
Abstract
BACKGROUND:
In developing countries, the recent increase in computer-related work has considerably increased the occupational complaint of pain.
OBJECTIVE:
To examine the effects of workstation design, posture and ergonomic awareness on the prevalence of pain for a year in the upper part of the body (eyes, hands, arms, shoulders, lower back, and upper back) among IT professionals in India.
METHOD:
To investigate the association of risk factors with the prevalence of pain in different body parts, a newly designed online questionnaire titled “A Questionnaire based on ergonomics for IT Professionals” was developed. The psychometric properties of this questionnaire were tested. 110 computer office workers were recruited from IT companies from major cities in India.
RESULTS:
The confirmation of reliability and lack of redundancy of items was provided by the calculation of internal consistency (Cronbach’s alpha 0.804) and cross-validation. 60% of participants was male. Mean age was 29.73±6.09 years. The prevalence of pain for a year in the upper part of the body was 38.2%. The frequently reported pains were in the neck (22.7%), lower back area (22.7%), and eye strain (21.8%).
CONCLUSION:
It was identified that long working hours, excessive usage of smartphones, lack of exercise, incorrect workstation adjustments, and incorrect posture were the risk factors for the prevalence of pain.
Introduction
The National Association of Software and Services Companies (NASSCOM) in 2010 stated that the Indian information technology industry, including IT and IT-enabled services, has grown from USD 4 Bn in the year 1998 to USD 52 Bn in 2008. In 2019, NASSCOM stated that the revenue crossed USD 165 Bn. The need to use computers increases as computer technology advances and software and computer packages are being developed. People are an essential part of every Information Technology (IT) company and critical to delivering quality services, and hence, the performance of an organization is directly related to the health conditions of its employees. A Shikdar et al. reported that occupational health and safety problems are continuously increasing among computer users [1]. Due to increased globalization and industrial advancements, researchers have concluded that work-related musculoskeletal disorders were prevalent amongst Indian software professionals [2]. The researchers have recommended that a precise risk assessment of the computer workstation is needed.
The concept of total safety, health and productivity are directly related to various factors like physical, physiological, postural and environmental [3]. The development of musculoskeletal disorders among IT professionals are due to the awkward posture adopted by them during work [4, 5]. The computer work is sedentary and it develops static stress in the body, leading to loss of strength, flexibility, and endurance [3]. Static stress and awkward posture are developed due to lack of various physical factors –improper backrest, no armrest on the chair, improper positioning of the monitor, keyboard and mouse, and uncomfortable workstation [6–9]. It is also confirmed that the risk factors associated with constant use of computers include physical, ergonomic factors such as desk, chair and screen height and working posture [7, 10], and the use of input device such as the computer mouse [11, 12]. The prevalence of musculoskeletal symptoms among keyboard users have been reported to be as high as 76% [10]. Compu-ter use for more than 4–6 hours was the most critical predictor of work-related neck pain followed by work-related factors such as the height of the screen and posture. It was identified that there was an association between the prevalence of work-related complaints of arm, neck, and shoulder and work-related risk factors (workstation, body posture, break time and social support), duration of hours using a computer and levels of ergonomic knowledge among office workers in Malaysia [13].
There is, however, a dearth of studies reporting the prevalence of pain among Indian IT professionals. The studies that identified specific work-related factors (computer workstation design, incorrect work postures, and ergonomic awareness) that lead to pain are limited in the literature. It was also noticed that with the advancement in technology, IT professionals use different devices like desktops, laptops, tablets, or smartphones at work.
The research questions thus put forth for this study were as follows: Which type of device was predominantly used at work and home, and which device influenced more pain? What was the 1-year prevalence of pain in the upper part of the body among the participants, and which upper part body region frequently reported pain? What were the deficiencies in computer workstation design that led to pain in the upper part of the body? What were the current risk factors (among daily computer usage, duration of the occupation, type of device at work, ergonomic information and training, no habit of exercise and age) that caused pain in the upper part of the body? What were the incorrect postures while working with the monitor, keyboard, mouse, armrest, wrist rest, and chair that led to pain in the upper part of the body?
The main aim of this study was to identify the current risk factors for occupational pain related with incorrect work habits, the awareness of ergonomic practices, computer unit postures and effects of workstation design among Indian IT employees.
Methods
Study participants
The survey was carried out between May 2016 and November 2016 [14]. One hundred and fifty computer office workers from Indian multinational IT companies from major cities like Delhi, Hyderabad, Chennai, Bangalore, and Mysore were invited for this study. The online questionnaire was shared with the alumni of the Karunya Institute of Technology and Sciences working in Indian IT companies via emails and social media. Informed consent was obtained from each participant. The respondents in this survey were included based on the following criteria (1) Working in the current position for at least one year (2) spends at least two hours per day working on the computer; (3) not afflicted from sickness and injury affecting the musculoskeletal system; (4) with no history of surgery in the upper musculoskeletal part of the body. One hundred and ten participants who satisfied the inclusion criteria were considered for the study.
