
Abstract
BACKGROUND:
Beyond the health-enhancing effects, work also has the potential of causing or worsening different health conditions in the same individual. However, research on within-worker aggregation of work-related health problems is scarce.
OBJECTIVE:
To describe the history and aggregation of work-related health problems in a population-based sample of women.
METHODS:
A total of 4330 women were asked whether they had ever had “a physical or mental health problem that was caused or made worse by your work”. The aggregation of work-related health problems was assessed using an exploratory factor analysis.
RESULTS:
Five groups were identified. Factor 1 included all items on musculoskeletal disorders - lower socioeconomic position, higher BMI, smokers and history of occupational accidents. Factor 2 included mental disorders together with headache and/or eyestrain - higher socioeconomic position. Factor 3 included the other disorders item with some loading from digestive disorders - older and public sector workers. Factor 4 included respiratory disorders - lower socioeconomic position and history of occupational accidents. Factor 5 included hearing and ear problems - blue-collar workers.
CONCLUSION:
There was a relevant aggregation of work-related health problems, which may inform the selection of specific components for interventions that aim to improve women’s work-related health.
Introduction
Work can have health enhancing effects as a source of paid income and financial security, as well as social integration. However, it also exposes workers to a wide range of physical and psychosocial stressors that can have a negative impact on health [1]. As a result, work has the potential to contribute to the onset or worsening of different health conditions in the same individual throughout working life. Nevertheless, research focusing on within-worker aggregation of work-related health problems is scarce.
The population burden of work-related diseases is still underestimated due to shortcomings in the available data [2], which reflect the definition, recognition and reporting challenges it entails. The low coverage of certain types of professionals by the social security system –namely rural workers, self-employed workers, workers in small-sized enterprises and in the informal economy –is another limitation of official data [3]. The constant emergence of new risks and the exposure to new substances that have not yet been identified as hazardous also pose a challenge to the acquisition of up-to-date and accurate data [3]. Moreover, the underreporting of less severe cases of disease is a constraint even in high-income countries that usually have better surveillance coverage. Among physicians, the difficulty in assigning an occupational origin, lack of awareness regarding reporting requirements and insufficient knowledge of diseases with an occupational aetiology constitute major challenges to disease diagnosis and attribution [3–5]. Conversely, worker-related barriers to disease reporting include less severe disorders, insufficient knowledge on reporting and compensation, and fear of retribution by the employer [6–8]. Thus, official figures provide insight into notified, recognised and compensated occupational diseases, which only covers a very limited group of disorders, while not encompassing the broader concept of work-related health problems.
Gender segregation in the labour market remains high; the uneven concentration of women in typically lower-paid sectors is still a concern [9]. Although women’s work participation has increased considerably in recent decades [10], women still face a double burden phenomenon where women working full-time in the labour market often face a second shift at home. Furthermore, though there are more men in informal employment globally, women in the informal economy are more often found in vulnerable work-related situations; for example, as domestic workers, home-based workers or contributing family workers [11]. Work-related health conditions among these women are less likely to be reported, and as a result are underestimated. Thus, comprehensive approaches using complementary methods in addition to official statistics are required [12], particularly when studying work-related health in women.
Valuable information to complement data from registries can be obtained using population-based approaches, as they provide the perspective of the target population outside of the workplace setting. In particular, large population-based prospective studies constitute a unique opportunity to obtain information on work-related conditions and to provide worker-centred estimates of the burden associated with work-related health problems with less a priori constraints, while also keeping up with the rapidly growing changes of the labour market. Although not designed for that purpose, a specific dimension where birth cohorts may be particularly interesting is in the study of women’s occupational health, since they imply regular follow-ups of working age women and frequently collect information on social context dimensions.
Thus, we aimed to describe the history and agg-regation of work-related health problems in a popu-lation-based sample of women from a large birth cohort study, and to quantify their association with sociodemographic, health and other work-related characteristics.
