
Abstract
BACKGROUND:
Accidental occupational injuries increase the risk of communicable diseases like hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) among dental personnel. Such occupational injuries affect healthcare quality by enhancing dissatisfaction and lack of motivation to work among dental personnel.
OBJECTIVE:
The present study aims to assess knowledge and awareness regarding needle stick and sharp injury among dental personnel and compared the knowledge and awareness level about needle stick injuries between dental professionals and dental supporting staff working at the School of Dental Sciences, Universiti Sains Malaysia.
METHODS:
This cross-sectional study was conducted from March 2016 to March 2017. The total sample included 112 registered dental personnel including dental professionals (lecturers, dental officers, and postgraduate students) and dental supportive staff (including staff nurses and dental surgery assistant) who were selected from the School of Dental Sciences, Universiti Sains Malaysia at Kelantan District of Malaysia. Data were collected by a structured questionnaire.
RESULTS:
In our study 60.7% respondents answered correctly for all the statements regarding knowledge and 51.8% of the respondents answered correctly for the statements regarding awareness on needle stick and sharp injury. No significant difference of knowledge level has been observed between the dental professionals and dental supportive staff (p < 0.819), whereas the awareness level was significantly different between these two groups (p < 0.016).
CONCLUSIONS:
There is a difference regarding awareness level on needle stick and sharp injury between dental professionals and dental supportive staff in our study but no differences were found in knowledge level between two groups.
Keywords
Introduction
Accidental occupational injuries among dental personnel continue to be a significant problem in the healthcare system because of the associated risk of acquiring infections [1]. The highest one year pooled prevalence of occupational percutaneous injury among dental workers was found to be 54.8% in Asia from a systematic review and meta-analysis based on studies published from January 2008 to January 2018, which reported the prevalence of percuteneous injuries among Healthcare workers [2].
However, percutenious injury increases the risk of communicable diseases like hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) [2, 3]. Such occupational injury leads to workers’ dissatisfaction and psychological trauma including depression, anxiety, post-traumatic stress disorder and causes job burnout which in turns enhances financial cost to the healthcare system [3]. This financial cost may be associated with management of illness of worker or compensation claims by the affected person [2, 4]. Consecutively, a clear impact has been observed on healthcare workers’ quality of life who had experienced needle stick and sharp injuries [5].
A study performed among southern Indian dental professionals in 2012, it was reported that 27.5% of the respondents had experienced at least one needle stick and sharp injury due to inadequate knowledge [6], whereas 50.9% Brazilian dental students had the same experience in 2016 [7]. However, Malaysian medical healthcare workers showed the highest incidence (21.1 per 1000 HCWs) of needle stick and sharp injuries followed by dental staff (7.5 per 1000 HCWs) in 2016 which became a matter of great concern for the health care sector [8].
Most of the recent studies regarding needle stick and sharp injuries emphasize healthcare professionals only [5, 9]. However, similar data among dental personnel are scarce although risks of needle stick and sharp injury in dental settings are very common. During routine use of sharp instruments for dental treatments as well as cleaning and disposing instruments, dental personnel have frequent exposure to diverse bacterial flora present in blood and saliva which increases chance of acquiring blood-borne infections [10]. Moreover, at a university hospital, dental procedures, cleaning and disposing instruments are often executed in limited time and with lack of skills [11].
Considering the safety issues of dental personnel it is mandatory to assess the knowledge and awareness level regarding needle stick and occupational sharp injury among dental personnel [10]. Additionally, findings from our study will help policy makers to understand the current scenario and create new policies in order to prevent needle stick and sharp injuries in dental settings. Considering the situation, in this study, we aimed to assess needle stick and sharp injury related knowledge and awareness among dental personnel and to compare knowledge and awareness level regarding needle stick and sharp injury between dental professionals and dental supporting staff working at the School of Dental Sciences, Universiti Sains Malaysia.
Methodology
This was a cross-sectional study. The sample included dental professionals (dental officers, dental lecturers, and postgraduate students) and dental supporting staff (dental nurses and dental surgery assistants) who worked at the School of Dental Science, Universiti Sains Malaysia, Kelantan District, Malaysia. These personnel met the inclusion criteria, which were: dental officers, dental lecturers, dental nurses, dental surgery assistants, and postgraduate students working at the School of Dental Sciences, Universiti Sains Malaysia for more than one year. The exclusion criteria were: lecturers working at the School of Dental Sciences, Universiti Sains Malaysia who do not specialize in dental-related subjects and postgraduate students who are involved in the medical field.
The total sample size was 115 dental healthcare personnel, including 65 dental professionals and 50 dental supporting staff. Due to unwillingness to participate, the study was completed with 112 samples. Among them, 63 were dental professionals including lecturers, dental officers, and postgraduate students, and 49 were dental supportive staff including staff nurses and dental surgery assistants. The purposive sampling method was applied to achieve the sample size. To achieve this, we included all dental nurses and dental surgery assistants, but we selected dental officers, dental postgraduate students, and dental lecturers randomly.
