
Abstract
BACKGROUND:
Workers with persistent disabling low back pain (LBP) often encounter difficulty staying at work. Self-management (SM) programs can offer interesting avenues to help workers stay at work.
OBJECTIVE:
To establish the plausibility of a logic model operationalizing a SM program designed to help workers with persistent disabling LBP stay at work.
METHODS:
We used a qualitative design. A preliminary version of the logic model was developed based on the literature and McLaughlin et al.’s framework for logic models. Clinicians in work rehabilitation completed an online survey on the plausibility of the logic model and proposed modifications, which were discussed in a focus group. Thematic analyses were performed.
RESULTS:
Participants (n = 11) found the model plausible, contingent upon a few modifications. They raised the importance of making more explicit the margin of maneuver or “job leeway” for a worker who is trying to stay at work and suggested emphasizing a capability approach. Enhancing the workers’ perceived self-efficacy and communication skills were deemed essential tasks of the model.
CONCLUSION:
A plausible logic model for a SM program designed for workers with disabling LBP stay at work was developed. The next step will be to assess its acceptability with potential users.
Introduction
Non-specific low back pain (LBP) is a musculoskeletal disorder defined as pain primarily in the low back region but sometimes referring to the lower limb and not attributable to a specific, recognizable, and known pathology (e.g., infection or fracture) [1, 2]. Some authors consider LBP persistent when symptoms continue for more than three months [3]. LBP is highly prevalent among the general population (about 38%) and affects a large number of workers [4]. LBP-related work disabilities are common. With a lifetime prevalence ranging between 60% and 80% [5], they represent a worldwide socioeconomic burden, which is mostly attributable to a small proportion of individuals who suffer from persistent pain and disability associated with long-term sick leave [6].
Despite the existence of various rehabilitation programs for work-related injuries, many workers who have completed their rehabilitation and returned to their jobs have difficulty staying at work [7]. Staying at work can be defined as workers’ ability to perform their work and meet their employer’s performance requirements without compromising the judicious management of their symptoms and disabilities following a return to work (RTW) [8]. Even if most workers are able to RTW following an injury, studies estimate at 50–60% the one-year recurrence rate of symptoms among people having recovered from an episode of acute LBP at work, while the one-year work disability recurrence rate is 10–15% [9, 10].
To address this problem, programs focusing on symptom self-management (SM) offer interesting avenues for managing LBP, and more importantly, for reinforcing workers’ ability to stay at work [11]. SM can be defined as patients’ ability to manage their symptoms, treatment, and the physical, psychological and social consequences of their health condition, as well as the changes in lifestyle habits that their condition requires [12, 13]. An SM program offers a means for developing users’ skills in managing their own condition by providing them with SM strategies and advice tailored to their needs [12, 14]. Although noteworthy, these programs do not propose strategies designed specifically to foster a sustainable RTW. Yet, Shaw et al. [15] suggest that it is feasible to adapt such programs to help workers with persistent LBP manage and reduce their disability, and ultimately to promote their sustainable RTW.
An SM program for workers with persistent LBP designed to help them stay at work would fit the definition of a complex intervention (e.g., healthcare interventions aimed at changing patients’ behaviors and strengthening their ability to manage their pain and disabilities) [16]. Indeed, it is considered a complex intervention since it has to take into consideration many interacting components (i.e., patients’ behaviors and beliefs) at different organizational levels (i.e., individual, social and occupational), while permitting a high degree of tailoring based on patients’ needs [16, 17].
One of the first steps in developing complex interventions is to elaborate a plausible logic model, based on the scientific literature on the issue under study (i.e., stay at work) [17, 18]. Evidence shows that a logic model represents a valid means for explicitly demonstrating how a program works, as it explains the relationships between objectives, activities and tasks, and identifies the resources needed to obtain the desired outcomes [18, 19]. This approach, used in the evaluative research field, provides insight into causal relationships between an intervention’s components [20]. To ensure the plausibility of a logic model, key stakeholders, such as work rehabilitation clinicians, associated with the issue under study must be consulted [18]. To our knowledge, a logic model for an SM program aimed specifically at helping workers with persistent LBP stay at work has been neither designed nor assessed to date by key stakeholders. Thus, the objective of this study was to seek the opinions of experienced clinicians in the work rehabilitation field to document the plausibility of a logic model for such an SM program.