Methods
Participants
This study was based on the prospective popula-tion-based birth cohort study Generation XXI [13, 14]. Newborns and their mothers were recruited during 2005/2006 from the five public maternities covering the metropolitan area of Porto, which included 91.6% of all deliveries in the catchment area at the time of recruitment. Of the mothers invited, 91.4% accepted to participate. A total of 8495 mothers and their 8647 children were enrolled at baseline. The cohort has been followed since childbirth, with four assessment waves of the overall cohort already completed. Only data collected regarding mothers were used to accomplish the objectives of this study. Data were obtained in the context of two follow-up waves, when their children were seven (April 2012 to April 2014) and ten years of age (July 2015 to July 2017).
For the present analysis, all women (n = 4330) who accompanied their child to the 10-year-old follow-up, and who had valid information on work-related health problems, age and educational level were included. When compared to the remaining mothers (n = 4165), women included in this study were older (30.0 vs. 27.9 years), had a higher educational level (11.2 vs. 9.7 schooling years) and were less likely to have a blue collar job (21.3 vs. 25.8%).
The Generation XXI cohort study protocol was approved by the Ethics Committee of the São João Hospital/University of Porto Medical School, and complies with the Ethical Principles expressed in the Helsinki Declaration and with the current national legislation. The project was registered with the Portuguese Authority for Data Protection. Written informed consent was obtained for all assessments.
Data collection
Sociodemographic characteristics
Women’s age and marital status were collected, and level of education was recorded as ≤9, 10–12, or > 12 years of completed education. Monthly house-hold income was recorded in EUR 500 categories, and was grouped into EUR≤1000, 1001–2000 and > 2000. The first class included the situation where both parents received around the minimum national wage (EUR 485.00 in 2013 [15]). Apart from wo-men’s age, which was collected at the children’s 10-year-old assessment wave, the additional sociodemographic characteristics were only available from the seven-year evaluation.
Work-related characteristics
Mothers accompanying their children to the seven-year-old follow-up were asked about five groups of work-related characteristics: i) maternal occupation (current or previous if unemployed or retired) was collected and classified according to the Portuguese Classification of Occupations 2010, which is based on the International Standard Classification of Occupations (ISCO-08) [16], and was grouped as follows: (a) managers, (b) professionals, (c) technicians and associate professionals, (d) clerical support workers, (e) services and sales workers, (f) skilled agricultural, forestry and fishery workers, and craft and related trades workers, (g) plant and machine operators and assemblers, and (h) elementary occupations; ii) participants were asked about the number of concurrent jobs, which were categorized as none, one, or two or more jobs; iii) data on employment status was grouped as employed as a full-time worker, employed as a part-time worker, unemployed, or other (including unpaid family worker, student, retired, homemaker); iv) the nature of employment was defined as civil service or public sector, private sector, self-employment or other (e.g. homemaker); and v) participants were also asked about whether they were in managerial positions.
Health-related characteristics
Weight and height were measured to the nearest 0.1 kg and 0.1 cm respectively, by trained examiners and according to standard procedures. Body mass index (BMI; kg/m2) was calculated and categorized into three groups - underweight/normal weight (≤24.9 kg/m2), pre-obesity (25.0–29.9 kg/m2) and obesity (≥30.0 kg/m2) - according to WHO standards [17]. Smoking status was assessed and participants were categorized as current smoker (daily or less than daily), former smoker (not smoking for at least six months) or never smoker. Participants were also asked whether they had ever had a work accident (commuting accidents excluded). Health-related variables were collected at the seven-year evaluation.