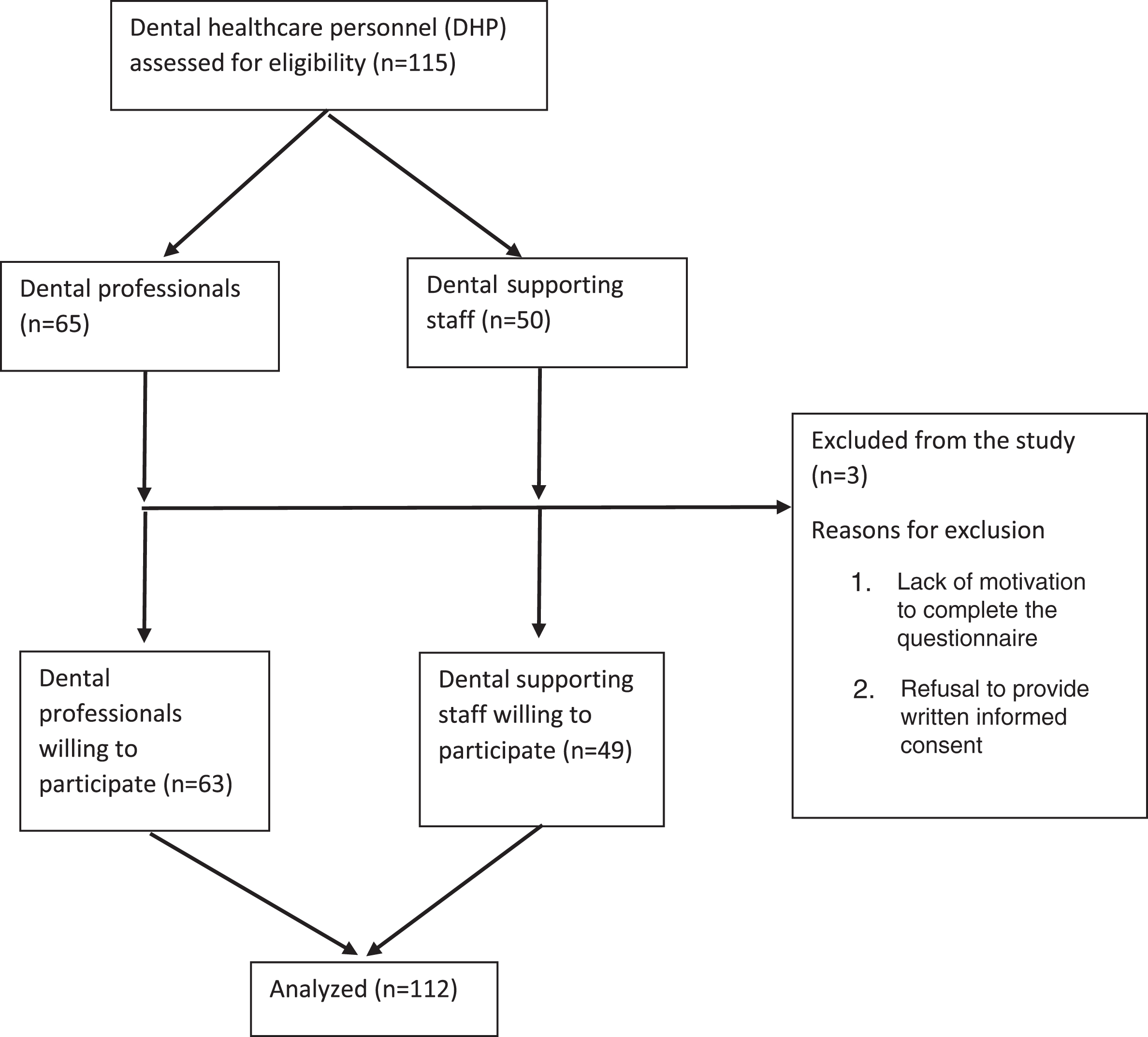
STROBE flowchart of recruitment of the health care personnel (study subjects).
Our research tool was a structured questionnaire, which consists of five sections. Section 1 assessed the sociodemographic data of the respondents including background information, such as age, gender, marital status, educational level, and details about their occupation and hepatitis B vaccination status. The details regarding their occupation asked in the questionnaire were job category, total service year, working hours per week, work in shift or overtime, number of patients treated, and injections per day. Section 2 assessed the frequency and determinants of needle stick and sharp injuries during their clinical life, the reporting behavior, and the management practice of respondents towards Needle stick and sharp injury. Section 3 assessed their knowledge level, and Section 4 assessed their awareness level. The questionnaire was adopted from related studies [5–8]. It was translated and validated in Malay prior to data collection.
