
Abstract
BACKGROUND:
Development of clinical practice at a Danish neurorehabilitation centre was delegated to a group of health professional developers. Their job function lacked conceptual foundation, and it was unclear how their working tasks contributed to evidence-based practice.
OBJECTIVE:
Conceptual clarification of the job function and pattern analysis of activity distributions for health professional developers.
METHODS:
Health professional developers kept continuous time geographical diaries for two weeks. Meaningful categories were subtracted through content analysis. Patterns were analysed within activity distributions with regards to evidence-based practice.
RESULTS:
A total of 213 diaries were collected from 21 health professional developers of three professions (physiotherapists, occupational therapists and nurses). Each participant reported 6–13 workdays (median 10 days). Eleven main categories of work tasks emerged with 42 subcategories. Overall, 7% of total time reported was spent on external knowledge, with minimal variation between professions and contractual time allocation.
CONCLUSION:
Conceptual clarification of work tasks was established for health professional developers. Their work activity distributions contributed mainly to maintenance of existing level of professional knowledge rather than to implementation of new knowledge, which did not fulfil the intended responsibility for development of evidence-based practice. Educational competence boost and data-driven change of organisation structure was recommended.
Introduction
Evidence-based practice in rehabilitation
Healthcare organisations such as hospitals and rehabilitation centres increasingly use a combination of qualitative and quantitative data in clinical decision-making, impact measurement and qualityassessment. This applies to the core task of treatment and care for patients as evidence-based practice [1] as well as to performance-based management of healthcare professionals [2]. Evidence-based practice has been defined by Sackett et al. as the “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients” [1]. This requires a combination of the best available external clinical evidence from research as well as individual expertise and reasoning [1]. Such evidence from rehabilitation settings is increasingly published to support informed decision-making in clinical practice development. A doubling of publications on the term “rehabilitation” between 2009 and 2019 to more than 36,000 articles on Pubmed [3] exemplifies a rise in so-called external evidence. This calls for extensive translation of knowledge from research into clinical practice. A recent Danish study by Kristensen and Hounsgaard found that appointed facilitators can be key stakeholders and important elements in anchoring this knowledge translation in clinical practice [4].
Hospitals and rehabilitation centres are knowledge-intensive, specialised units with a continuous focus on education and training [5]. In comparisonto the traditional biomedical paradigm, the rehabilitation approach is a relatively new mindset in hospital settings in modern healthcare [6]. As described by Wade [7], the rehabilitation paradigm is a valuablecontribution to general healthcare that supports thechange in rationale from a pathogenetic to a saluto-genetic approach, combining multi-disciplinary interventions, active patient involvement and evidence-based medicine [6]. To be leading specialists of such complex in-hospital services, rehabilitation centres require competent healthcare professionals to develop clinical practice through translation of scientific and clinical evidence into daily practice. A practice development that must match the highest standard of available evidence on an international level. Proctor et al. have clarified that it is important to ensure treatment effectiveness and quality of care through successful implementation of new treatments, practices, and services [8]. This means that if new knowledge is not systematically applied in daily work routines through practice development within an organisation, it is likely to adversely affect effectiveness of treatment and quality of care. Further, the complexity of a biopsychosocial approach and multi-disciplinary setting calls for flexible and agile knowledge development [9], which must always be balanced with direct patient-related tasks in busy hospital settings with high performance standards.
Setting
Hammel Neurorehabilitation Centre and University Research Clinic (HNURC) delivers a free public rehabilitation service. It has served as a hospital since 1894 and as a rehabilitation centre since 1998 [10]. Management and healthcare professionals have contributed to the organisational growth into the current status as a University Research Centre with acombined focus on clinical development, education and research [11, 12]. The clinical rehabilitation setting with team coordinated, patient-centred, and multi-disciplinary approach to promote active patient participation is described by Pallesen et al. [13]. It is organisationally structured with a multi-disciplinary top management and delegated responsibility to local management in eight clinics. Management and health professional developers share responsibility of providing an evidence-based rehabilitation service of the highest possible quality.
