
Abstract
BACKGROUND:
Returning to work (RTW) is an essential goal for many stroke survivors. Currently, the prevalence of RTW post stroke in developing countries such as Jordan is unknown. Additionally, more research is required to identify factors that contribute to RTW post stroke.
OBJECTIVES:
This study aims to (1) determine the prevalence of RTW among stroke survivors in Jordan, and (2) determine the predictors of RTW from a holistic perspective using the Occupational Therapy Practice Framework (OTPF) 3rd edition.
METHODS:
Recruitment was carried out from different Jordanian hospitals and rehabilitation centers. A complete battery of outcome measures was used to reflect OTPF domains. These included outcome measures of occupations, client factors, performance skills, and context and environment. Logistic regression was used to determine factors that predicted RTW.
RESULTS:
69 participants were enrolled; 45 Males, 24 females; mean age±SD, 52.2±11.07 years. Only 29% succeeded in RTW during the first year after stroke onset. The highest percentage of RTW was among craft workers (40% ), and those who were self-employed (60% ). Of those who resumed work, 35% returned to their previous work, while 65% needed to make work modifications, or change positions or jobs. Factors that predicted higher rates of RTW were walking speed (Odds ratio (OR)=0.004, 95% confidence interval (CI)=0.00–0.55, P < 0.02), as well as absence of environmental restrictions (OR = 21.16, 95% CI = 1.91–233.5, P < 0.013).
CONCLUSIONS:
The alarming low prevalence of RTW among stroke survivors in Jordan emphasizes the essential need to develop vocational rehabilitation programs. Clinicians should pay attention to enhancing walking abilities and reducing environmental restrictions post stroke, in order to improve the occurrence of RTW.
Keywords
Introduction
Returning to work (RTW) is an essential goal for many stroke survivors, as it is an important factor in determining quality of life in this population [1]. Studies show that early RTW boost self-confidence and satisfaction and yields better health and personal-wellbeing post stroke [2, 3]. The prevalence of RTW among stroke survivors in studies varies according to country; it ranges from low prevalence (26.7% –35% ) [4–7] to high prevalence of RTW (51% –75% ) [3, 8–10]. Within this realm, determining prevalence of RTW post stroke in a country and/ or region is cru-cial to identify population needs, form policies, and allocate health care resources to this specific issue. Without knowing the prevalence of RTW in this population and its impact on a societal level, health systems and governments would not be aware of the necessities the patients need, such as support care systems and other facilities.
In this regard, the literature indicated a dearth of data on the prevalence of RTW in developing countries such as Jordan. The available evidence regarding prevalence of RTW among stroke survivors is largely based on information obtained from developed countries [3–10], where cultural, economic and health care structure differs in significant ways from those in developing countries.
In Jordan, as per most other developing countries, knowledge about stroke in general is scarce. However, it is been noted that the Middle East in general has had a significant increase in stroke incidence and death rates during the last ten years [11]. Studies by Bahou et al. [12, 13], which were conducted in Jordan, reported that the mean age of participants (61.2 years) was younger than the mean age reported in developed countries. Additionally, these studies indicated that a significant prevalence of stroke among Jordanian population younger than 55 years (41 of 200). Furthermore, vocational rehabilitation programs are under-estimated, and underutilized, thus this is a contributing factor for poor outcomes in terms of RTW after chronic illnesses. This, alongside additional cultural and socio-economic factors, may hinder the RTW rate among stroke survivors in Jordan. Therefore, this is an area that warrants further investigation.
Besides prevalence, the knowledge related to the main contributing factors that influence RTW in this population is a key for finding approaches that would facilitate RTW. Our literature search indicated that few studies investigated a wide range of predictors, which have an effect on the time of RTW after stroke occurrence [2, 14]. These factors included independency in performing activities of daily living (ADLs) and instrumental activities of daily living (IADLs) [3, 15], cognitive abilities [9, 16], emotional and psychological functions [3], motor skills [9, 17], stroke type [4] and additionally, context and environmental factors such as age and gender [2, 18], socioeconomic status [19], work type [2, 19] and workplace [20]. However, these factors were explored separately with a lack of knowledge on how they can interact with each other. The findings related to these factors were also inconclusive in most cases, due to the heterogeneity in the studied cohorts as well as the used outcome measures [2]. Moreover, certain important factors which are known to affect stroke survivors and may impact their ability and/or decision to RTW, such as urinary incontinence and social interaction, have not yet been explored in Jordan and similar countries. It is clear that this area warrants further investigation. Understanding the depth and the breadth of factors that may have an impact on early RTW post stroke is important as it can shed the light on future therapeutic approaches to facilitate patients’ RTW post stroke. Therefore, the aim of this study was to determine the prevalence of RTW among stroke survivors in Jordan and to determine the predictors of RTW among a cohort of stroke survivors from Jordan.