Methods
Study design
This study used a pragmatic theoretical approach, as knowledge arises out of actions, situations and consequences within a social and political context [21]. A qualitative design [22] involving a two-phase process adapted from Coutu et al. [23] was used. First, participants had to complete a self-administered questionnaire on the plausibility of the logic model by appraising its plausibility and suggesting modifications if deemed necessary. The same participants took part in a focus group [22] to discuss the proposed modifications to the logic model in order to ensure its plausibility. The authors used the Consolidated criteria for reporting qualitative research (COREQ) [24] checklist to report all relevant information.
To develop the logic model for an SM program designed specifically to help workers with persistent and disabling LBP stay at work, we followed McLaughlin et al.’s framework for developing logic models [19]. First, we gathered empirical data via a thorough literature review. This included a narrative review of theoretical models underlying the SM model [25], as well as a systematic review of the essential elements for an SM program for persistent LBP and disability that has been proven effective [26]. The integration of these results led to the development of a logic model based on the principles of a behavior change model: the common-sense model of self-regulation of illness [27, 28]. The logic model’s ultimate goal is to support a sustainable return to regular work for workers who have been on long-term sick leave due to persistent and disabling LBP. It is composed of four specific objectives that operationalize a problem-solving process, which constitutes the general objective of the model (see Fig. 1). Each specific objective is composed of two sub-objectives, which in turn have their own activities and tasks allowing the attainment of each specific objective.
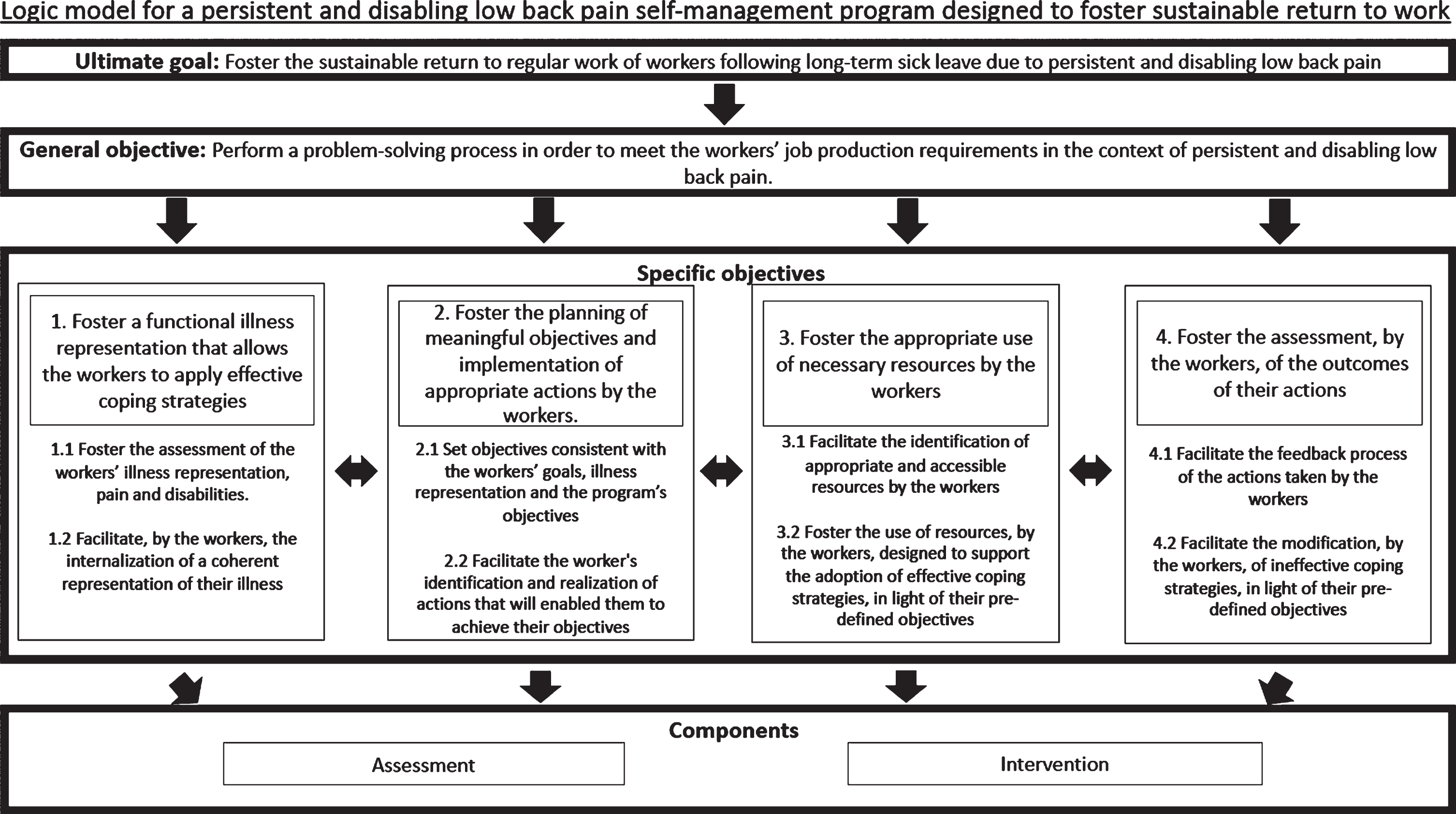
Objectives of the proposed logic model for the SM program.
