score (n = 64) on the Karolinska Sleepiness Scale was 3.8+/–2.1 with a range of 1 to 9 points. For reference, a score of 3.8 reflects a state of being “rather awake”. Thirty percent of participants (n = 13) scored above six, indicating increased risk for driving impairment [34]. Participants (n = 55) reported an average of 5.5 hour of sleep per night +/–2.7 hours. Taken collectively, our participants reported, on average, less than adequate sleep per night without reporting substantial impairment of alertness or excessive daytime sleepiness.
Stress
On average, participants (n = 60) scored 29.9+/–14.4 on the PTSD Scale- Civilian version with a range of 17 to 75. Thirty-five percent (n = 21) or participants scored greater than 30. The suggested cut-off score for the general population is between 30 and 35, with scores greater than this range indicating a need for further evaluation [32]. Fifteen percent of participants (n = 9) scored 44 or more, which is correlated with stressful symptomology status post motor vehicle accidents [35]. For comparison, 15% of the general population is estimated to have PTSD [32]
Mindfulness
Participants (n = 34) scored an average of 4.9+/–0.9 on the Mindfulness Attention and Awareness Scale. Healthy adults typically score ∼4, indicating that our long-haul trucking participants report greater mindful disposition than the general population [31].
Relationships among variables of interest
Age (r = 0.56), mindfulness (r = 0.37), and having ever received treatment for a mental health complaint (r = 0.40) was associated with number of years as a commercial truck driver. This indicates that the contexts associated with being a commercial truck driver may contribute to mental health impairments as well as greater mindful disposition. Based off the evidence, it is plausible that the cumulative, chronic experience of high working demands paired with inadequate sleep and social isolation increases the risk of mental health complaints [36]. Whereas, mindful disposition may be increased related to the practice of professional techniques used in the industry, such as systematic environmental scanning to maintain awareness of the environment. Mindfulness was also positively associated with age (r = 0.33) and negatively associated with PTSD symptomology (r = –0.30), meaning that mindfulness may protect against psychological hazards associated with the industry.
Epworth Sleepiness scores were correlated with Karolinska Sleepiness scores (r = 0.30), but only Karolinska Sleepiness scores (r = 0.30) were correlated with hours of sleep per night. This indicates that alertness and overall awareness of the environment may be impaired before inappropriate daytime dozing occurs.
Post-traumatic stress scores were correlated with both Epworth Sleepiness (r = 0.29) and Karolinska Sleepiness scores (r = 0.33), and having received mental health services in the past 12 months (r = 0.60). This means that participants with greater PTSD symptomology were more likely to have received mental health services in the past twelve months, and that there was a small relationship between mental health complaints and subjectively inadequate sleep.
Mindfulness disposition was inversely correlated with post-traumatic stress symptomology (r = –0.66), Karolinska Sleepiness scores (r = –0.50), and having received mental health treatment in the past 12 months (r = –0.38). This indicates that mindfulness may play a protective role in protecting against PTSD symptomology within this high-risk population. Higher scores on the Karolinska Sleepiness scale indicate greater sleepiness, meaning that mindfulness is associated with greater alertness. No other bivariate relationships yielded a correlation ≥0.30. Table 2 portrays all bivariate relationships examined.
Relationships Among Variables of Interest
Relationships Among Variables of Interest
Note. Significant findings indicated in bold.
A single regression model identified the variables of interest on having received mental health services over the past twelve months. The total variance explained in the dependent variable (having received mental health services in the past twelve month) by all variables of interest was 48.5% (p = 0.002), indicating a large effect [37]. Significant predictors of having received mental health services in the past twelve months were years as a commercial truck driver (β= 0.312; p = 0.047), sleepiness as measured through the Karolinska Sleepiness Scale (β= –0.425; p = 0.031), and post-traumatic stress symptomology (β= 0.576; p = 0.006). (*Please note higher Karolinska Sleepiness scores indicate greater sleepiness.) Tables 3 and 4 provides additional detail on regression modeling results.
Single Regression Model
Note. Dependent Variable: Have you received professional treatment for your feelings of upset or distress at any time in the past 12 months?
ANOVA
Note. Dependent Variable: Have you received professional treatment for your feelings of upset or distress at any time in the past 12 months?
Overall, although we found that most participants did not report excessive daytime sleepiness, the average hours of sleep per night reported was 5.5, substantially less than the 7–9 hours recommended to avoid the consequences of sleep deprivation including slowed reaction time, impaired judgement, and symptoms of depression [6, 38]. In fact, sleepiness and number of years as a long-haul trucker were associated with increased mental health complaints. Whereas, mindful disposition was associated with less PTSD symptomology, greater alertness, and greater incidence of having sought mental health care in the past twelve months.
The literature supports that the schedule, demands, and overall long-haul truck driving culture place drivers at risk for impaired mental health, low health care utilization, and inadequate sleep [1, 4]. In turn, this population experiences increased risks to total worker health, affecting the workers and the communities they serve [2]. As total worker health influences not only the individual’s quality of life, but also influences occupational safety, understanding ways to improve total worker health warrants our concern [39].
Although more research is needed, mindfulness warrants consideration in the improvement of the overall total worker health and occupational safety profiles of those working in the transportation industry. The practice of mindful awareness has gained support over the past decade as a factor promoting occupational safety through increased awareness and attention to the present environment, and improved executive functioning [17, 40]. Excitingly, mindfulness may also alleviate common health burdens associated with the transportation industry, including excessive fatigue, sleepiness, and impaired mental health, which influence total worker health and occupational risks [14, 41].