Study instruments
In the recent past, it was noticed that IT employees predominantly used desktops as well as laptops in their workplace. It was found from the literature that there were different questionnaires designed and developed to acquire data from the computer users to assess physical, psychosocial and environmental factors, and demographic characteristics of the computer workstation. Moreover, there were other questionnaires developed to find the complaint of pain in different body regions. Also, instead of asking the computer users to fill 2 or 3 questionnaires, a new on-line questionnaire was designed to collect demogra-phic, employment, physical workstation, complaints of pain and work environment information. Moreover, very few online questionnaires were available to assess a computer workstation and the prevalence of pain. Eight questions were added to assess the adjustability feature of the armrest, monitor, keybo-ard tray and mouse tray. Five questions were added on the design of the wrist pad. Eight questions were added to acquire information on the amount of time spent per day on coding/typing, computer aided design, animation, meetings, video conferencing, tea-ching, reading and talking on the phone.
An online questionnaire titled “A Questionnaire based on ergonomics for IT Professionals (QEIP)” was developed to collect the most accurate and re-levant information to know the occupational health of employees of offices, banks, and IT sector. The validated tool Maastricht Upper Extremity Questionnaire (MUEQ) [15] and the Occupational Safety and Health Administration (OSHA) checklist (USA) (https://www.osha.gov/SLTC/etools/computerworkstations/checklist_evaluation.html) were referred to formulate this customized questionnaire. This Questionnaire was designed to identify pain experienced in the upper part of the body and to find the risk factors for the prevalence of pain. According to the time study done, it took approximately 15 minutes to fill out the questionnaire.
The pilot study was conducted on 30 employees, and the reliability test was carried out on the newly designed questionnaire. The Cronbach’s Alpha was found to be acceptable (Cronbach’s Alpha = 0.804). Based on the review by experts and the results of the pilot study, redundant and irrelevant questions were removed, and some of the questions were re-framed.
The QEIP is a 98-item survey. Five sections co-ver the following areas: demographic informat-ion, employment information, physical work station characteristics, ergonomic injury-related symptoms (complaints), and work environment. The first section (Demographic Information) consisted of questions related to the demographics of the computer user. The second section, ‘employment information’ covered questions related to the duration of occupation, daily computer usage, type of computer tasks performed, and the nature of breaks during work. A set of questions was used in this section to evaluate the awareness of ergonomic principles used in the workplace by the IT employees. The third section of the QEIP questionnaire, ‘Physical Work Station Characteristics’ is a 40-item self-report dichotomous checklist, which evaluates the available workstation equipment and risk factors related to workstation postures. This section identified specific risks for symptoms related to posture of the neck, head, shoulders, trunk, and seating issues. This section of the questionnaire also recognized risks associated with the position of the keyboard, mouse, monitor, armrest and wrist rest, and lack of hands-free telephone headset a document holder. The fourth section, ‘ergonomic injury-related symptoms (complaints)’ comprises dichotomous questions related to a complaint of pain in the upper part of the body and severity of pain. A set of questions related to the type of treatment received and the duration of exercise were also included in this section. The fifth section, ‘work environment’ includes dichotomous questions related to the environment (temperature, ventilation, illumination, and noise) of the computer workstation.
The QEIP evaluates risk factors in the following domains: gender, daily computer usage, duration of the occupation, type of device, ergonomic information, ergonomic training, exercise, age, workstation, and body posture. The dependent variable was the incidence of pain in the neck, eye, upper and lower back, right and left shoulder, elbow, upper arm, forearm and hands prevailing for at-least seven days over the past one year. The analysis of risk factors was performed for each area autonomously.
Statistical methods
Characteristics of the study population
Characteristics of the study population
Note. The demographics of the respondents are listed.