In addition, internal consistency was tested, and Cronbach’s alpha was 0.75, which was considered acceptable. Data entry and analysis were conducted using SPSS version 22.0. For the descriptive analysis, categorical data were analyzed with the use of percentages and frequency, whereas numerical data were analyzed with the use of mean, median, standard deviation, and interquartile range. A score of 1 was given for a correct answer, whereas 0 was given for a wrong answer. Student’s t-test was performed to determine differences between dental professionals and dental supportive staff. The study protocol was approved by the Human Research and Ethics Committee of Universiti Sains Malaysia. Respondents were told that the information provided is confidential and that their identities are not revealed with regard to the information they provided. In addition, informed consent was taken prior to data collection.
The total sample size was estimated to be 115 but due to unwillingness to participate, the total sample size was 112. Among the respondents, a few (8%) of the respondents reported experiencing needle stick and sharp injury in the previous one year and all of them reported about needle stick and sharp injury to their supervisors immediate after acquiring injury and 66.7% of them had taken post-exposure prophylaxis (PEP). Among them less than half of the respondents chose to promote active bleeding of injury site (11.1%) and wash the wound thoroughly with soap and running water (33.3%) as recommended by the guidelines. When enquired for vaccination status among healthcare personnel almost all (98.2%) reported to be immunized against Hepatitis B with at least one dose. Among the respondents, the majority (75.0%) had a total service year of five years and above. Most of them did not work in shift (94.6%), and more than half did not work overtime (64.3%). The respondents had average working hours of 39.13 (±8.48 SD) per week. According to our survey, the average number of patients treated per day was approximately 3, whereas the number of injections given per day was at least one. About half of the injuries (44.4%) were caused by needle only, followed by needle and file together (33.3%), coupland elevator (11.1%) and periodontal probe (11.1%). When enquiring about factors responsible for injury more than half (55.6%) of them suggested hastily cleaning and disposing of instruments followed by crowded space (33.3%), fatigue (22.2%) and imprudence of colleagues (11.1%).
Table 1 shows the sociodemographic characteristics of the dental personnel by age, sex, education level, and job categories. More than half of them had age groups of 31 to 40 years old (54.5%) and two third of them were female (66.1%). The majority was married (80.4%). Among the respondents, one fourth (25%) were dental surgery assistants, followed by dental lecturers (23.2%), community nurses (20.3%), postgraduate students (19.6%), dental nurses (18.8%), and dental officers (13.4%).
Socio-demographic characteristics of the dental personnel (n = 112)
Socio-demographic characteristics of the dental personnel (n = 112)
Table 2 reveals work activities associated with needle stick and sharp injuries among respondents experienced injury. When the respondents were asked about tasks performed during injury, they reported that one third of the injuries (33.3%) occurred during handling or aftercare of needles or sharps on tray, followed by recapping needle after use (22.2%), injection (11.1%), passing needle (11.1%) and suturing (11.1%) and disassembling needle or sharp devices (11.1%).
Work activities associated with needle stick and sharp injuries (n = 9)
Table 3 presents the assessment of knowledge on needle stick and sharp injury. When the respondents were asked whether they know about Universal Precaution Guidelines, the majority (83%) answered that they knew about them. In addition, when they were asked about safety needles or safety syringes, most of them (86.6%) answered that they heard about them.
Knowledge on needle stick and sharp injuries among dental personnel (n = 112)
Table 4 presents the awareness on needle stick and sharp injury. The majority (90%) of the respondents were aware that most injuries occurred during disposal of used needles. Among them, more than two thirds (78.6%) of the respondents reported that PEP should be initiated within 1 hour of the injury. Meanwhile, 68.8% answered that the risk of HIV transmission from needle stick injury is 0.3%. Most (86.6%) of the respondents reported that they had received training regarding infection control, and almost all of them (95.5%) followed the Universal Precaution Guidelines.
Awareness on needle stick and sharp injuries among dental personnel (n = 112)
Table 5 reveals the results of independent t-test analysis to compare the level of knowledge and awareness regarding needle stick and sharp injury between dental professionals and dental supportive staff. No significant difference of knowledge level was observed between the two groups (p < 0.819) but the awareness level was significantly different between these two groups (p < 0.016).
Comparison of knowledge and awareness between dental professionals and dental supportive staff (n = 112)
*Significant level p value <0.05.