Health professional developers in rehabilitation
At HNURC, a group of health care professionals of three professions (occupational therapists, physiotherapists and nurses) are responsible for clinical practice development. As such, they have an additional function with regards to development respon-sibility specified in their contract of employment. They will in this article be referred to as HPDs – health professional developers. All HPDs have multiple functions and tasks. They work with hands-on rehabilitation of patients on an equal footing with other clinicians. In addition, they carry out clinical development tasks at the centre such as describing guidelines for daily treatment routines and training of new staff members. The HPDs perform clinical development tasks according to their individual role description.Some have one-third of their time allocated to hands-on rehabilitation and two-thirds of their time to clinical development. Others have an equal but opp-osite contractual time allocation.
The intention behind the HPDs job function was to delegate responsibility of professional development within the rehabilitation centre to an expert group with top level of competence within specialised areas of neurorehabilitation. The responsibilities and mandatory tasks for the HPDs was described within the organisation as: 1) representative participation at meetings to coordinate overall time consumption for clinical development projects, and 2) (unspecified) tasks appointed directly by local management. It was further specified, 3) that one day a week (Wednesdays) should be reserved for tasks unrelated to patient treatment or care. With only these few official requirements, the individual choices and tailored task balance allowed for flexible solutions within each clinic in accordance with varying personal preferences, time allocation keys, managerial expectations and local work cultures. However, it created conceptual confusion of the tasks performed during daily work routines, and it led to uncertainty of who was responsible for which development related task, and even to what extent specific tasks were taken care of or contributed to evidence-based practice.
Objective
The aim of this study was to conceptualise the job function of health professional developers at HNURC and to study patterns of activity distributions with regards to evidence-based practice.
Design
Method
Within the framework of time geography, activities can be categorised to study occupational patterns [14]. The time geography methodology is a mixed-method approach based on diaries filled out by individuals who report the timeframe for their daily activities in their own words. The time geography approach offers potential to investigate interaction between the diarist and other people, activities and places. In this study, it was purposeful to study the conceptualisation of work tasks and their relative time distributions, and further analysis of people and places was not undertaken. A time geographical analysis contains the combined qualities of both personally reported experience and quantified inventories. It has been used in different settings to assess work patterns [15–17], and includes software to code and quantify activities to visualise time distribution of activities as a total sum of time, i.e. during a 24-hour timespan or a full work day [18].
A time geographical study was applied in two parts:
All HPDs at HNURC were invited to keep a time geographical diary during all working hours for a continuous period of two weeks. Diary data consisted of the date and time for activities performed, and the places and people present during the activities. Content analysis was performed to extract meaningful categories from reported activities (see example in Fig. 1). Activity distributions with time summed to 100% were generated to investigate patterns of time spent on activities in the emerged categories (see the matrix in Appendix 1).
Data collection
Demographics such as name, profession and place of employment were obtained from participants, and contractual time allocation for developmental and clinical tasks was obtained from a local registry. Time geographical diary data was collected on paper in a pre-printed matrix with column headings for registration of time, activities performed, and places and people connected to the activities (diary form, Appendix 1). HPDs received a pdf-file with a blank diary matrix and printed as many as needed. Time geographical diaries were filled in by HPDs during working hours for two weeks (equivalent to a total of ten workdays). The two-week duration of the data collection period was chosen to enhance variety in work tasks and to achieve a broad and realistic representation of the actual work tasks and time distributions of the HPDs with as little disruption as possible to daily clinical practice. The participants received written information about correct completion of the diaries, and they were invited to contact the first author by phone or email with any questions during the data collection period.
Pilot study
Four HPDs participated in a pilot study and completed diaries during a short period of three workdays in January 2018 to test the diary matrix. Only minor alterations were made concerning removal of a supplementary column where the participants could classify activities as primarily relevant for research, practice development or clinical practice. Since data from that column was not included in this study, all pilot data was included in the total material.