Work-related health problems
Mothers accompanying their children to the 10-year-old follow-up were asked to report, via a self-administered questionnaire adapted from the 2013 Labour Force Survey (LFS) ad-hoc module on ‘acci-dents at work and other work-related health problems’, whether they had ever had “a physical or mental health problem that was caused or made worse by your current work or any previous work”. If an affirmative answer was provided, additional information on the type of condition was obtained and categorized as follows: (a) bone, joint or muscle problem that mainly affects the back, (b) bone, joint or muscle problem that mainly affects the neck, shoulders, arms or hands, (c) bone, joint or muscle problem that mainly affects the hips, knees, legs or feet, (d) stress, depression, anxiety or mental disorders, (e) breathing or lung problems, (f) headache and/or eyestrain, (g) heart disease, stroke or other circulatory system problems, (h) kidney, stomach, liver or other digestive problems, (i) hearing and ear prob-lems, (j) skin problems, (k) infectious diseases (virus, bacterium or other type of infection), and an open-ended option (l) other health problems. The open-ended option category included, with decreasing frequency, immune-mediated, neurological, voice-related and endocrine conditions. Women were also asked whether any of those health problems had been officially recognized as an occupational disease. Data on the spouse’s history of work-related health problems were retrieved from the same questionnaire applied to biological fathers of the Generation XXI children who accompanied their child to the seven-year assessment wave, and those who were part of the same household as the mother at the time were included in this analysis.
Statistical analysis
The characteristics of the study population were described at the seven-year-old assessment wave by summarizing categorical variables as counts and proportions. The different types of work-related health problems reported in 2013 were also described as relative frequencies.
The associations between reporting at least one work-related health problem and sociodemographic, health and work-related characteristics were estimated using a logistic regression model to calculate adjusted odds ratios (ORs) and the respective 95% confidence intervals (CIs).
Exploratory factor analysis (EFA) based on tetrachoric correlation with varimax rotation due to the dichotomous nature of the variables on work-related health problems were applied to reveal clusters of work-related health problems [18]. The number of factors was set equal to the number of eigenvalues≥1.0 [19]. In order to assess the robustness of the results, other strategies were used, namely removing the ‘Others’ category due to its heterogeneity or using a different criterion to determine the number of factors (sample size adjusted BIC - Bayesian Information Criterion). Within factors, variable loadings with an absolute value of 0.40 [20] or higher were interpreted as having a meaningful contribution to the corresponding underlying factor. For each participant, a factor score was calculated using the weights of each of the variables for that particular factor. In order to compare the mean component scores by sociodemographic, health and work-related characteristics, and thus interpret the factors resulting from EFA, a one-way analysis of variance (ANOVA) was performed.
Data were analyzed using the statistical software IBM SPSS Statistics for Windows, Version 21.0 (Chicago, Illinois), and the R package version 3.3.0 (‘psych’ package).
Results
Table 1 summarizes the participants’ sociodemographic, health and work-related characteristics. Most women were younger than 45 years of age (85.3%), had 12 or less years of education (68.5%), were married (87.0%), were pre-obese or obese (54.5%), and had never smoked (63.5%). Regarding their spouses, 29.3% reported ever having had a work-related health problem. The most common occupational groups among women were Services and Sales Workers followed by Professionals (28.6% and 21.5%, respectively). Most participants had one job (73.2%), were full-time workers (70.8%), worked in the private sector (65.9%), and were not in managerial positions (70.2%). A history of occupational accidents was reported by 23.7% of the women.