Methodology
Study design and participants
This study was an observational-cross sectional investigation in which 69 participants with post stroke were recruited from five hospitals (Al Bashir Hospital, Prince Faisal Bin Al Hussein Hospital, Zarqa Governmental Hospital, King Abdullah University Hospital (KAUH), and Princess Basma Educational Hospital), and two rehabilitation centers (Al- Takafol center, and Adulil Women Society for Rehabilitation), representing three different districts of Jordan (Irbid, Amman and Zarqa). Recruitment occurred between October 2018 and March 2019. The inclusion criteria included: 1) being diagnosed with a first or recurrent ischemic or hemorrhagic stroke, 2) having the stroke of at least 3 months previously (but not more than 2 years ago; to control heterogeneity and fundamental factors to influence the willingness to RTW), 3) age is ≥18 years old at the time of hospitalization (there was no upper age limit because continuing engagement in self-employed work above the official work age is a familiar phenomenon in Jordan), 4) free of any other neurological diseases or transient ischemic attack (TIA), and 5) employed [participant was an employee at the time of stroke onset (full time, part time or self-employment) either in a competitive work (i.e. paid work) or non- competitive work (i.e. household work or voluntary work)]. Participants were excluded if they had a stroke for less than three months, and retired or unemployed at stroke onset.
Face-to face interview using a battery of outcome measures was used to collect data. The data collection took about 60–90 minutes for each participant. It was carried out in a quiet, private environment and free from any distractions. The interviews were carried out by 3 research therapists (1 from each geographical area) consisting of 2 occupational therapists and 1 physical therapist with at least 5 years’ experience in providing care for stroke survivors. Two days of training program was conducted for those therapists focusing on the study objectives, the outcome measures, and the interviews protocol to ensure the consistency in carrying out the interviews and collecting data. All participants gave a written informed consent approved from the Institutional Research Committees of Jordan University of Science and Technology (HK-20180443) and ministry of health at Jordan (44A∖155∖2018).
Outcome measures
A battery of outcome measures, which relates to Occupational Therapy Practice Framework (OTPF) 3rd edition, was used. The OTPF has two parts; the domain and the process (Fig. 1). The domain includes areas that are of concern to the therapist (occupations, client factors, performance skills, performance patterns, context and environment). The process part is considered the guidance line for practitioners to provide health care services in a client-centered focus. The process part consists of three steps; intervention plan, implementation, and intervention review [21]. The OTPF provides a comprehensive umbrella that combines these factors affecting work and classifies them within domains [21].

Occupational Therapy Practice Framework (OTPF); Domain aspects and process steps. Abbreviations: ADLs; Activities of daily living. IADLs; Instrumental Activities of Daily Living.
Accordingly, outcome measures were divided into four sections: 1) occupation’s related outcome measures, 2) client factors related outcome measures, 3) performance skills related outcome measures, and finally 4) context and environment related outcome measures. Arabic versions for all tests were used and were administered in a standardized manner according to a priori prepared SOAP procedure. Order of tests was randomized between participants to avoid order-effect [22].
The primary outcome being studied is RTW post stroke onset. This aspect was evaluated using the Work Rehabilitation Questionnaire (WORQ) self- reported version, question number 4 from part one. The WORQ includes 57 items divided into two parts. The first part contains 17 questions to assess person’s work information, socio-demographics and environmental factors. While the second part includes 40 items, that provide information related to all aspects of work functioning [23]. WORQ 40 items are rated on the rating scale that ranges from (0–10). Score of zero represents no problem, a score of 10 represents a complete problem. The higher the number, indicates the greater extent of the problem [23].
Independent in performing ADLs was assessed using Barthel Index (BI). The index consists of 10 items which rated based on the amount of assista-nce required to complete each activity [24, 25]. The scores are classified as follows: 0–39 (completely dependent), 40–79 (partially dependent) and 80–100 (independent) [24].