Participants
Participants were the 24 HPDs at the neurorehabilitation centre. All were experienced clinicians at expert level with three to 21 years of experience. They were ten nurses, seven physiotherapists and seven occupational therapists.
Data collection period
Pilot data was collected in January 2018. It was agreed between management and specialists that the month of May would be an appropriate period for the whole group, because there was no overlap with holidays or major projects that would make the HPDs tasks or time distributions differ from a normal workflow.
Workdays reported
Due to individually fluctuant work schedules with a mix of day-, evening- and night shifts to cover a 24-hour rehabilitation service at the centre, a mix of working hours equivalent to daily practice was expected.
Data analysis
Data on work activities was collected from paper forms and coded into categories according to the content analysis described by Elo og Kyngäs [19] by the first author. Categories were numbered and quantified using the software “Vardagen 2011 version 2.6.0.0” developed by Kajsa Ellegård and Kersti Nordell [14]. Data on time and activities was exported to Stata15 (StataCorp LLC, College Station, USA) to sum up results. Graphs were processed in Microsoft ® Excel ® (for Office 365).
Conceptualisation
The HPDs reported their daily work tasks over time in their own terms. A coding of these terms was applied to produce categories and subcategories as a complete conceptualisation of the HPD function. The first author performed all initial coding and contacted informants regularly to ensure that the emerged categories were in accordance with the informants’ understanding of reported activities as described by Gibbs [20]. As diaries were hand-written, questions concerning readability were similarly clarified. Patterns from individual data were combined into categories that covered the patterns and combinations between them (see example in Fig. 1). There were no predefined categories; all emerged from words used by the HPDs within the diary data. When content and meaning of a reported activity did not fit into the conceptual constructs of the words in an existing category, a new category emerged, or an existing category was redefined using different wording that contained the content and meaning of the new activity. Whenever possible, words that were reported by participants were preserved as category names to respect the intended meaning from the participants. When new categories emerged, all category names were read cross-sectional to avoid overlap and ensure exhaustion.
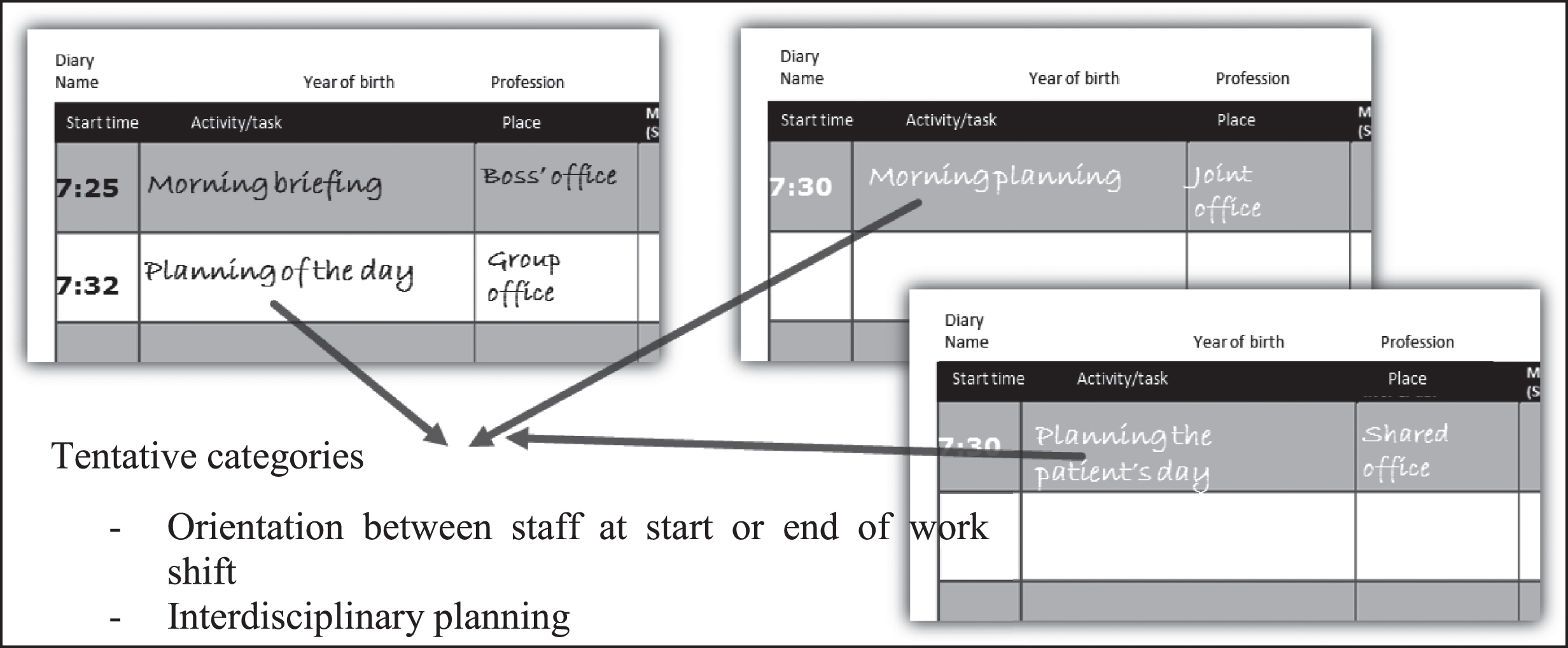
Example of content analysis: Categories and subcategories emerged from the participants own terms and content in the handwritten diaries.