Prevalence of reporting at least one work-related health problem by sociodemographic, health and work characteristics among Generation XXI mothers
Prevalence of reporting at least one work-related health problem by sociodemographic, health and work characteristics among Generation XXI mothers
The overall prevalence of reporting at least one work-related health problem since the beginning of working life was 31.5% (n = 1366). Fig. 1 shows the proportion of each type of health problem. Mental disorders were the most prevalent (21.3%), followed by those related to the neck and/or upper limbs (17.0%), and headache and/or eyestrain (16.9%). The prevalence of reporting an officially recognized occupational disease was 11.4%
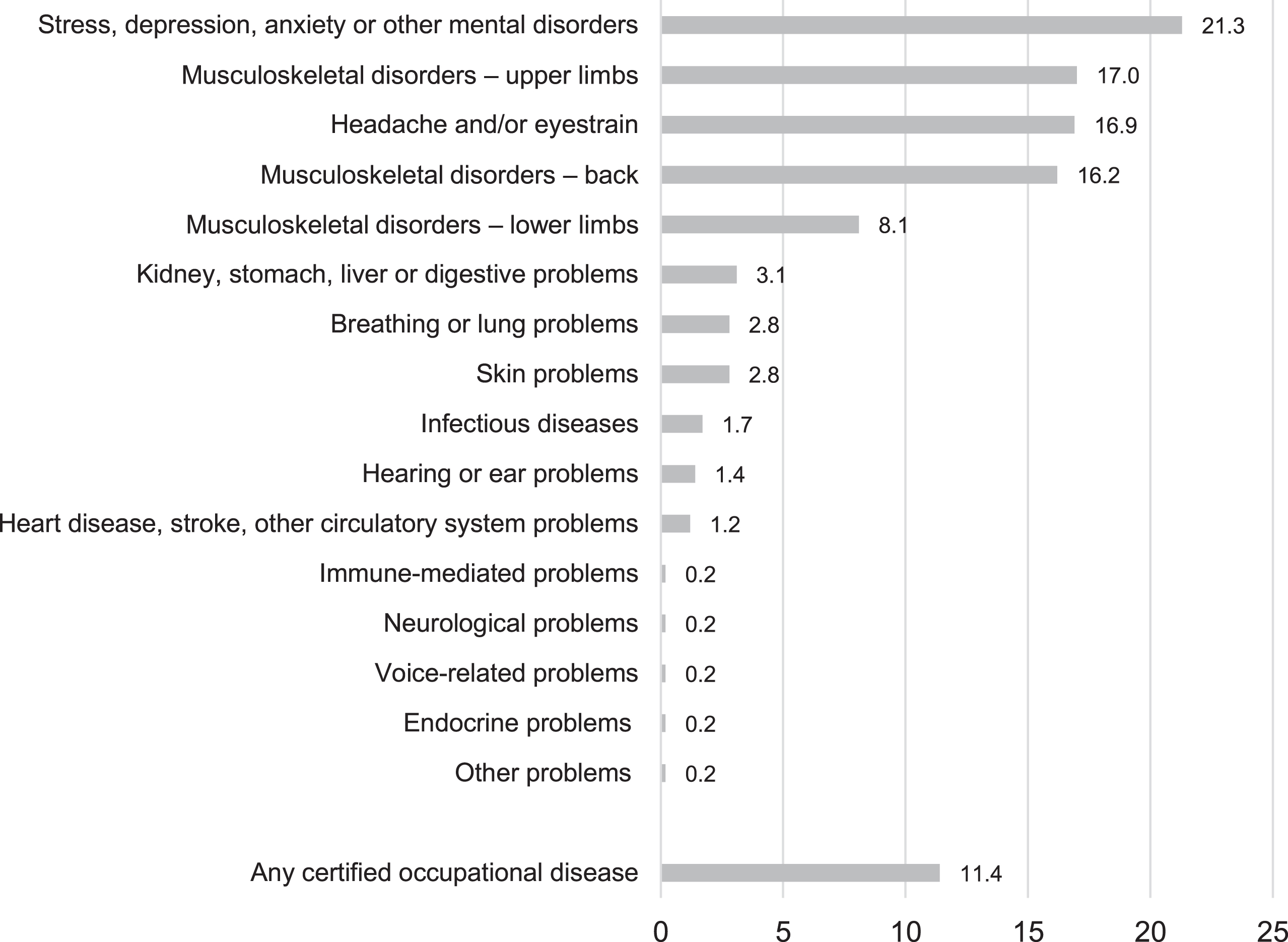
Proportion (%) of each work-related health problem and of recognized occupational diseases among Generation XXI mothers.