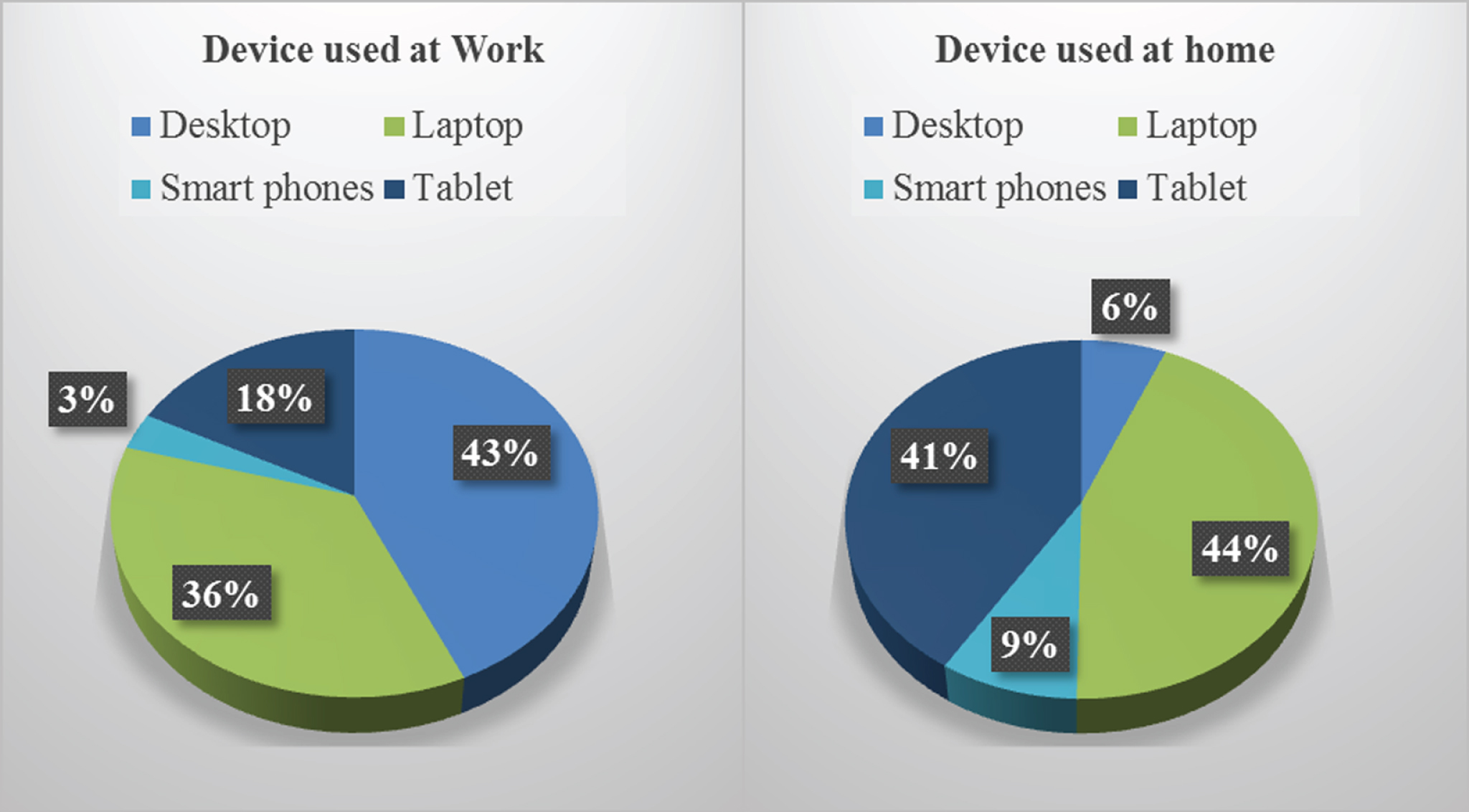
The percentage of devices predominantly used at work and home are represented.
Independent sample t-test was carried out to find the association between pain and gender. One Way ANOVA test was carried out to examine the relationship of risk factors i.e., daily computer usage, duration of occupation, type of device, ergonomic information, ergonomic training, exercise, and age separately with pain in the upper part of the body. Chi-square test was conducted to examine the association of the design of computer workstation (Monitor, Keyboard, mouse, chair, armrest, and wrist rest) and body posture with pain in different body regions. The complete data was entered and cross-verified for consistency. SPSS version 20.0 (IBM SPSS Statistics Version 20.0) statistical software package was used to analyze the data, and p < 0.05 was considered statistically significant.
Demographic characteristics
The sample size was 110 participants. Mean age was 29.73±6.09 years (range 21–58 years), and 60% responses were from male candidates. The age of 59% of the study population was between 21–30 years, out of which 64.6% was males, and 35.5% was females. 97.3% of the study population was right-handed. A majority of the study population was employed between 1–5 years (93.6%) and 6.4% of them had already worked between 6–10 years in their current position. 61.2% of the male respondents worked 1–5 hours per day on a computer, compared to 38.8% of the female participants. The demographic characteristics of the study population are summarized in Table 1.
Physical workstation characteristics
The devices which were predominantly used at work were desktop (43%) and laptops (36%) whereas the devices which were predominantly used at home were laptops (44%) and tablets (41%) (Fig. 1). Out of the 72 respondents who used laptops, 33.3% connected a keyboard, 58.3% connected a mouse, 15.2% were able to adjust the plugged-in keyboard and mouse height and 69.4 % placed their laptops on a platform so that the display was at a comfortable height as shown in Fig. 2.