World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2.0), is a global and generic assessment tool of health and disability. It includes 36 items from six domains to assess IADLs. The point scale ranges from 0–4 and is used to rate an individual’s performance experience of these domains. A higher score indicates a greater difficulty in clients [26–28].
Client factors: Body functions and body structures
The Montreal Cognitive Assessment (MoCA) is a 30-point screening test for different cognitive abilities [29]. The scores of MoCA range from 0 to 30; scores below 26 reveal that there is a deficit in cognitive abilities. Emotional aspects such as anxiety and depression were measured using Hospital Anxiety and Depression Scale (HADS). The HADS contains two subscales; HADS for anxiety (HADS-A) and HADS for depression (HADS-D). Each subscale includes seven questions which rated from 0–3, scores range from 0 to 21 points for each scale. The highest score reflecting large degree of depression and anxiety [30].
Urinary Incontinence (UI) was assessed using the International Consultation on Incontinence Que-stionnaire–Urinary Incontinence–Short Form (ICIQ-UI-SF). This scale evaluates the impact of UI on daily life, based on patient’s perspective [31, 32]. The total score of ICIQ-UI-SF ranges from 0 to 21 with the higher score indicates the greater feeling of burden due to UI [31]. Side of the stroke, stroke type (hemorrhage vs. ischemic) as well as duration since stroke onset were extracted from medical records.
Performance skills (motor skills and social interaction skills)
Grip strength is selected to be an indicator of muscle strength of upper extremities (UEs). It was measured using a dynamometer (Jamar-Sammons Preston, Model 5030J1) [33]. Measurement was demonstrated based on the test protocol as described by Simpson, in order to ensure consistency of application of the procedure [34]. Walking Distance was assessed using the Six- Minute Walk Test (6-MWT) [35]. Walking speed was evaluated using the Ten-Meter Walk Test (10- MWT). This test assesses walking speed in meter per second over a short distance [36].
Fatigue Severity Scale (FSS) is a 9-items questionnaire commonly used to measure the severity of pathological fatigue that effects person’s motivation, exercise, general physical function, and daily activities. Questionnaire’s items were scored from 1 to 7 [37]. The cut-off score of FSS is 4; a score greater than 4 indicates pathological fatigue [38]. Social interaction skills were assessed using WHODAS 2.0 domain 4 (getting along with people) [26, 28].
Context and environment
Context and environment variables (Age, gender, education, marital status, social support) and work type were extracted from WORQ (questions 1–17). Work type and work demand were classified according to the Jordan Standard Classification of Occupations (JSCO-04) [39]. The JSCO-04 divides jobs into 10 major groups; 1) managers, 2) professionals, 3) technicians and associated professionals, 4) Clerks, 5) service and sales worker in markets, 6) skilled agricultural, 7) craft and related work, 8) plant and machine operators, 9) elementary occupations, and 10) armed forces occupations.
Statistical analysis
Statistical analyses were performed using SPSS software version 20 (SPSS, Inc., Chicago IL, USA.). Descriptive statistics were calculated; means±SD were used for continuous variables, while frequencies were used for categorical variables. Simple binary logistic regression was used to identify potential variables associated with RTW. Variables with a significant simple binary logistic regression were included in a multiple binary logistic regression model (i.e. only significant clinical variables from the simple logistic regression were included in multiple binary logistic regression). For the multiple binary logistic regression, age, time since stroke onset and duration of rehabilitation intervention intake were additionally added to the model as covariates. Results were reported as odds ratios (OR) with the 95 % confidence interval (CI). P < 0.05 was considered as statistical significance in all analysis procedure.
Results
Study participants
Of the 136 subjects who were approached, 74 eligible stroke survivors agreed to participate in the study and provided a consent form (i.e. recruitment rate of 54.41% ). Of those 74 participants who were recruited, only 69 completed the study (i.e. retention rate 93.24% ) (Fig. 2). Table 1 demonstrates the demographic information of the included participants.