Figure 2 and Supplementary Table 1 show the associations between participants’ sociodemographic, health and work-related characteristics, and reporting at least one work-related health problem throughout working life. Women more likely to report a work-related health problem were 36–45 years of age (OR = 1.23, 95% CI: 1.04–1.47), had more than 12 years of education (age-adjusted OR = 1.16, 95% CI: 1.00–1.36), were single (age- and education-adjusted OR = 1.44, 95% CI: 0.99–2.09), had a EUR 1001–1500 monthly household income (adjusted OR = 1.23, 95% CI: 1.03–1.47), were obese (adjusted OR = 1.21, 95% CI: 1.01–1.44), were current smokers (adjusted OR = 1.24, 95% CI: 1.06–1.45), had reported any work accidents since the beginning of working life (adjusted OR = 2.52, 95% CI: 2.17–2.92) or had a spouse with a history of work-related health problems (adjusted OR = 2.60, 95% CI: 1.92–3.52). Concerning work-related characteristics, women were more likely to report a work-related health problem if they had more than one concurrent job (adjusted OR = 2.16, 95% CI: 1.58–2.94), and were in a managerial position (adjusted OR = 1.18, 95% CI: 1.02–1.36). Compared to workers in the civil service or public sector, those from the private sector and self-employed participants had lower odds of work-related health problems (adjusted OR = 0.81, 95% CI: 0.67–0.96 and adjusted OR = 0.69, 95% CI: 0.54–0.89, respectively). No strong associations between occupational group and health problems were found. Women who were unemployed or had an unpaid occupation at the time of the questionnaire had lower odds of reporting a history of work-related health problems throughout life (adjusted OR = 0.70, 95% CI: 0.59–0.84 and adjusted OR = 0.26, 95% CI: 0.17–0.41, respectively).

Association between participants’ (a) sociodemographic and health characteristics, and (b) work characteristics and reporting at least one work-related health problem (odds ratio, OR, and respective 95% confidence interval, CI).
Five groups describing health problem aggregation (Table 2), which accounted for 57.2% of the observed variance, were identified using an EFA among women who reported at least one work-related health problem (n = 1366). Factor 1, which accounted for the largest proportion of variance (17.9%), included all items on musculoskeletal disorders, i.e. those affecting the back, neck and/or upper limbs, and lower limbs. Factor 2 included the items on stress, depression, anxiety and other mental disorders, as well as headache and/or eyestrain (11.6% of the variance explained). Factor 3 included mostly systemic organic diseases and/or dysfunctions, namely the item on other types of disorders comprising immune-mediated, neurological, voice-related and endocrine problems, and also had some loading from kidney, stomach, liver or digestive disorders. Factor 4 included breathing or lung problems and factor 5 included hearing or ear problems. Heart disease, stroke, other circulatory system problems, as well as skin conditions and infectious diseases did not clearly load into any of the factors using this approach. The robustness of the factor solution using two alternative approaches was tested. First, the category ‘Others’ was removed from the EFA with the percentage of total variance explained decreasing (51.3%), and only factors 1 (musculoskeletal disorders) and 2 (mental disorders, and headache and/or eye strain) remaining stable (Supplementary Table 2). Alternatively, an EFA with seven factors was performed, according to a different number of factors extraction criterion - sample size adjusted BIC (Supplementary Table 3) - and the same two factors 1 and 2 emerged. In both approaches, with the exception of factors 1 and 2, the remaining factors did not clearly overlap with the original EFA solution.
Exploratory factor analysis with tetrachoric correlation for reporting at least one work-related health problem (eigenvalue≥1.0 criteria)
*Includes immune-mediated, neurological, voice-related and endocrine conditions, among others.
Figure 3 shows the mean scores for each factor across sociodemographic, health and work characteristics. Women scoring higher on musculoskeletal disorders (Factor 1) had a lower educational level, a higher BMI, were more likely to be current smokers, had a lower income, were not in a managerial position, had a history of occupational accidents, and were predominantly blue-collar workers (skilled agricultural, forestry and fishery workers, craft and related trades workers, plant and machine operators and assemblers, and elementary occupations) as well as services and sales workers. Factor 2 (mental disorders, and headache and/or eye strain) showed higher scores among participants with a higher educational level, a higher income, and with white-collar jobs. Factor 3 (systemic organic diseases and/or dysfunctions) presented higher scores in older and in public sector working participants. Factor 4 (breathing or lung problems) was associated with a lower educational level, a lower income and reporting work-related accidents. Finally, factor 5 (hearing or ear problems) scores were higher among blue-collar workers.