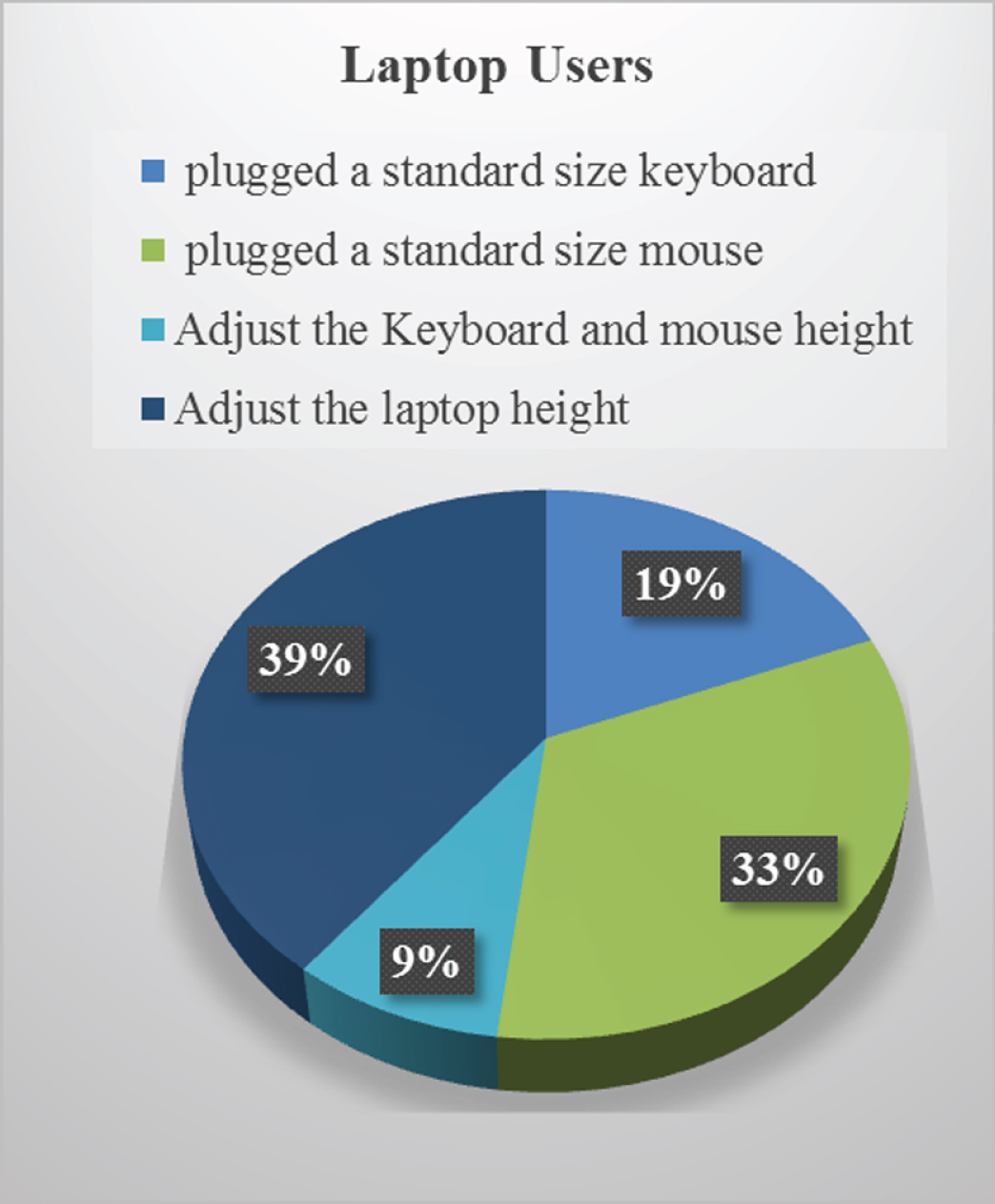
The percentage of the respondents who worked on laptops connected with a standard size keyboard and mouse used a height adjustable keyboard tray and mouse tray, and placed their laptops on a platform so that the display was at a comfortable height are shown.
The 1-year prevalence of pain in eye, arm, neck, shoulder, and back among the participants was 38.2%. Complaint of pain in males and females was 34.85% and 43.18% respectively. The frequently reported pain was in the neck (22.7%), lower back (22.7%), eye strain (21.8%), upper back (13.6%) and shoulder (12.7%) as presented in Fig. 3. The participants were divided into two sub-groups based on their complaints of pain in upper extremities: (1) mild cases: subjects who reported that the pain disappeared after a short rest; (2) severe cases: subjects who reported that the pain continued after work and even after a short rest. Most of the subjects in the study population reporting pain had mild symptoms (74%), whereas only 26% complained of severe symptoms.