A convenience sample of rehabilitation clinicians from the private and public sectors in the province of Quebec, Canada, was recruited to participate in the study. The authors aimed to recruit 8 to 12 participants for the focus group. This is consistent with previous, similarly designed studies [23] and current literature on focus groups [29, 30], and ensures that each participant has the opportunity to express opinions and that data saturation is achieved on main themes [29, 30]. The inclusion criteria were as follows: 1) at least two years of clinical experience in work rehabilitation with workers who had work disabilities related to musculoskeletal disorders (MSDs), and 2) the ability to communicate in and read French. Clinicians from various professions in the rehabilitation field (e.g., physical therapist and occupational therapist) were invited. Rehabilitation professionals with widely ranging perspectives were recruited to include multiple points of view. Invitations were sent out by email and the recruitment period lasted three weeks, from March to April 2018. The focus group was held in a university setting and composed of homogeneous participants (i.e., rehabilitation professionals). Participants received financial compensation for their participation since the focus group was held outside normal working hours.
Ethics statement
The study protocol was approved by the Ethics Committee of the Centre Intégré Universitaire de Santé et Services Sociaux de l’Estrie- Centre Hospitalier Universitaire de Sherbrooke (CER CIUSSS de l’Estrie-CHUS) (project number: 2018–2640). All participants gave their written informed consent to participate in the two phases of this study (online survey and focus group) and for the audio recording and transcription of the focus group. They were advised that all collected data would be kept confidential and anonymized.
Data collection
Phase 1: Survey on the plausibility of the logic model, conducted via a self-administered online questionnaire
First, the preliminary version of the logic model for the SM program was sent by email to each participant, along with a link to an online questionnaire. Through the SurveyMonkey© platform, participants were informed about the study context and then asked to view a short informative video summarizing the key elements of the logic model. Afterwards, participants were asked questions related to the logic model components. The questionnaire was pre-tested by five health professionals. The questions asked were based on the work done by Rossi et al. [31] on plausibility assessment. The questions were as follow: 1) Are the objectives presented in the model relevant and sufficient to achieve the ultimate goal of the program?, 2) Are the objectives clearly formulated and well defined?, and 3) Are the activities and tasks in the model necessary and sufficient to attain their respective objectives? For each question, participants had to answer yes or no to indicate whether they agreed or not. All the participants’ answers remained anonymous to prevent potential bias. When they disagreed with a question (i.e., they answered no), they were asked to suggest possible modifications to the formulation of the objective, activity or task to increase its plausibility. Participants had three weeks to complete the survey. Their answers and proposed modifications were used to structure the focus group (phase 2). This first phase also gave participants enough time and resources to prepare for the focus group.