A respondent validation was conducted to ensure content validity of the coded categories. Member checks were performed by two informants of different professions; a nurse and a physiotherapist. The coding of the first author was checked, and all emerged categories were discussed and approved. An extra category was added after this check, as both participants independently pointed out that a particular type of activity reported in the diaries did not match any already existing categories. The new category was named “Practical Tasks”. It concerned activities such as retrieving and bringing things for others, putting towels and sheets in cupboards, or emptying pelvic boilers, thus being activities that did not have a professionally defined content and could be performed by anyone with or without a health professional education.
The categorisation that emerged directly from the dataset structured and reduced the variation in the reported activities to enable a conceptual clarification of the HPDs work tasks. It also enabled a quantification necessary for systematic observation and pattern analysis.
Patterns within activity distributions
Activity distributions for the main categories were generated by summing the HPDs working time to 100%. The summed result with relative time spent per category was calculated for all HPDs in total, by profession (occupational therapists, physiotherapists and nurses) and by time allocated for developmental tasks (respectively one-third and two-thirds of the participants’ working time).
Ethical considerations
The study was performed in agreement with management at HNURC. According to the Danish Regional Scientific Ethical Committee regulations, the project was not notifiable, as no human biological material is included. The study was exempt from notification and permission requirements by the Danish Data Protection Agency [21].
Results
A total of 213 diaries were collected from 21 health professional developers from three professions at HNURC (seven physiotherapists, six occupational therapists and eight nurses) from January 19th to June 3rd, 2018. The summarised results of participants, activities and time are shown in Table 1. A total of 3351 unique entries were reported. Each participant reported from 6–13 days (median 10 days) covering 1680 working hours in total (see Table 1). Five diary days were excluded with only one or two activities reported. The exclusions were justified as the circumstance would yield an inadequate level of detail that did not add a relevant degree of nuanced information to contribute to conceptualisation of the HPD job function or realistically reflect the actual task variation during a workday.