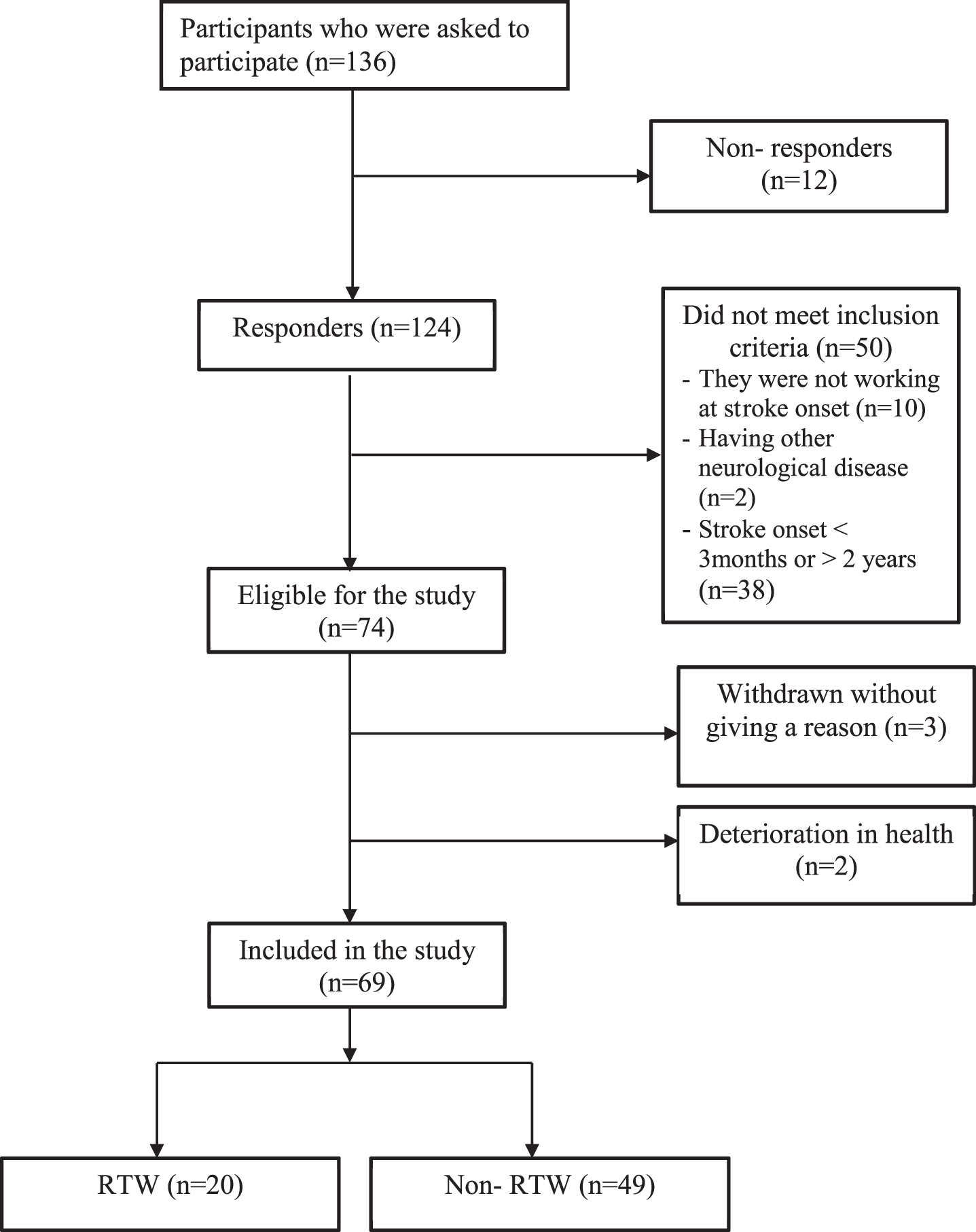
Flowchart of the study participants. Abbreviation: RTW; Return to work.
Basic characteristics for participants who enrolled in the study
SD; standard deviation. JOD; Jordanian dinar.
Participants prior to stroke onset were working either in a competitive work (n = 65; 94.2% ) or a non-competitive work (n = 4; 5.8% ). Mean years of employment was 20.78 years (SD±14.52). Work skills level (work demand) varied among participants; skilled worker level was the highest (43.5% ), while vocational work level was the lowest (4.3%) (Table 2).
Basic characteristics related to work prior stroke
RTW; Return to work. SD; Standard deviation.