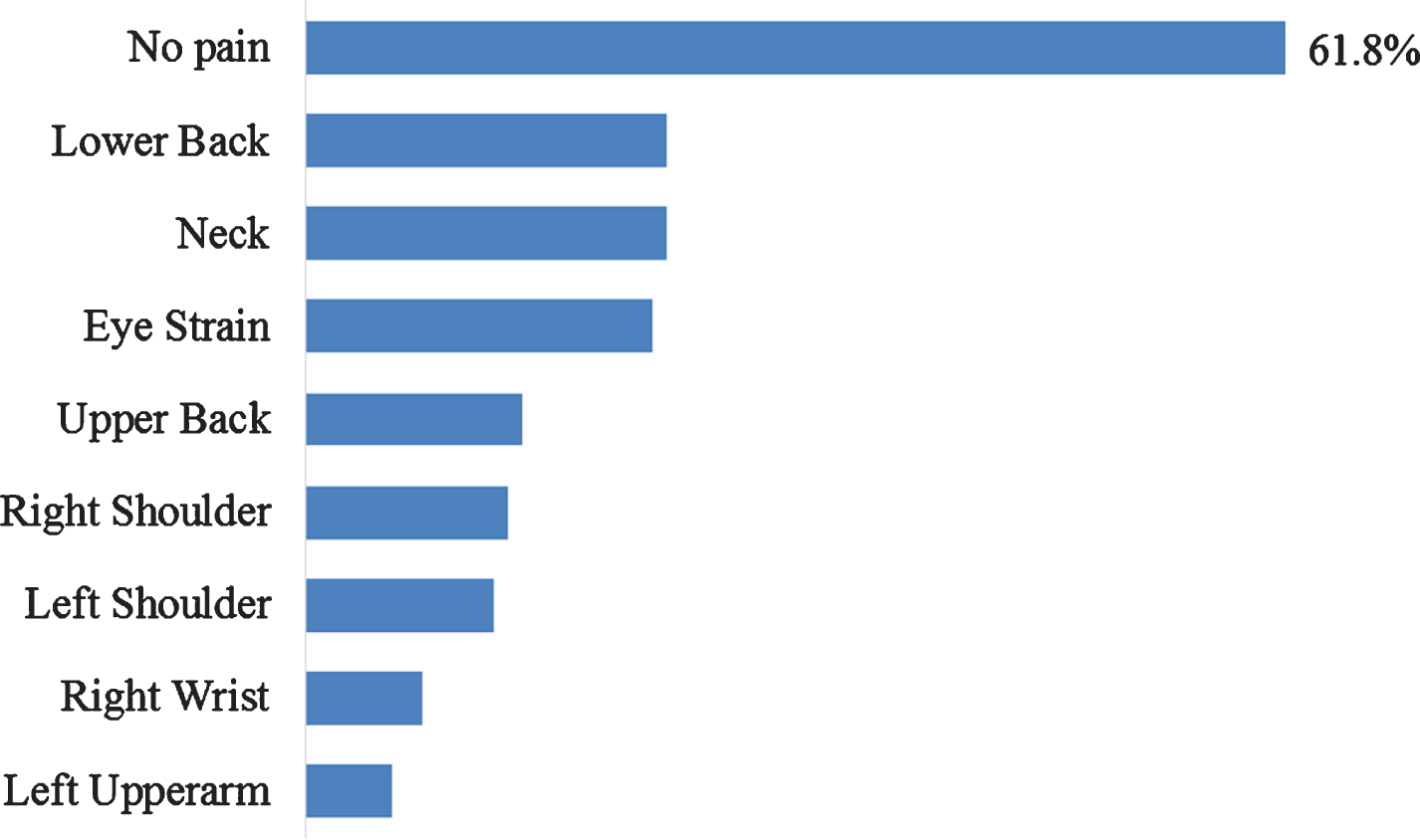
The percentages of the 1-year prevalence of pain in different body regions among the participants are represented.
The general symptoms among those with complaints in the upper musculoskeletal part of the body was pain (83.3%), fatigue and exhaustion (90.4%), stiffness (95.2%), numbness (95.2%) and tingling sensation (92.8%) and weakness (92.8%). Among the participants with complaints, 42.8% (n = 42) had taken treatment from a hospital for their illnesses. The treatment included physiotherapy in 28.5%, medication in 9.5% and other treatments in 4.7%. In addition, 28% (n = 12) reported complaints was absenteeism from work and for n = 34 reported complaints (Work-38%, Leisure-42%, Work and Leisure-31%), the normal activities were affected.
Risk factors verses pain complaints
Risk factors verses pain complaints
Note. The p value obtained from the independent sample t test and one-way ANOVA test done on the risk factors for the prevalence of pain are listed and a value of p < 0.05 is considered significant and p < 0.01 is considered highly significant.*p<0.05. **p<0.01.
Deficiencies identified in computer workstation design
The employees who worked with wrongly adjusted office equipment were at larger risk of developing job-related musculoskeletal disorders. The ergono-mic principles were not known to many of the emp-loyees. Since the anthropometry data differed from place to place, it was required to find the condi-tion of the working environment and deviations from the standard ergonomics practices. The workstation was evaluated with the modified OSHA VDT workstation checklist which was integrated into the newly designed questionnaire QEIP in the section called “Physical Workstation Characteristics,” and the issues faced in the workstation are prioritized and presented in Table 3. As shown in Table 3, the leading deficits recognized in computer unit design with respect to an IT employee were; mouse height was not adjustable (67.30%), wrist rest was not pro-vided (60.00%), feet were not supported by a stable footrest (58.20%), difficulty in keeping trunk perpendicular (40.00%), keyboard height was not adj-ustable (36.40%), foot was not resting on the ground (33.60%), awkward positions of shoulders and arm during computer task (31.80%), absence of armrests or non-adjustable height of the armrest (31.80%) and elbow and upper arm away from the trunk while working (29.10%). The above-mentioned deficiencies in workstation design usually led to pain and discomfort in the neck, shoulders, forearm, and wrists.