Participants and activities. Number of participants, activities and reported time grouped by the represented professions; occupational therapists (occup), physiotherapists (phys), and nurses. Results shown as n (mean per person)
Participants and activities. Number of participants, activities and reported time grouped by the represented professions; occupational therapists (occup), physiotherapists (phys), and nurses. Results shown as n (mean per person)
All HPDs were women with a homogenous educational level corresponding to a Bachelor’s degree with the exception of only two (8%) of the 21 participants who had a supplementary one-year Master’s degree. Diaries were collected from all working HPDs at the time of the study. The three HPDs who did not participate were a) on long term sick leave b) on maternity leave and c) on a terminated work contract. Eleven of the HPDs (52%) had a third of their time contractually allocated to development tasks, whereas the other nine had two-thirds (see Table 1).
Conceptualisation – what the HPDs do
Eleven main categories of work tasks emerged (listed in Table 2) with 42 subcategories (2–6 subcategories per main category) (see full list of categories and subcategories in original Danish language in Appendix 2). These categories constituted a full conceptualisation of the HPDs work tasks as they were based on all reported activities during the datacollection period. The main categories were 1) Handing over, coordination, and planning; 2) Meetings, 3) Administrative tasks, 4) Tasks related to patients and their next of kin, 5) Facilitate competence development (social, learning and organisational); 6) Facilitate competence development (professional); 7) Treatment equipment, aids, technology, workplace, and premises; 8) Research related tasks; 9) Education and conferences; 10) Personal competence development; and 11) Meals and breaks. The 42 subcategories listed in Appendix 2 mirror a daily work routine with a high degree of variation and potential for frequent shifts between tasks during workdays.
Percentage of reported time for the eleven main work task categories that emerged from data by profession, contractual time allocation and in total (subtotals summed for tasks related to external knowledge and individual clinical expertise, respectively)
Percentage of reported time for the eleven main work task categories that emerged from data by profession, contractual time allocation and in total (subtotals summed for tasks related to external knowledge and individual clinical expertise, respectively)
The activity distribution for the total HPD group in the 11 main categories is presented in Fig. 2. The majority of their time was spent on tasks related to patients and their next of kin (33%), corresponding to the core task for the general clinical staff at the rehabilitation centre. This was no surprise, since the HPDs contractual time allocation for development related tasks would vary from one-third to two-thirds of their total working time, with remaining time dedicated to hands-on rehabilitation. Secondly, the HPDs only obligatory task was meeting attendance, which was summed to 18% of their reported time. The expert position of the HPDs was established by facilitation of competence development for other employees during 16% of their time. These well-represented tasks would, however, only contribute to maintenance of an existing level of professional knowledge within the organisation, as no external knowledge would enter the organisation through them. Summing up, 93% of the HPDs reported time was spent on tasks related to build up their individual clinical expertise and reasoning.
Development related tasks
At the other end of the spectrum, tasks among the least represented were research related tasks (2%) followed closely by participation in education and conferences (2%), and personal competence development (3%); corresponding to the only activities that could improve the knowledge level within the organisation through external evidence. Summed up, the HPDs spend only 7% of their total time on such development related tasks. See Fig. 2. This result equals to a low fulfilment of the intention behind the job function.

Total activity distribution for all HPDs: Working time summed to 100% for all participants to enable visual inspection of the activity distribution of the whole group. Tasks related to development account for only 7% of the total time.
In Figs. 3 and 4, a dichotomised inventory of development related tasks related to either external knowledge or individual clinical expertise maintaining current level of knowledge, is shown as proportions of total time reported by profession and contractual time allocation.