Post stroke, only 29% of the studied cohort RTW; 95% of the returners were with a competitive work (Table 3). All participants who returned to work were able to resume their work during the first year post stroke, where the mean time between the stroke and the RTW was 2.5 month (SD±2.56; ranging from 1 to 12 months). The highest percentage of RTW were among craft workers, whilst the lowest rate was within the Clarks and plant and machines operators (Fig. 3). Of those who resumed work, 35% returned to their previous work, while 65% needed to make work modifications, or change positions or jobs. Amongst those who were unable to RTW, 18.4% reported the intention to engage in other work in the future (Fig. 4).
Prevalence of RTW among study population (n = 69)
Prevalence of RTW among study population (n = 69)
RTW; Return to work.
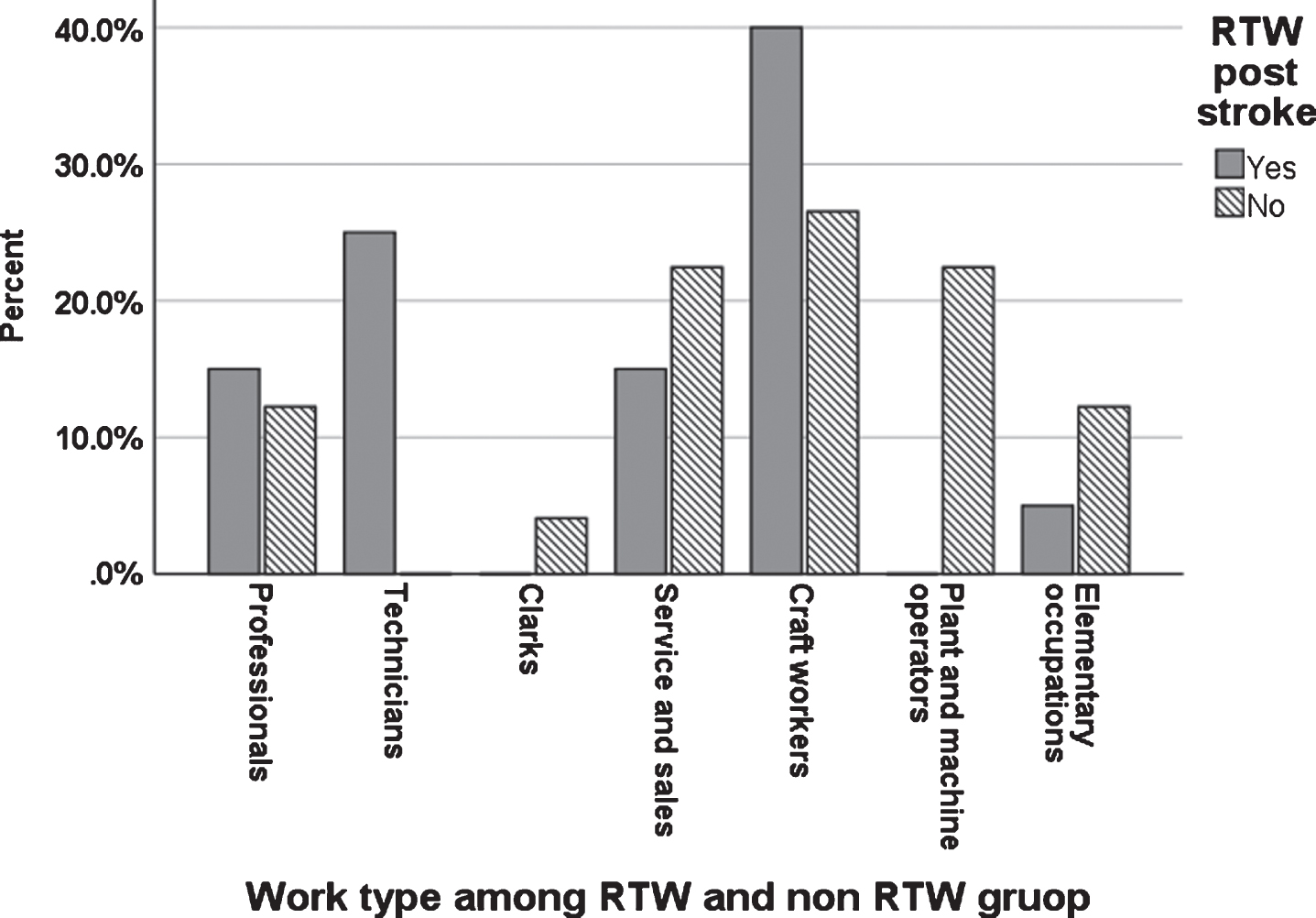
Percent of participants who successfully returned to work and who did not return to work after stroke, distributed according to work types.