Monitor position verses pain in different body regions
Monitor position verses pain in different body regions
Note. This table shows the association between the design of monitor with pain in the respective body regions mentioned in the column heading (eye, neck, lower back, shoulder, upper/lower arm, wrist, and hand). *p<0.05. **p<0.01.
An independent sample t-test was conducted to find the association between pain experienced and gender. The p = 0.308 (p > .05) (Table 2), indicated that males and females have a similar prevalence of pain. A One Way ANOVA test was carried out to examine the relationship of daily computer usage with pain in the upper part of the body. As shown in Table 2, using the computer for a long time per day led to significant pain in the upper part of the body (p = 0.029). The 1-year prevalence of pain for those who worked on desktops at work was 38.81%, on laptops was 37.50%, on tablets was 20% and on smartphones was 55.56%. It was found from Table 2 that the p-value gained for those working on the smartphone was 0.03, which was statistically significant (p < 0.05). This indicated that people who predominantly worked on smartphones were more inclined to discomfort and pain. From Table 2, it was found that the p-value for the people who did not exercise regularly was 0.003, which was significant. This indicated that the people who exercised regularly had less pain in the upper part of the body. It was also found from Table 2 that, the association between duration of the occupation, ergonomic information, ergonomic training, and age with pain were not significantly associated with pain. This indicated that the main risk factors for the pain were long hours of working, regular usage of smartphone, and lack of regular exercise.
Design of the chair verses pain in different body regions
Note. The association between the design of the chair with pain in the respective body regions mentioned in the column heading (eye, neck, and wrist) is presented in this table. *p<0.05. **p<0.01.
Position of keyboard verses pain in different body regions
Note. The association between the design of a keyboard stand with pain in the respective body regions mentioned in the column heading (eye, upper back, and right and left shoulder) is presented in this table. *p<0.05. **p<0.01.
From Table 4, through Chi-square statistical test, it was reported that the significant p-value (p < .05) confirms the association between the position of the monitor and pain in pain in the upper part of the body. As shown in Table 4, the monitor placed far from the user, led to pain in the neck and shoulders and the monitor placed not directly in front of the user while working, led to pain in eye, neck, lower back, shoulders, upper and lower arm, wrist, and hand.
Position and design of the mouse verses pain in different body regions
Position and design of the mouse verses pain in different body regions
Note. The association between the design of the mouse with pain in the respective body regions mentioned in the column heading (right shoulder, upper arm, wrist, and hand) is presented in this table. *p<0.05. **p<0.01.
The association between the design of chair and pain in the upper part of the body was found by performing the Chi-square test, and the p values obtained were listed in Table 5. It was inferred from Table 5 that IT professionals using chairs with non-adjustable height and chairs not fitted on rollers reported pain in eye, neck, and wrist. In Table 3, only 13.6 % of the users were using a chair with non-supportive backrest. Hence, the majority of the IT professionals were provided with a chair with backrest supporting the lower back.
Risk factors related to keyboard position
The association between the position of keyboard and pain in the upper part of the body was found by performing the Chi-square test, and the p values obtained were listed in Table 6. The researchers inferred from Table 6 that the users having no provision to adjust the height of the keyboard developed pain in the eye, upper back, and left and right shoulders. It was also indicated with no provision to move the keyboard in the left-right, and front-back directions to the user, led to pain in shoulders.
Risk factors related to the position and design of the mouse
A Chi-square test was carried out to find the association between the position and design of the mouse to the user and the pain experienced by the user in pain in the upper part of the body. From Table 7, it was understood that an unfitting variety of the design of the mouse would also lead to pain in right upper arm, wrist, and hand. It was also inferred that the mouse placed in incorrect position led to the right wrist and hand pain. Furthermore, the researchers inferred from Table 7 that the users having no provision to adjust the height of the mouse developed pain in right shoulder and wrist. It was also made known that no provision to adjust the position of the mouse in different directions (front, back, left and right) led to pain in the right upper arm.
Risk factors related to the design of the armrest
The statistical test, Chi-square test was carried out to find the association between the design of armrest and the pain experienced by the user in different body parts. From Table 8, it was found that since the p-value is significant (p < .05), working on a computer with arms not supported can lead to pain in the left and right wrist as well as the hand.
Risk factors related to the design of wrist rest
From the Table 9, through the Chi-square statistical test, it was reported that the significant p-value (p < .05) confirms the association between the design of wrist rest and pain in some of the body regions. As shown in Table 9, it indicated that improper placement of wrist rest and using a wrist rest filled with beads developed pain in the left and right forearm. It can also be seen from Table 9 that wrist resting on sharp edge led to pain in left and right hand and wrist.
Design of arm rest verses pain in different body regions
Design of arm rest verses pain in different body regions
Note. The association between the design of arm rest with pain in the respective body regions mentioned in the column heading (left and right upper arm, wrist, and hand) is presented in this table. *p<0.05. **p<0.01.