Mean and 95% CI factor scores by sociodemographic, health and work-related characteristics.
In this study, we found that almost one third of working age mothers, selected independently of occupational exposures, reported at least one work-related health problem during their working life. Mental and musculoskeletal disorders were the most frequent work-related health problems, and were also the main features of the two most robust aggregation factors identified using exploratory factor analysis. Different factors were associated with specific sociodemographic, health and work characteristics that were not evident when estimating the association between any work-related health problem and the same characteristics. This study demonstrates the potential of using a large population-based birth cohort as a valuable and complementary source of information to describe work-related health problems. In particular, for work-related psychological distress and musculoskeletal disorders, which were the most prevalent health problems in our sample, assessing the worker’s own perspective is informative, and even more significant in countries that do not recognize mental disorders as occupational diseases [21] or in countries that do not include certain types of musculoskeletal disorders in their national list of occupational diseases [22].
A low proportion of women reported having one work-related health problem officially certified as an occupational disease, which shows the discrepancy in estimates between the latter and the broader concept of work-related health problem, and is a reflection of the definitional, identification and recording issues that work-relatedness entails.
The study of work-related conditions among women is particularly relevant in our context, as Portugal constitutes one of the 13 out of 29 European countries where the prevalence of self-reported work-related health problems is higher in women than in men (7.0% vs 5.5%) [23, 24]. Accordingly, we also observed the same pattern in data stemming from official statistics [25], where 70.1% of officially recognized occupational diseases occur in women [26]. Specifically, women present an increased prevalence of negative mental health outcomes than their male counterparts [27], which may be explained by the cumulative exposure to psychosocial risk factors that women face both at home and in the workplace. Additionally, although the number of women in the workforce has increased considerably in recent decades, there is still an unequal task division at home, even when both partners work full-time, and women remain primarily responsible for domestic work (such as caring for children, the elderly and disabled). This double burden phenomenon decreases women’s time for recovery after a workday, which has been linked, not only to negative mental health outcomes, but also to increased musculoskeletal symptoms [28–30], which in turn may hamper everyday family activities, particularly in families with children.
Our results are in line with previous national self-reported estimates from 2013, in which mental and musculoskeletal disorders were shown to be the most frequently reported work-related problems by women regarding the previous year [25, 31]. Likewise, a similar pattern has been described throughout Europe [23]. However, contrasting our finding of a higher burden attributed to mental disorders, back-related musculoskeletal disorders throughout working life were the most prevalent in 2013 [31]. This may be explained by the comparative overrepresentation of white-collar workers in our sample, when compared to national data [25], who are more likely to be affected by mental disorders [32, 33]. Additionally, we estimated working life prevalence, with the aim of providing a picture of workers’ entire professional life. When compared to shorter reference periods, our option may have introduced some recall bias leading to the underestimation of disorders of shorter duration that are more likely to be forgotten, as may be the case for acute episodes of musculoskeletal symptoms.