The distribution of work status of participants after stroke.
Factors significantly associated with RTW in the simple binary regression analyses after adjusting for the time since the onset of stroke and the duration of rehabilitation intake post stroke are shown in Table 4. The final model of the multiple logistic regression which included all predictors that were statistically significant in the simple logistic regression, was statistically significant (χ2 = 24.86, p < .0.00), indicating that the model was able to distinguish between participants who returned to work and those who did not. The prediction value of the relationship for model as a whole was 45.3% (Nagelkerke R squared). Walking speed (OR 0.004, 95%
Simple binary logistic regression showing variables associated with RTW
Simple binary logistic regression showing variables associated with RTW
aSignificant result (P < 0.05). CI; Confidence interval. WORQ; Work Rehabilitation Questionnaire. BI; Barthel Index. ADLs; Activities of daily living. IADLs; Instrumental activities of daily living. WHODAS 2.0; World Health Organization Disability Schedule 2.0. Do.1; Domain 1 (understanding and communication). Do.2; Domain 2 (getting around). Do.3; Domain 3 (self-care). Do.4; Domain 4 (getting along with people). Do.5; Domain 5 (life activities). Do.6; Domain 6 (participation in society). MoCA; Montreal Cognitive Assessment. HADS; Hospital Anxiety and Depression Scale. ICIQ-UI-SF; International Consultation on Incontinence Questionnaire–Urinary Incontinence–Short Form. 6- MWT; Six-Minute Walk Test. 10-MWT; Ten- Meter Walk Test. CWS; Comfortable walking speed. FSS; Fatigue Severity Scale.
Multiple binary logistic regression showing variables associated with RTW post stroke
aSignificant result (P < 0.05). CI; Confidence interval. ADLs; Activities of daily living. BI; Barthel Index. WHODAS 2.0; World Health Organization Disability Schedule 2.0. Do.5; Domain 5 (life activities). 6- MWT; Six-Minute Walk Test. 10-MWT; Ten- Meter Walk Test. CWS; comfortable walking speed.
To the best of our knowledge, this is the first study to focus specifically on the prevalence of RTW among stroke survivors in Jordan and its associated factors. This study clustered a set of variables that affect RTW rate based on the OTPF model which included occupations, client factors, performance skills, and context and environment. Our findings indicated that only 29% of the studied cohort returned to work. This percentage was in line with other studies (where RTW rates ranged from 26.7% to 32.1% ) conducted in Germany, Japan, and France [4, 40]. However, this rate was less than the rate observed in other studies conducted in Australia, Sweden, India and another studies in Japan, where the rate of RTW ranged from 51% to 75% [3, 41]. There are several possible explanations for this finding.
The high rates of RTW in the studies mentioned above could be attributed to the differences in the sample size, inclusion and exclusion criteria, and the study design. The social security in Jordan provides an adequate allowance for those who are unable to RTW due to illness. The mean age of participants who were enrolled in our study was 52.4 years, with the age for most of the participants (45% ) ranged from 51 to 61 years. Though this was not stated explicitly by participants, it can be hypothesized that it is potentially more feasible for these patients to access benefits of the current legislations in Jordan and retire earlier. Additionally, the absence of vocational rehabilitation programs in Jordan may have the impacted the observed results; to our knowledge such services are a neglected area in healthcare [42] as well as in Jordan. Overall, vocational rehabilitation services are critically important as a positive facilitators for RTW post stroke [17]. Study by Hartke et al. [43] reported that most stroke survivors who received voc-ational rehabilitation services recognized their positive impact. Vocational rehabilitation services assist survivors in obtaining job, and realistically assess their vocational interest as well as providing self-esteem.