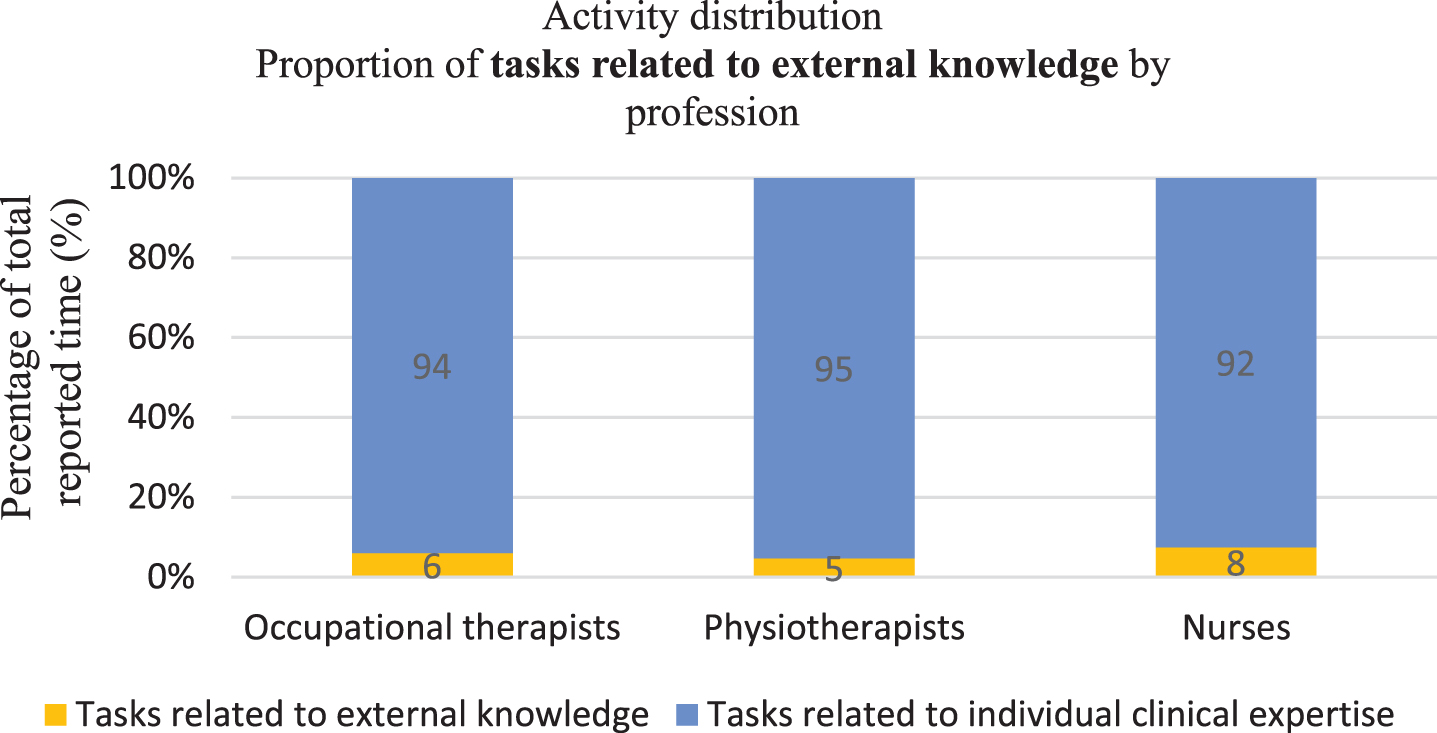
Proportion of tasks related to external knowledge by profession: Working time summed to 100% for participants from each profession (occupational therapists, physiotherapists and nurses).

Proportion of tasks related to external knowledge by contractual time allocation: Working time summed to 100% for participants by time allocation (Those having one-third of their time allocated to practice development and those with the majority of their time (two-thirds) allocated to practice development).
The proportion of time spent on build-up of external knowledge seemed to vary only a little between professions from 6% for physiotherapists, 7% for occupational therapists and 8% for nurses. When studying proportions of time spent on practice development by contractual time allocation, a surprisingly higher proportion of time spent on tasks supporting implementation of external knowledge were reported by HPDs with less time allocated for development (8% vs. 5%). The proportions were not statistically compared due to complexity of composite data summed from multiple participants with varying total time at work.