Our approach suggests that looking at associations between participants’ characteristics and reporting at least one work-related health problem is likely to hide a heterogeneous group of problems. We looked into how these health problems could aggregate using an exploratory approach to summarize work-related health problems. EFA was compatible with five clusters of co-occurring work-related health problems and specific sociodemographic, health and work-related characteristics. The factor that included all items on musculoskeletal disorders (Factor 1) was associated with a low educational level, obesity, smoking, low income, blue-collar jobs, not being in a managerial position and a history of occupational accidents. This is in line with the frequently reported risk factors for work-related musculoskeletal disorders that include, in addition to smoking and high BMI, high biomechanical and psychosocial demands [34] –which are commonly linked to a low educational level and low income blue-collar jobs [35]. Furthermore, the presence of co-morbidities, including previous musculoskeletal injuries, constitutes a risk factor for work-related musculoskeletal disorders [34]. Our finding of a second factor, which grouped mental disorders and headache and/or eyestrain, and was associated to qualified occupations is also in line with previous findings of a higher prevalence of psychosocial problems among white-collar workers when compared to blue-collar workers [33]. Moreover, the use of visual display units, predominantly linked to white-collar jobs, has been associated with headache and other eyestrain symptoms [36]. Our hypothesis that older participants are more likely to report systemic organic conditions that are usually associated with ageing and aggravated rather than caused by work, was reflected in Factor 3, which aggregated the item on other types of disorders (immune-mediated, neurological, endocrine and other problems) and also kidney, stomach, liver or digestive disorders. Workers from the public sector also scored higher in Factor 3, which may translate a healthy worker effect whereby individuals with chronic conditions might be less likely to remain in more competitive and insecure workplaces, such as private and informal sectors. Regarding the associations between Factor 4 (breathing and lung problems) and a lower education and income, previous research on work-related respiratory problems has traditionally focused on men. Indeed, work environments affected by occupational exposures associated with lung health, such as primary and secondary industries, are dominated by men [25], and there is limited understanding of how these exposures affect women. Nevertheless, the most frequently recognized occupational respiratory diseases in Portugal [25] are highly prevalent in industries where female workers are largely employed: silicosis (crystalline silica particles’ exposure) and the ceramic industry [37], and asthma and exposure to cleaning agents [38, 39]. The latter is also an exposure that disproportionately affects women in the household when compared to men. Some studies have also linked occupational asthma in women to biologic agents, the textile industry, flour dust, and occupations such as hairdressers/beauticians and healthcare professionals [38–41]. The association between lung problems and a low education and income can thus be explained by the higher prevalence of manual jobs, or alternatively by reverse causation, as work-related asthma is linked to adverse economic and employment consequences, particularly among manual workers [42–44]. Finally, in our study, women reporting hearing or ear problems (Factor 5) were predominantly blue-collar workers, which is in line with current knowledge that noise-induced hearing loss is not only associated with age but also blue-collar jobs [25, 45, 46].
We acknowledge that multiple factoring solutions could be applicable to our data, each implying different interpretations and associations with background characteristics. Indeed, when we tested two slightly different analytical options, the clustering of factors 3 to 5 or 7, which involve comparatively infrequent conditions, the results obtained differed. Due to our sampling frame, our findings are likely to be more robust to detect work exposures and general health profiles that are more frequent in the general working population. Factors 1 and 2 loaded in the same manner when using different approaches, showing that musculoskeletal conditions and headache and/or mental health conditions are likely to represent a stable and meaningful grouping of work-related health problems in the general female working population. The factoring solution found by our EFA had a cumulative percentage of variance explained slightly below the commonly accepted threshold of 60% [47], which may be explained by the fact that our latent variables are difficult to identify.