Phase 2: Focus group
All the proposals made by the participants were compiled by the research team and transcribed into a summary of findings, which was then given to each participant. The facilitators read aloud all of the proposals generated by the questionnaire for a given component. Participants were then asked to discuss the plausibility of the proposals, based on their relevance, clarity, definition and necessity. At the end of each discussion on a specific component of the logic model, the facilitators summarized the information to facilitate comprehension and help the participants and the research team better understand the changes proposed to increase the model’s plausibility. The focus group was audiotaped and the researchers took notes to complete data collection. The group was conducted by a researcher experienced with this method (MFC) and a student-researcher (CL), for a total of three hours. The facilitators took great care to ask open-ended questions as neutrally as possible to avoid influencing the participants’ responses. The data were collected in French. For publication, all quotations were translated by a certified translator.
Data analysis
No data analyses were conducted of the survey results, as all proposals made by the participants on the questionnaire to increase plausibility were transcribed and anonymized by the research team. No results were given to the participants to avoid impacting the content of the focus group discussion. Thematic analysis was performed on the transcribed verbatim. Coding was performed manually by two members of the research team (CL and YTL) using a predefined coding list pertaining to the components of the logic model (i.e., objective, activities and tasks). Emergent codes were sought in an effort to remain as faithful as possible to the transcript. The codings assigned to the verbatim by two members of the research team (CL and YTL) were compared. The results were discussed by the researchers, and when there were coding discrepancies, the discussion continued until a consensus was reached. Based on the thematic analysis of the transcript, a summary of the main findings regarding ways to improve the objectives, activities and tasks to achieve greater plausibility of the logic model was written for the focus group. This summary ultimately helped to establish the final logic model that obtained consensus among the research team members.
Results
Participants’ characteristics
A total of 32 clinicians were invited to potentially participate in the study. Six expressed interest in taking part in the study but were not available, and 15 never replied to the email invitation. A total of 11 participants therefore took part in the focus group, and only one participant was unable to complete the online questionnaire prior to the focus group due to personal constraints (see Fig. 2). However, this participant did perform all other tasks in preparation for the focus group and participated actively in the discussions.

Flowchart of the recruitment process for focus group participants.
The recruited participants were mostly women working as occupational therapists. Their mean age was 41 years (range = 28–59 years) with clinical experience ranging from 5–30 years (mean experience of 16.18 years). Since all the participants were health professionals, they all had at least a bachelor’s degree in their own profession. The majority had qualifications above entry level (i.e., master’s or doctoral degree and continuing education) in health sciences programs (see Table 1).
Participants’ sociodemographic characteristics
* = The age and years of experience variables are presented within a specific range of numbers in order to ensure the confidentiality of the participants. 1OT = Occupational therapist. 2PT = Physical therapist. 3PSY=Psychologist.
During phase 1, participants who completed the online questionnaire made a total of 53 proposals, 38 concerning the objectives and 15 regarding the tasks and activities. This represents an average of 5.3 proposed modifications per participant. No proposed modifications were suggested for objectives 3.2, 4.1 and 4.2 of the original logic model, as well as the activities and tasks related to objective 3.1 Therefore, these components were not discussed during the focus group.
Overall, these results suggested that, our panel of rehabilitation clinicians found the model to be plausible, contingent upon a few modifications. Essentially, all summarized modifications proposed by the focus group were integrated. During the focus group, participants grouped most of the 53 individual proposed modifications, leading to a lower number of modifications. Also, some individual suggestions made by the participants in the survey concerning very specific changes to the wording of certain components of the model were documented and integrated directly into the final version. The final English version is available on the following website: https://www.usherbrooke.ca/caprit/.
General objective: Perform a problem-solving process in order to meet the workers’ job production requirements in the context of persistent and disabling low back pain
Participants raised the importance of making more explicit in the model the margin of maneuver for a worker who is trying to stay at work. Based on ergonomics, the concept of margin of manoeuver at work refers to the leeway given to a worker to continually adjust his or her work activities to varying demands and capacities over time so as to preserve a balance between the two [32]. This leeway is determined by the worker’s work situation (social environment, work demands, work adjustments and tools, as well as, working conditions), but also by certain individual factors (representations, capacities, concrete living situation) related to his or her personal life.
“Lastly, regarding the idea of margin of maneuver, I think it’s the underlying factor in all of this; I think it’s important.” (Participant 4)
Regarding the statement “in order to meet the job’s production requirements,” all the participants agreed that the job’s requirements had to be taken into consideration since they represent a reality that workers have to deal with in order to stay at work. However, they rejected the term “production” as not being applicable to all types of work (e.g., a worker on an assembly line versus a security agent), in addition to limiting the possibilities of intervention in the workplace.