Design of wrist rest verses pain in different body regions
Note. ‘*’ denotes p < .05 which indicates that there was an association between the design of wrist rest with pain in the respective body regions mentioned in the column heading (left and right forearm, hand and wrist) is presented in this table. Designs with no provision for wrist rest and gel-filled wrist rests were insignificant and hence were not included in the table. *p<0.05. **p<0.01.
Posture verses pain in different body regions
Note. The association between the incorrect posture with pain in the respective body regions mentioned in the column heading (eye, neck, lower back, shoulder, upper/lower arm, wrist, and hand) is presented in this table. *p<0.05. **p<0.01.
The association between the incorrect posture and pain in different body regions was obtained by conducting chi-square test. The p-value obtained less than 0.05 is listed in Table 10. This analysis showed that the posture head and neck bent while working and shoulders and upper arms stretched forward or elevated led to pain in the entire upper part of the body. The posture trunk leaning forward or backward led to pain in lower back, shoulder, arm, wrist, and hand.
Discussion
The present study investigated the correlations between risk factors and the prevalence of self-rep-orted pain among computer professionals from India.
The observed 1-year prevalence of pain in eye, arm, neck, shoulder, and back among the participants was 38.2%. It was also found that the self-reported pain in the eye, neck, and back was much higher than the forearm and hand region. According to the studies conducted in Sudan, Dutch, Greece, Selangor and Kuala Lumpur, Estonian, Turkey, India, Ghana and Australia, neck, back, and shoulder pains were the most frequently reported complaints [17–22]. The present study also showed that there was an increase in health care expenses, as 42.8% took treatment from hospitals for their health issues, while 28% reported absenteeism from work. Priyanga Ranasinghe et al. also reported an increase in medical expenses, as 22.7% had taken treatment from health care professionals for their ailments [18].
It was observed that computer professionals predominantly used desktops and laptops at work and used laptops and smartphones at home. The observed prevalence of pain in the usage of a smartphone at work was 55.56%, which was much higher than that of desktop, laptop, and tablets. It was also observed that the prevalence of pain for the usage of the laptop at home was 42.11 %, which was much higher than the other devices. This indicated that computer users tend to position their laptop in their homes incorrectly.
Previous studies confirmed that pain in upper mus-culoskeletal extremity among computer office workers was related with both physical and psychosocial risk factors [17–22]. The present study showed that long hours of work and no habit of exercise were significantly associated with the prevalence of pain. The results also showed an association between non- neutral postures (bent head and neck, elevated/stretched shoulders, non-supported arm, and twisted trunk) and pain experienced among IT professionals in India. This finding was consistent with previous studies that reported the correlation of pain and incorrect posture of the neck, upper arm, and wrist among IT professionals in India [4, 5].
The issues faced in the workstation were prioritized and presented in Table 3. Based on the priority of the issues in workstation evaluation, the correlation between the issues and the prevalence of pain in different body regions was found in this study and presented from the Table 4 to Table 10. From the Table 4, it was inferred that not placing the monitor directly in front of the user-led to pain in the eye, neck, lower back, shoulder, lower arm, wrist, and hand. Similarly, the monitor distance being too far led to pain in the neck and shoulder. Szeto and Sham [23] also found that computer professionals working in different oblique positions (central screen position, angled left position, and angled right position) of the monitor led to mutual rotation and side flexion of the head and neck and also a significant increase in the muscle activity of the ipsilateral cervical erector spinae and contralateral upper trapezius. The reason for the incorrect placement of the monitor could be due to the usage of telephone or referring to a document while working on the computer. From Table 3, 69% of cases did not use a document holder, and 56.40% did not use a headset for the telephones. Hence, it is recommended that usage of headset and placement of a document holder next to the monitor to refer the required document would help to maintain neutral postures of the neck, back, shoulders and arm and thus ultimately reduce pain [24].
From Table 5, it was found that users not seated on height-adjustable chairs fitted on rollers experienced pain in the eye, neck, and wrist. It was also observed that the majority of IT professionals used adjustable height chairs fitted on rollers and were having lumbar support backrest.
The usage of keyboard and other pointing devices caused sustained exposure to force repetition and non-neutral postures of the upper extremity [6]. From Table 6, it was found that IT professionals using the computer workstation with no provision to adjust the position of keyboard-led to pain in the eye, upper back and shoulder which was consistent with previous studies done. From Table 7, it was examined that the input device (Keyboard and mouse) placed improperly led to pain in the wrist and hand. The experimental study done by Kotani et al. [6] sugges-ted that a reduction in non- neutral postures of the wrist was observed as the keyboard was moved away from the user and it was noted that the presence of a large pad was needed to keep the wrist from extending during the task. From Table 7, it was found that using a non-suitable type of input device led to an increase in pain in the upper arm, hand, and wrist. The pressure at the carpal tunnel and muscle fatigue for an ergonomic mouse were evaluated and found less fatiguing [8].