However, in our study, mindfulness failed to predict utilization of mental health care when all other variables of interest were considered. In the full regression model, it was PTSD symptomology and sleep –and not mindfulness- that remained the significant, modifiable characteristics predicting utilization of care. This means that mindfulness was insufficient as a predictor of health care utilization in the face of more severe PTSD symptomology. Whereas mindfulness improves personal regulation of emotion (i.e., loneliness, depression, anxiety) [42], our results indicate that there is a threshold past which mindful disposition is inadequate to protect against more severe symptomology, such as that seen in PTSD [16, 22]. Therefore, any mindfulness applications should be paired with mental health screenings and referral to care when appropriate.
In addition to PTSD symptomology, sleepiness remained significant in the multivariable model predicting mental health care utilization. Specifically, participants reporting greater sleepiness were less likely to utilize mental health care services. Yet, our bivariate analysis showed that excessive sleepiness was associated with increased PTSD symptomology, which should follow trends for increased health care utilization. Drivers may not view sleep problems as issues that could be addressed through mental health care treatment. Although we did not measure this directly, sleepiness is a concept very close to that of fatigue, which is known to alter motivation and compliance to safety regulations [43]. Therefore, it is not unreasonable that self-care, such as utilization of mental health care, would suffer in the face of impaired sleep and consequential fatigue. Therefore, risks for poor mental health utilization should be examined holistically.
Although this study is the first of its kind to examine the associations between mindfulness, PTSD, and mental health care utilization among long-haul truck drivers in the US, and important associations were found, more research is needed to understand the mechanisms of effects, and the best interventions to fill health care gaps. We acknowledge that this study was limited due to inherent bias and variability of self-reported outcomes, real-time attrition (drivers who started the survey but did not finish it), and that the sample is not representative of the general long-haul trucking population, which is predominately male. Further, this study is limited by the fact that data was not obtained related to previous exposure to or training in mindfulness practice. Future research should continue to examine the relationships between sleep, mental health, and safety, and explore mindfulness as a potential moderator to occupational risks. More objective measures, such as sleep studies, and research addressing the feasibility and acceptability of implementing mindfulness interventions among long-haul truckers should also be considered. Although our study did not find that mindfulness predicts health care utilization, considering the promise of mindfulness to improve mental health, sleep, and overall occupational safety, more research is warranted.
Results from our study has several implications for practice. Occupational health professionals should screen for inadequate sleep and impaired mental health in this population and find innovative ways to increase health care utilization in this transient population with unique health care needs. Targeted mobile messaging and mobile health care visits may prove beneficial to increase awareness and knowledge of common health burdens, and to facilitate linkage to care and adherence to health treatment plans [44, 45]. Screening instruments, such as those used in this study, can be administered via mobile devices when needed, although time burden to clients should be considered when choosing strategies to increase worker health. Specifically, occupational health professionals should consider the Epworth and Karolinska Sleepiness Scales to quickly screen and assess propensity for daytime sleepiness and excessive sleepiness, respectively [29, 46]. The PTSD-Civilian Scale can be used to quickly screen for PTSD symptomology and can be paired with instruments to assess general depressive symptomology through tools such as the CES-D [32, 47]. Whereas these are not diagnostic tools, they hold value in identifying risk and the need for referral. Likewise, mindfulness scales, such as the Mindfulness Attention and Awareness Scale, can be used in conjunction with mobile mindfulness training platforms as adjunctive therapy [30, 48].
Although screening is due diligence, employers and policy makers must also consider the implications this research offers. Namely, 1) Excessive sleepiness and mindful disposition influence total worker health and occupational health and safety; and 2) The federal regulations currently in place are inadequate as a stand-alone intervention to promote sufficient sleep and decrease risks associated with sleepiness and fatigue. Further, it is unlikely that there are any policies or programs in place to promote mindfulness, which continues to show promise through increased awareness, reaction time, and judgement, and extend its influence to promote improved sleep and mental health [17, 49]. It is time that our driving companies and policy makers consider mindfulness as an intervention.
Within the Total Worker Health framework, mindfulness should be considered as a means to improve both occupational health and safety, and the overall health and wellbeing of the worker [39]. Therefore, work-based programs and policies to incorporate mindful practice-beyond simple screening- into daily life are warranted [39]. Specifically, employers of the transportation industry can support the practice of mindfulness through increasing the availability and feasibility of mindfulness training. Both seminar-style and distance accessible mindfulness-based interventions have demonstrated improvements in mindful disposition and psychological wellbeing in the general population, making either option viable to suit the schedules and preferences of employees [50, 51]. Policies to support increased mindfulness include the provision of annual competencies on mindfulness, company-based incentives for demonstrating a personal commitment to the practice, and a commitment from leadership to continue to provide time for mindfulness training [39]. In these ways, a more comprehensive commitment to total worker health and occupational health and safety can be implemented, with the safety of over 3 million workers in consideration.
Conclusion
The transportation industry carries substantial risk for impaired occupational safety and total worker health. Inadequate sleep and impaired mental health further exacerbate risks [1, 2]. It is our duty as occupational health professionals to continue research and translation efforts to improve the health of the three million workers serving this industry and our nation’s needs. Occupational health professionals can facilitate improvements in total worker health and the overall safety profile of the industry through the systematic implementation of evidence-based techniques to increase awareness and identification of risks associated with the occupation while finding innovative ways to reach a transient population and link them to much needed health care. Specifically, more effort is needed to evaluate the feasibility, acceptability, and effectiveness of interventions, such as mindfulness, within the transportation industry and to convince our industry leaders of the human and economic worth of implementing the programs, policies, and practices associated with a total worker health framework.
Conflict of interest
None to report.