“Could we simply talk about ‘requirements’ without putting all the emphasis on ‘production’? I mean, I agree with the idea of ‘requirements,’ but I think there’s a little too much emphasis on ‘production.’ But yes, the whole idea of ‘requirements’ is important.” (Participant 10)
The participants also raised the importance of including the SM concept in the general objective since it is at the core of the logic model. They felt that the notion of SM represents a broader concept that itself encompasses a problem-solving process. SM puts more emphasis on how the worker can manage and live with his health condition, unlike a problem-solving process alone, which focuses on solving a health problem.
“[It’d be better] to put the emphasis on self-management than on problem solving (...). The worker’s going to read this as ‘problem solving, so my goal is to solve my back pain problem.’ Whereas self-management focuses a little less on managing the ‘I’ve got back pain’ problem and [more on] ‘how can I live with these symptoms and succeed in managing them?’ So particularly since it’s a general objective (...) [it’s better] to emphasize self-management than problem solving.” (Participant 1)
Objective 1: Foster a functional illness representation that allows the workers to apply effective coping strategies
All participants cited the need for greater clarity in this objective, specifically concerning the term “functional illness representation.” They mentioned that the adjective “functional” is used excessively in the rehabilitation field but is not very specific. Making it more explicit would help prevent misunderstandings. During the focus group, the participants proposed a common definition.
“I’d written, ‘foster in the worker an illness representation that allows him to apply effective coping strategies.’ (...) When it comes down to it, the [idea of] ‘functional’ means that it allows (...) application of effective coping strategies. (...) But sometimes I find that ‘functional’ is used to mean all kinds of things.” (Participant 2)
Participants also stressed that the workers’ representation of their condition should allow them to move towards adopting positive coping strategies. Another point discussed was the notion of illness. For the participants, this term has a negative connotation as it focuses more on disabilities. They proposed replacing the term “illness” by “health condition,” which takes into consideration both the strengths and limitations of the worker.
“Perhaps it’s the word ‘illness’ that sounds a bit negative.” (Participant 2)
“Yes, ‘representation of the illness, of the pain and of the perceived disability.’ You know, we’re [actually] talking about (...) three negative things. (...) [But] we [really] want his condition to be represented, we want it to be represented with [both] its strength and its weaknesses. His ‘health condition,’ perhaps? Uh, uh. Rather than ‘illness [representation], maybe ‘health condition representation’?” (Participant 4)
Regarding the tasks and activities related to objective 1, the participants all agreed that they were necessary and sufficient to facilitate achievement of the objective.
Objective 2: Foster the planning of meaningful objectives and implementation of appropriate actions by the workers
To ensure that objectives 2.1 and 2.2 lead to the achievement of objective 2, the participants suggested that objective 2.1 should include having the workers prioritize their objectives and added the notion that the workers should plan measurable objectives over time. In fact, they stressed the importance of the workers establishing a timetable for planning objectives and achieving specific goals. They also pointed out that being able to prioritize one or more objectives allows workers to focus their efforts on one particular meaningful objective at a given time.
“You know, an objective, it’s all well and good to set an objective, but you know, often you also need to have a timeframe in your objective. And to say, as well, when you’re setting objectives, ‘can the patient establish a certain order of priority so that he is able to focus his efforts on things that are more important, and to give a sort of timeframe for it, or an order,’ to say ‘I’m gonna try to achieve that objective within a certain amount of time.”’ (Participant 1)
The participants also suggested adding more activities and tasks for both objectives 2.1 and 2.2. For objective 2.1, they proposed adding a task to help the workers identify and compose meaningful, realistic and measurable objectives. For objective 2.2, they proposed additions that mainly concerned equipping workers to evaluate their perceived self-efficacy and level of motivation to implement and carry out their action plan.
“So to ask for him to set objectives, (...) but also to see what his level of motivation and confidence is. In other words, [get him to assess] his motivation to achieve this [or that] objective so that he can prioritize and classify his objectives, and also [get him to assess] his level of confidence. It’s all fine and dandy to have objectives, but if they’re unrealistic, uh, that’s no good either. So it might just be a matter of including these additional steps in the tasks that involve evaluating the objectives. I mean, in the tasks to evaluate, um, you know, the presence of pre-determined objective, etc., but also to see, to evaluate motivation, the degree of motivation and confidence about reaching the set objectives.” (Participant 1)
Objective 3: Foster the appropriate use of necessary resources by the workers
The majority of the participants expressed the need to clarify objective 3 as they considered the term “necessary resources” too vague and potentially misleading. To this end, one participant made a suggestion, which was accepted by all participants regarding specifying the resources that could be used by the worker.