However, the main result prevails that the proportion of development related tasks adding external knowledge to clinical practice was low (8% or less) across professions and contractual time allocation.
A conceptual clarification of the HPD function was established with a total of 42 subcategories of varying work tasks in eleven main categories. The HPDs spent 93% of their total time on tasks maintaining an existing level of knowledge based on individual clinical expertise obtained from tasks related to patients, administration, and meetings, with most of their time (33%) spent on tasks related to patients and their next of kin. Only 7% of their total time was spent on practice development adding external knowledge. Proportions varied only marginally between professions and time allocations.
Evidence-based practice based on individual facilitators
With a busy work schedule including up to 42 different tasks, HPDs at HNURC and similar settings need to master a constant prioritisation of tasks. The fact that HPDs had contractually allocated time to take on tasks that were not directly patient-related should deliberate them from acute clinical obligations. However, most of their development dedicated time was consumed by daily practice routines, meetings and administrative tasks that served as maintenance of a current level of knowledge within the organisation. These activities would primarily serve to build-up personal one-on-one experience with patients and colleagues, making clinical expertise and reasoning the primary competence of the HPDs. To ensure evidence-based development of clinical practice at the highest possible level equivalent to international standards, external knowledge must however be obtained and integrated within the daily work routines of an organisation [22]. Commemorating Sackett’s definition of evidence-based practice [1], a combination of external and internal knowledge is necessary to optimise treatment and care for patients in modern healthcare. This could be true especially for rehabilitation practice due to the biopsychosocial approach that implicates a broad, specialised knowledge within multiple areas. This practice development should be supported by skilled facilitators [4]. However, with the individual expertise and reasoning generated mainly from one-on-one treatment of patients and bedside training of colleagues, the HPDs could not be expected to possess the skills to learn and transfer scientific knowledge to develop clinical practice.
The research practice gap
The Danish Leadership and Management Commission with ten experienced leaders appointed by the Minister for Public Innovation has recently announced official recommendations to perceive professional competence as working on the basis of systematic knowledge and evidence [23]. In an evidence-based practice, the desired outcome of HPDs would be development related tasks integrating external clinical evidence and individual-situated clinical expertise and reasoning in daily practice. However, the HPDs time distribution only supported implementation of external knowledge to a very low degree.
Law [22] has pointed out that a primary obstacle for evidence-based practice is the false assumption that it already exists. Further, she addresses the necessity of a humble approach from health care professionals who need to embrace the potential of their current practice being less than optimal. This matches the psychological effect established by Dunning and Kruger that lack of skill can deprive people not only of the ability to produce a desired outcome, but also of the expertise necessary to surmise that they are not producing them [24].
To implement the latest systematic knowledge and evidence, the HPDs should be able to critically assess scientific articles and to perform effect evaluation of clinical outcome measures. With such skills, the HPDs could facilitate a boost of knowledge within the organisation. Even though the HPDs were experienced and hardworking, their working task distributions did not support them to become familiarised with the latest and most effective choice of treatment. These reflexive competencies could be obtained through additional education such as a supplementary Master’s degree.
Decision-making to support evidence-based practice
The results should also be seen in an organisational context. Wright et al. describes individual-situated expertise as an intuitive skill fit for clinical decision-making [5]. When such expertise is integrated into managerial decision-making, a commitment to changes of daily actions and development of practice can be expected due to involvement in the decision process.
As logistics, time, and staffing influence decision-making for all health care professionals, a systematic application of new knowledge should be part of a supportive organisational structure to ensure effectiveness of treatment and high quality of care.
A total of 93% of the HPDs time was spent on tasks related to clinical expertise. This implies that the HPDs could not be facilitators of the latest external knowledge, and that their level of competence could not be expected to exceed that of an experienced clinician. This calls for an organisational structure that should involve the HPDs and yet separate them from the responsibility of decision-making with regards to implementation of new knowledge.