To the best of our knowledge, this is the first study that assessed the knowledge and awareness regarding needle stick and sharp injury among dental personnel in Kelantan, Malaysia. Our study period was from March 2016 to March 2017. Our study results revealed that most of the injuries occurred during recapping (22.2%) and handling (33.3%). This result is consistent with other studies of needle stick and sharp injury among dental personnel [6, 13]. This is probably because most of the injuries occurred among the dental supportive staff because they were in charge of cleaning up and washing the instruments. In agreement with a study performed by Malik, the majority of our respondents (77.8%) reported the incident to their supervisors although 83% stated that they know about the Universal Precaution Guidelines [10]. However, gaps were observed in the knowledge and practice. Reporting rate was quite satisfactory in our study compared with the study performed in similar context among medical Health care workers in the same country; meanwhile, only 30.9% had reported the incident of needle stick and sharp injury according to their result [14]. Immediate reporting of occupational exposures to the authority was necessary to ensure appropriate counseling and facilitate prophylaxis or early treatment [10]. Among the respondents almost all (98.2%) reported that they were immunized against Hepatitis B while similar findings can be seen in a study performed in Turkey among healthcare workers [3].
Despite having good knowledge on infection control of washing a wound area, less than half of the respondents chose to promote active bleeding of injury site (11.1%) and wash the wound thoroughly with soap and running water (33.3%) as recommended by the guidelines. In the present study, the majority of our respondents answered correctly for most of the statements regarding knowledge on needle stick and sharp injury. These findings were higher than the findings indicated in a study conducted at the Rural Dental College of India, probably due to participation of training in infection control [15]. In this study findings showed no relation between knowledge and practice of needle stick and sharp injury among the respondents. Somehow, an information gap still remained on practice and safe practice.
Among the respondents, only one third (34.8%) thought that most needle stick injuries have not been neglected so far. This may be because the reporting protocols for needle stick and sharp injury have not been well established and fully known by them. More than half of the respondents answered correctly for all the statements regarding awareness on needle stick and sharp injury. This result is better than the study conducted at the Rural Dental College in India [15].
No significant difference was observed between the knowledge level of dental professionals and dental supportive staff regarding needle stick and sharp injury needle stick and sharp injury. However, the awareness level is significantly different between the two groups. Dental professionals are shown to have a higher awareness level regarding needle stick and sharp injury than the dental supportive staff.
This phenomenon can be attributed to the existence of stringent infection control program, regular training of the staff on the standard precautions, inclusion of infection control practices in the teaching curriculum of the medical and dental students, surveillance and the regular practices of use of gloves, and availability of safety devices. The Centers of Disease Control reiterates the importance of a culture of safety in the work place to prevent occupational hazards. The strategies that should be employed to improve staff practices toward safety measures include established multidisciplinary injury–prevention teams with representatives from all disciplines at risk for exposure, written exposure control plan with a hard copy available to all employees, enforcement of sharps injury reporting and records, and education of frontline workers.
Our study also showed that the majority (66.1%) of the dental personnel had the misconception that needles should be recapped after use. The recapping of needles has already been prohibited under the Occupation Safety and Health Administration (OSHA) blood-borne pathogen standard [16]. In addition, only 52.5% knew about needleless safety devices. The availability and compliance to adopting safety-engineered devices will help in reducing needle stick and sharp injuries and risk of blood-borne infections including HIV/AIDS.
Timely reporting of occupational exposures to an employee health service is a prerequisite to ensure appropriate counseling, facilitate prophylaxis or early treatment, and establish legal prerequisites for workers’ compensation [17].
The limitation of the study is that data were collected from a tertiary level hospital only, and no information was taken from private dental clinics at Kelantan. The study results might not represent the entire scenario of Kelantan district. This study also might not reveal the information regarding knowledge and awareness of needle stick and sharp injury among dental personnel in the entire country. Another limitation has been observed among dental healthcare personnel during recalling the pattern and number of sharp injuries they had experienced during past one year. However, we tried to reduce the recall bias by checking the records where they had reported about their injury.
Finally, we can agree that despite adequate demonstration of knowledge on Universal Precaution Guidelines, the precautions were not fully practiced. Practice of standard precautions for infection control needs to be followed by all HCWs irrespective of the patient diagnosis and perceived infection status [18, 19]. To obtain optimum level of safety precaution practices among HCWs, training and education on workplace safety, safe handling and disposal of sharps, provision of personal protective equipment, availability of safety engineered devices, health education materials displaying the protocol and flow chart of reporting on exposures, and access to interventions are required.
Conclusion
In our study, no significant difference was observed in the knowledge level. However, a significant difference was observed in the awareness level between dental professionals and dental supportive staff working at the School of Dental Sciences at Universiti Sains Malaysia regarding needle stick and sharp injury. Thus, further improving the knowledge and awareness of dental professionals and dental supportive staff in Kelantan is of the utmost importance.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We are grateful to the dental lecturers, dental officers, dental postgraduate students, dental staff nurses and dental surgery assistants who participated in our study. We would also like to acknowledge the School of Dental Sciences, Universiti Sains Malaysia for giving us the opportunity to conduct this important research.