“I would add: the use of necessary personal, physical or organizational resources. (Proposal #15) “I support the proposal (...) It’s not redundant, it’s more specific, it’s another plus. At the same time, you’re defining what is said a little further on about resources, [where] you specify, [and here] you’re already pointing in that direction.” (Participant 11)
The participants wondered whether potential future users of the SM program (i.e., workers) should be able to use pre-existing resources, as well as develop others of their own. For example, the workers may have access to educational resources related to communication strategies but will also need to develop self-confidence in order to advocate for themselves and state their position to their employer.
“Are we [trying to encourage the worker] to use and develop his own resources or just use those of others? You know, if [we want to] encourage him to develop his own resources, I don’t know, like communication skills, he should ‘develop’ [them], not just ‘use’ [them], right? (...) Sometimes I don’t think they [workers] have everything [they need]. I think they may need to develop certain resources on their own.” (Participant 2)
Regarding the activities and tasks related to objective 3, the participants mentioned that the idea of workers acting as active collaborators with those around them to identify and make use of resources in the long term was not sufficiently present in the proposed logic model. For them to do so, workers need to be able to act as their own negotiator with the people around them (i.e., employer, co-workers and friends).
“To say that you have to equip the worker to also become, like, his own, um, negotiator in the workplace so that he can stand up for himself and then continue applying his strategies [to preserve] his health over the long term. Well, this means that there’s really a notion of negotiating that’s a little bit more than just knowing where your resources are [and] using them, [it’s more the idea of] being able, after that, to feel confident in order to continue applying them. And in fact, this is often what’s lacking, I mean, that people don’t have the self-confidence they need to continue applying [them] in the workplace.” (Participant 7)
Objective 4: Foster the assessment, by the workers, of the outcomes of their actions
For objective 4 and objectives 4.1 and 4.2, additional activities and tasks were suggested to increase the model’s plausibility. First, activities and tasks designed to equip workers to assess their level of satisfaction with the results generated by their actions were added at the participants’ request. They saw it as important to take the workers’ level of satisfaction into consideration, since workers may be satisfied with their SM of their health condition without necessarily having achieved their desired objectives. Moreover, they mentioned that the level of satisfaction assessed could also be linked to the worker’s adherence to the SM program.
“A more rational [aspect] being that of achieving the objectives, and level of satisfaction as well. Because you may have, um, you may not have achieved the objectives at all, but your level of satisfaction can be high, which is what’ll enable the person (...) to keep on trying to adhere to it after that.” (Participant 10)
During the focus group, one of the participants suggested adding a task in which the workers gather feedback from their entourage. The workers would be able to question their co-workers, friends and family about their SM of their health condition. The associated resources would include effective communication strategies for seeking constructive feedback from the right individuals. Globally, this process consists of assessing the impact of the workers’ environment on their representation of their health condition in order to facilitate their adaptation process.
“Do the tasks include asking the people in your entourage for feedback? (...) But it might be worthwhile, you know [to ask], ‘Have you noticed if any of my behaviors are good?’ You know, suggesting some ideas for possible things that [workers] can go and ask others. ‘Have you noticed if I have any behaviors that, um, seem appropriate for managing my condition?”’ (Participant 8)
However, some participants mentioned that the proposed task could induce workers to disregard their functional limitations and the margin of maneuver available to them. They stated that it could also negatively influence workers’ representation of their condition if, for example, they asked for a hostile co-worker’s opinion about their ability to self-manage, and this co-worker then blamed them for not doing their fair share of the work. Furthermore, the relevance of adding such a task was also discussed by the participants, given the absence of support from health professionals, as well as the fact that it renders more complexity to a program intended to be user-friendly.