This study is consistent with other studies [2, 44] in which the chance to RTW increases over time, especially in the first year after stroke. Our findings reported that stroke survivors would either RTW early (within two months’ post stroke onset) or would delay their RTW up to one year after stroke. Similar findings were reported by Westerlind et al. [8] who found that 48.3% of stroke survivors had RTW within the first year post stroke. Our results are important not only for stroke survivors but also for work organizations and governments when establishing rules and policies of labor. In Jordan, for example, six months is the maximum duration of sick leave after an injury. Improving the knowledge of when it is the optimal time for RTW after stroke could improve our understanding of the time that should be provided to stroke survivors to receive appropriate rehabilitation treatment.
Previous studies [2, 40] found that RTW was higher for “white collar” jobs (office work), while our study demonstrated that most of returners to work were craft worker (40% ), which is considered as one type of a “blue collar” job. Although craft jobs require more motor functions, this observation can be traced back to the fact that the participants of these category in our cohort were self-employed. It can be argued that being a self-employed would have provided a better chance to these participants to make necessary adjustments and modifications at work place which facilitated RTW. Overall, the vast majority of the participants in our study who had succeeded in resuming their work have returned to modified work or to work with less requirements than the previous one. This corresponds to a previous study [45] which reported that external changes such as modifying job demands, or performing job tasks using alternative equipment and tools [42], enhance the ability of stroke survivors to RTW.
Regarding the predictors of RTW post stroke, our findings showed that absence of environmental restrictions was a predictive factor which associated positively with RTW. This finding is similar to that emerged from previous studies [17, 45]. In the current study, 87% of all participants mentioned that their environmental restrictions are the main barrier against resuming their work. These findings are supported by Brannigan et al. [17] who found that work place modifications such as work with reduced hours or less duties, and adaptation of the physical work environment enhanced the ability to RTW post stroke. Similar to a previous study [46], our study found also that while those who were self-employed had higher chances for RTW compared with those who were employed in an organization. This can be traced back to the lack of modification in work environment in such organizations. Similar to previous study [20], our findings suggest that clinician should emphasize aspects related to education and awareness of workplace community about functional limitations and restrictions of the stroke survivors. Moreover, adaptation on working hour, work status, and working demands could all be areas of concern in term of facilitating the ability to RTW among stroke survivors.
Our results showed, in accordance with other studies, that walking speed was another significant predictor on RTW post stroke [9, 17]. Larsen et al. [44] found that walking disabilities formed a main barrier to RTW. A study by Vestling et al. (1) found similar findings, where the ability to walk was significantly associated with RTW. This consistency in results might be due to the fact that walking abilities are difficult to overcome in some type of work.
Overall, clinicians should pay attention to enhance walking abilities and minimize environmental restrictions post stroke; being ambulatory, independent at discharge, as well as having lesser environmental restrictions in work environment were predictors for the ability to RTW after stroke.
Study limitations
This study is not without limitations. First, the study population should be larger to investigate a wide breadth of factors. The absence of significant association between RTW and some factors (e.g. work-related functions assessed by WORQ, cognitive abilities, depression and anxiety, UI, age, education, gender and income) may be due to the sample size. Second, this study did not specifically examine values of work as being associated with RTW [17]. Qualitative studies are essential to give a deeper understanding of RTW value and its surrounding issues. Third, in this study we did not take into consideration the phenomenon of work stability post stroke. Further studies are warranted to investigate the transition status from being not working to resume work, and the work stability among stroke survivors in long term perspective.
Conclusion
The alarming of low prevalence of RTW among stroke survivors in Jordan emphasizes the essential need to develop vocational rehabilitation programs aimed towards assessing and managing factors that have negative effects on early RTW post stroke. Overall, findings from this study may be important in determining the factors and the time that should be taken into consideration when the stroke survivor is asked to RTW. This is not only important for the client but also for the work institutions, on how to support the stroke survivors to RTW. Clinicians should pay attention to enhance walking abilities and minimize environmental restrictions post stroke; being ambulatory, dependent at discharge as well as having lesser environmental restrictions in work environment post stroke, seem to be important contributors to the successful occurrence of RTW after stroke.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Acknowledgments
The authors would like to acknowledge all the participants of the study. Acknowledgement for funding support is to Jordan University of Science and Technology (Grant number 20180443 to HK) and for the European Union; this manuscript is the academic outcome of a master student who attended a program funded project by the Erasmus+Program of the European Union entitled (Establishment of an interdisciplinary Clinical rehabilitation sciences master program at JUST JUST-CRS) (Project No: “573758-EPP-1-2016-1 JOEPPKA2-CBHE-JP”).