Shoulder pain played an essential role in the co-ordination of wrist flexors and extensors during computer mouse work [25]. The present study also confirmed that the non-adjustment of the position of the mouse led to increased pain in the wrist, upper arm, and shoulder (Table 7). It is recommended that the discomfort and fatigue for right-handed computer mouse could be reduced by placing the mouse and keyboard at the same height and a distance of 13 cm from the midpoint of the right edge of the keyboard and a little distance away along the y-direction (around 5 cm) [26].
From Table 8, it was found that the non-supportive armrest led to increased pain in the wrist and hand. From Table 9, it was found that improper placement of wrist rest and using a poor design of wrist rest (beaded) led to increased pain in the forearm. Likewise, wrist resting on sharp edges led to pain in the hand and wrist. As per the investigations done by Nag et al. [8], forearm support can considerably reduce electromyography activity of the bilateral forearm and shoulder muscles. Furthermore, gel-filled wrist rest in comparison with the bead packed wrist rest can reduce the load on the forearm muscle [8]. Another study confirmed that the forearm support could reduce shoulder muscle activity and torque and palm support can lower wrist extension and applied forces to the mousepad [27]. In the current study, there was significantly (p < .05) high discomfort level due to lack of wrist/palm rest.
The study showed that it is essential to use adj-ustable workstations to reduce pain in eyes, arms, necks, shoulders, and back. It was also found that ergonomic knowledge and training were not significantly related to the pain experienced by the users. From the present analysis, it is suggested that having only ergonomic intervention can be less effective. It was found by Feuerstein et al. that ergonomic intervention, along with job stress management, was highly effective [28].
It was also observed that the 1-year prevalence of pain among the participants was 38.2%, which was less compared to the previous studies done [2, 29]. It was also noticed that the majority of participants were provided with suitable adjustable works-tations. It was observed that despite having some ergonomic knowledge to adjust the workstation acc-ording to ergonomic principles and having an adj-ustable workstation, there was still a prevalence of pain. Previous studies suggested that the risk factors related for the growth of musculoskeletal ailments were due to psychosocial risk factors (excessive workload, time pressure, and absence of social support from colleagues and superiors) [4, 30]. Hence, it can be suggested that because of psychosocial risk factors, the computer users were unable to adjust their workstation as per the ergonomic guidelines. The significant interventions done by various researchers to reduce pain in computer workers were mainly ergonomic training [31–33], software to give reminders to the users of the incorrect posture adapted (surveillance system) [34, 35], exercise training [36], sit-stand workstations [37, 38], dynamic workstations to reduce sedentary work [39–43], multi-position workstation [44], taking active breaks [45], an automated monitor [46] and wearable posture correction sensor on head and neck posture [47] to adjust the monitor position as per the seated height of users. The challenge faced by the researchers with the surveillance system was that it could only be used as a reminder and the computer users need to depend on themselves to adjust their posture to reduce myopia, backbone/neck diseases, and other health problems. Wu et al. studied the posture enhancement of users by developing and evaluating a system called ActiveErgo, which automatically adjusts the monitor height to the seated height of the user [46]. They have confirmed that this system improves the posture compared to manual configuration and helps more users significantly to fully meet ergonomics guidelines. Hence, in order to further improve occupational health of IT employees, it was suggested to use a smart workstation which could automatically adjust the position of the chair, keyboard, mouse and forearm rest based on the user’s anthropometric data and as per ergonomic guidelines to maintain a neutral posture.
The present study has several limitations, and the results must be considered based on it. The participants found the 98-item survey too long. There could be bias in reporting of complaints in the past 12 months. The effect of psychosocial risk factors was not included in the present study. Further studies might improve self-reports on work postures and evaluation of the design of workstation by conducting an experimental study using high precision instruments like electrogoniometers and 3-D motion analysis of infrared camera system to detect work postures continuously. A similar study can be done among the IT professionals in North India to validate further or compare the results.
Potential applications of this research include knowledge of the most reported upper body region pain and the investigations of the risk factors cau-sing pain. This will help the researchers, workstation designers, and computer users to carry out appropriate ergonomic interventions to improve the occupational health of IT employees.
Conclusion
The current risk factors for complaints of pain related to computer workstation design, bad work postures, and ergonomic awareness among Indian employees are identified in this study.
Both desktops (43%) and laptops (36%) were predominantly used at work and laptops (44%), and tablets (41%) are predominantly used at home in India.
It was observed that using computers for long hours per day led to pain in the upper part of the body. It was found that people who predominantly worked on smartphones were more prone to discomfort and pain. It was also observed that the people who did re-gular exercise had less pain in the upper part of the body.
It was ascertained that despite having well des-igned and adjustable workstations and good erg-onomic knowledge; pain was prevalent among IT employees. Therefore, in order to improve occupational health of IT employees, it was suggested to use a smart workstation which could automatically adjust the position of the chair, keyboard, mouse and forearm rest based on the user’s anthropometric data and as per ergonomic guidelines to maintain a neutral posture.
Conflict of interest
None to report.
Funding
There was no funding available to carry out this work.