“Personally, I find that everything in the clinical interventions is super helpful and reasonable. I wonder whether, in a self-management program aimed at [helping workers] stay at work, we aren’t going a little too far. You know, you can [try to change] lots of things. I mean, for me, as I’ve been saying right from the start, it seems to me that this is an application that should be really [quick to use], with super easy solutions for the worker.” (Participant 5)
Finally, all participants agreed on the importance of adding a task involving the workers’ self-assessment of their progress over time. It implies that the workers are able to appreciate their progress over time, which in turn motivates them to continue using the program on a regular basis.
“I think it’s really necessary, in fact, to support the participant in evaluating himself over time, because people aren’t really good at self-evaluating. They need a little push, to say [to themselves], ‘Yes, I’m on the right track.’ And to continue to be motivated to use the application.” (Participant 7)
Discussion
Through a qualitative design involving an online questionnaire and an in-person focus group, we were able to assess the plausibility of our new logic model for a SM program designed specifically to help workers who have persistent and disabling LBP stay at work. Overall, the findings revealed that making three minor modifications and seven additions would increase the model’s plausibility.
First, the participants expressed the need to incorporate the concepts of SM and margin of maneuver into the logic model. This was addressed by modifying the general objective and adding an intermediate objective. All participants agreed that the margin of maneuver represented an essential component of a SM program and it emerged as the predominant theme of the discussions. The application of the margin of maneuver in the work rehabilitation field is more recent, and there is relatively scant literature pertaining to this concept [33]. Durand et al. [32] identified the presence of a margin of maneuver as an important contributor to a sustainable RTW for workers who have been on long-term sick leave due to a MSD.
Second, our results showed the need to replace the term “illness” in objective 1 by “health condition.” “Illness” was initially chosen by the researchers to align more clearly with Leventhal et al.’s common-sense model of self-regulation of illness [27, 26]. However, according to the clinicians, “illness” has a negative connotation in that it emphasizes patients’ limitations rather than their abilities. This is also convergent with past studies that have shown that workers’ illness (or health condition) representations play a vital role in facilitating their return to work [34, 35]. The World Health Organization (WHO) proposed a definition of health as a “state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity” [36, p. 1], which has lately been criticized because of its requirement of “complete (...) well-being” [37]. By this definition, people fully capable of self-managing their chronic health condition (e.g., persistent LBP and disability) would be classified as unhealthy [37]. Yet, in work disability, workers do not necessarily define themselves as “ill” [38]. There is a need for a new definition of health, one that is based on a continuum (e.g., the SM of persistent LBP and disabilities) rather than on a dichotomy between good and bad health [39]. In fact, Huber et al. proposed a new definition of health: “the ability to adapt and self manage in the face of social, physical and emotional challenges” [39, p. 3]. This definition is more consistent with the aims of the SM model and with the observations made in this study. In fact, workers perceive themselves in a functional model of capacity/incapacity [38]. Thus, clinicians’ proposed modification to remove the term illness was therefore made to eliminate any negative connotation. This also illustrates the usefulness of assessing the model’s plausibility with experienced clinicians in work rehabilitation in preventing misinterpretations.
Our findings highlight an important added value to the study. Indeed, it shows that participants focused on using a capacity paradigm or positive psychology and user-based approaches. From a positive psychology perspective, this model has some similarities to the resilience approach, by addressing the sense of coherence [40, 41] and a goal-directed method [42]. In our model, coherence is addressed with the representation of the health condition and the goal-directed approach is supported by the common-sense model of self-regulation of illness of Leventhal et al. [35, 43].
The capacity paradigm that was put forward by the clinicians has strong ties with the model of sustainable employability [44], based on the capability approach [45], which states that sustainable employability is strongly influenced by the worker’s capabilities, functioning and freedom to be able and enabled to realize what he values in his work [44, 46]. Our logic model of a SM program to support workers stay at work is coherent with the individual resources opportunities workers can use to support their capabilities. However, in the social environment, let’s not forget that the workplace setting is a major actor in promoting capabilities with workplace resources [44]. For this aspect, occupational guidelines for managing LBP can be followed [47].