Limitations
The analysis was based on self-reported data. This led to a high degree of correspondence between the desired reports from the participants and the results obtained - for better or worse. If the HPDs had the desire to report an efficient work productivity to gain recognition, there may be a mismatch between the activities reported and the tasks performed by the HPDs resulting in potential information bias. Also, the HPDs were invited to fill in the diaries real-time, but if diaries were filled in with delay at the end of the day or later, there was a risk of recall bias, especially considering the busy work schedules reported. However, the HPDs all willingly participated in the data collection, and the diaries generally reflected daily observations of their workflow made by the primary author at the rehabilitation centre during the data collection period. Further, the homogenous activity distributions across groups could indicate that all participants understood the instructions in the same way and reported within the same understanding. The HPDs were allowed to report their own tasks, and the result is their voice speaking. With a conceptualisation based on inductive methodology of self-reported activities, the results reflect a mix of the factual task distribution and the subjectively reported feeling of bustle, commitment, job satisfaction, professional identity, etc, which is unknowingly written into their individual choice of words.
It is a profound limitation of this study that data does not allow for generalisation to other organisational settings as the clinical practice, service and management structure of the specific rehabilitation centre was locally developed within the Danish health care legislation and welfare system. Work tasks and distributions of HPDs reported here might differ from similar investigation results from other hospitals or rehabilitation centres. The problems with translation of external knowledge into clinical practice and the continuous struggle for health professional developers to prioritise between comprehensive responsibilities and tasks must, however, be recognisable within a plethora of other health care settings. Further, the need for an organisational supportive structure in combination with a boost of professional competencies could be recommended in any health care setting as well to substantiate knowledge transfer from research to clinical. This study serves as a clear example of data-driven analysis to systematically approach the subject with respect for individual, subjective reporting from competent health care professionals.
Conclusion
Conceptual clarification of work tasks of health professionals responsible for practice development was established in a clinical rehabilitation setting. Knowing how the HPDs working time was distributed between 42 tasks in eleven main categories made it possible to analyse their job function with regards to fulfilment of evidence-based practice development, which was accomplished inadequately. This study adds emphasis to the difficulties of task prioritisation in busy health care settings. The HPDs activity distributions contributed primarily to individual clinical expertise rather than development of evidence-based clinical practice based on external knowledge. A data-driven foundation for management to optimise the organisational structure of evidence-based practice development could be supported by these results with the recommendation of either upgrading the competencies of the HPDs to integrate external knowledge or by separating them from responsibilities regarding decision-making on implementation of new knowledge.
Implications
To ensure that all patients receive optimal treatment, the welcome challenge of evidence-based clinical practice has emerged in rehabilitation centres as in the entire health sector. Evidence from research results emerges with exponential speed, and health professional developers need to integrate new knowledge in an already busy workflow to offer treatment of high quality and avoid adverse effects in specialised settings. Thus, it is not enough that research results exist, or that specialists become skilled and experienced practitioners. Research and experience constitute two supplementary types of knowledge that must be combined to obtain evidence-based practice. This requires for health care organisations to examine and reflect on the consistency between working tasks performed by people responsible for clinical development and to offer a supportive organisational structure to ensure an ever improving, agile health care service.
Authors’ contributions
The first author initiated the study, conducted the investigation, analysed the results and wrote the article. The second author was experienced within neurorehabilitation research and offered guidance on methodological considerations regarding the content analysis and commented on the article. The third author supported the methodological application of the time geographical method and commented on the article. The last author contributed to the scope of the article, discussed the data analysis and the discussion of the results and commented on the article.
Conflict of interest
The authors report no conflicts of interest and no external funding.
Footnotes
Acknowledgments
The first author wishes to thank management at HNURC for approving the project, all who took part in the study, the two clinical experts, M and C, who assisted the data validation with member checks, and especially the leading therapist Mette Skjærbæk Svane for professional companionship. This project was carried out as an honours programme project at Aarhus University.