Our sample of mothers from a population-based birth cohort may have limited the generalizability of our findings to the entire female workforce. These women may be homogeneous with regards to some sociodemographic characteristics as they represent a target population of women from an urban setting that gave birth to a child at a specific moment in time. Indeed, in comparison to the female population in the Northern region (Portuguese NUTS II classification) in 2013, women included in this study had a higher educational level (15.3 vs 31.5% with more than 12 years of education [48]) and blue-collar jobs were underrepresented, particularly Plant and Machine Operators and Assemblers (12.2 vs 4.7%) and Elementary Occupations (18.7 vs 10.0%) [49]. Nevertheless, our sample had an unemployment rate of 17.6%, which is similar to the 18.0% female unemployment rate in the Northern region in 2013 [50]. The nature of our data did not allow us to infer on the co-occurrence of work-related health problems at the same time, only that they were reported by the same individual throughout their working life. Also, the participants’ characteristics presented refer to one moment in time and may not be an accurate proxy for the entire lifetime exposure. Nevertheless, the fact that only 18.6% of women changed their occupational category (between low skilled blue collar, high skilled blue collar, low skilled white collar and high skilled white collar [51]) from the baseline to the follow-up evaluation occurring seven years later, leads us to believe there was a substantial stability over time regarding occupations and exposure to professional risks in these women. Moreover, we relied on self-reported information to define work-related health problems without clinical validation, which may introduce some level of misclassification. For instance, the finding that reporting a work-related health problem was associated with reporting an occupational injury may be explained not only by the exposure to occupational hazards that contribute to both problems, but also by the possibility that acute episodes of chronic problems may have been reported and classified as accidents, such as musculoskeletal disorders occurring after lifting heavy loads. However, symptoms are a key component of any clinical diagnosis of the most prevalent health problems in our sample. As a result, it has been shown that problems, such as musculoskeletal, are often accurately self-reported while underrepresented in clinical records [52]. In other cases, such as depression and anxiety, there is no relevant difference between data stemming from health surveys and electronic health records [52]. Also, the fact that associations were stronger for work characteristics when compared to sociodemographic and health characteristics reinforces that, in general, participants were able to assess work-relatedness. Overall, using a large population-based sample provided us with the perspective of the target population outside the workplace, with no a priori constraints, such as occupational group, sector of activity or type of health problem. It also allowed us to focus, not only on occupational diseases, but especially on the wider concept of work-related health problems as experienced by female workers.
Conclusion
By using a population-based sample, this study provided a worker’s perspective on work-related health problems since the beginning of working life, including the identification of groups of health problems with specific characteristics. We found that the factor that gathered all items on musculoskeletal disorders as well as the factor that gathered the item on stress, depression, anxiety and other mental disorders, and headache and/or eyestrain, were the most reliable factors. As such, our analysis supports the need for a shift from a disease-by-disease approach towards a worker-centered perspective, while forming a basis for the selection of specific bundles of interventions that aim to improve women’s work-related health that are better targeted, prioritized and integrated.
Conflict of interest
None to report.
Funding
This study was funded by the European Regional Development Fund (ERDF), through the Operational Programme Competitiveness and Internationalization, and national funding from the Foundation for Science and Technology (FCT) - Portuguese Ministry of Science, Technology and Higher Education - under the projects “STEPACHE - Raízes pediátricas da resposta ampliada à dor: das influências contextuais à estratificação do risco” (POCI-01-0145-FEDER-029087; Ref. FCT PTDC/SAU-EPI/29087/2017), and “HIneC: Quando se revelam as desigualdades em saúde?” (POCI-01-0145-FEDER-029567; Ref. FCT PTDC/SAU-PUB/29567/2017). This work was also supported by the Unidade de Investigação em Epidemiologia - Instituto de Saúde Pública da Universidade do Porto (EPIUnit) (POCI-01-0145-FEDER-006862; Ref. UID/DTP/04750/2013), by Administração Regional de Saúde Norte (Regional Department of Ministry of Health) and Fundação Calouste Gulbenkian. This research was also supported by the PhD Grant PD/BD/128009/2016 (Joana Amaro) co-funded by FCT and the Human Potential Operating Program of the European Social Fund (POPH/FSE Program). This study is also a result of the project DOCnet: Diabetes & obesity at the crossroads between Oncological and Cardiovascular diseases –a system analysis NETwork towards precision medicine (NORTE-01-0145-FEDER-000003), supported by the Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the ERDF.
Footnotes
Acknowledgments
We thank the families enrolled in Generation XXI for their kindness, the members of the research team for their enthusiasm and perseverance, and the participating hospitals and their staff for their help and support. We also thank Henrique Barros and Ana Cristina Santos for their role in the coordination of the Generation XXI cohort and the field work team for their dedication.