Finally, the third minor modification involved including the concept of prioritization. This modification also had a theoretical foundation. In psychology, the risk of having too many competing objectives has been seen to prevent their attainment, and consequently, to negatively influence self-efficacy [48]. Moreover, our study findings highlighted the need for objectives that are measurable over time to strengthen workers’ self-regulation process, which in turn allows them to assess the overall changes associated with their health condition. These overall changes have been shown to explain, to a significant degree, workers’ adherence to a home-exercise program for non-acute LBP [49]. As for the additions proposed by the participants to increase the logic model’s plausibility, the vast majority involved the tasks (n = 6). Only one addition concerned the activities.
The addition of one task to objective 3.1 should facilitate workers’ use of communication and negotiation strategies with their work entourage (i.e., employers, co-workers). Communication and early dialogue between main stakeholders has been shown to build better social relations with co-workers, foster a supportive environment and improve workers’ ability to do their work [50–53]. The additions of users’ self-assessment of their level of satisfaction, their obtention of feedback from their various environments and their assessment of the progression in their SM skills over time should increase the plausibility of the tasks and activities related to objective 4.1.
Our findings also allowed the integration, into objective 2.2, of users’ self-assessment of their perceived self-efficacy and motivation to accomplish their action plan and their planning of a timetable to facilitate its implementation. Perceived self-efficacy can be defined as a person’s beliefs about his capabilities to carry out an action successfully in a specific context (i.e., I can do most of my work despite the pain) [54]. By incorporating the workers’ representation of their health conditions in the logic model, it implicitly addresses the notion of perceived self-efficacy. However, the participants deemed it important to explicitly mention this concept by adding specific tasks related to it, as it represents a key aspect of SM. Another major concern voiced by the participants pertained to the notion of adherence to the SM program, which is closely related to users’ level of motivation and perceived self-efficacy. Difficulty with sustaining motivation has been identified as a major barrier to the SM of persistent pain [51].
In addition to assessing the plausibility of the logic model, the participants made recommendations for improving program adherence which included means to foster users’ motivation, a user-friendly program tailored to users’ needs, and the implementation of a reward system based on users’ accomplishments. These recommendations align with the strategies used to foster adherence to SM programs that we found in the literature [56, 57]. In fact, two studies of factors influencing adherence to a home exercise program by individuals with persistent LBP, based on their perspectives, revealed that individualized interventions, feedback, the feeling of being supported, the effectiveness of the intervention and simplified exercises that can be performed anywhere are all good strategies for fostering optimal adherence [55, 56].
Strengths and limitations
We consulted the evidence literature for the initial design of the preliminary version of our logic model and sought the opinions of experienced clinicians to assess its plausibility. These represent two different sources that should increase the credibility of the results on the assessment of the plausibility of the logic model [57]. The quality of the information obtained from a focus group is contingent upon the relevance and credibility of the participants in relation to the issue studied. We sought to recruit a variety of health professionals to enrich the results obtained. Given that a large majority of the participants were occupational therapists, this may have influenced the results of our focus group. However, we do not regard this as a bias since, in our study context, occupational therapists are the main rehabilitation professionals involved in work rehabilitation, thus they assume strong leadership roles in the promotion of a sustainable return to work [58]. Moreover, the presence of a psychologist and a physical therapist allowed to address the psychogolocial and physical aspects related to this issue. Another potential bias concerns the risk of one opinion outweighing the others. This was reduced by the active participation of other health professionals during the focus group (i.e. physical therapist and psychologist) and the use of thematic analysis. The small number of participants may be a limitation of the present study. However, convergent results and redundancy were observed regarding the main themes discussed in the focus group, suggesting that relative data saturation was achieved. We did not go back to the participants to validate our analyses after the focus group, but the facilitators regularly summarized the information discussed during the focus group to prevent any misunderstandings.
Conclusion
This study proposes a new and plausible logic model for a SM program designed specifically to help workers with persistent and disabling LBP stay at work. It was deemed essential to produce this logic model prior to developing the content and implementing a preliminary version of the SM program in this specific context. The next steps will be to assess the acceptability of the SM program with potential future users (i.e., workers suffering from persistent pain and disabilities secondary to LBP and trying to stay at work) and the feasibility of implementation in pragmatic rehabilitation settings.
Conflict of interest
None to report.
Footnotes
Acknowledgments
This work was supported by grants from the Quebec Rehabilitation Research Network (REPAR), the Institut de recherche Robert-Sauvé en santé et en sécurité au travail (IRSST) and the Ordre professionnel de la physiothérapie du Québec (OPPQ).