
Abstract
Background:
Small and medium sized enterprises are yet uncharted territory in terms of presenteeism. In addition, the Demand-Control-Support (DCS) and Siegrist’s Effort-Reward Imbalance (ERI) models are proposed to predict stress-related health problems, but not for sickness behaviors such as presenteeism.
Objective:
This study aims to examine the relationships between psychosocial risk factors, presenteeism, mental and physical health in the context of small and medium-sized enterprises (SMEs). This study also examines the moderating effect of company size on these associations.
Methods:
To test the association between psychosocial risks, presenteeism, and health, only people working in small and medium-sized enterprises (SMEs) of between 2 and 199 employees were included in the sample, giving a total of 2,525 SME employees surveyed. To test the differences in exposure to psychosocial risk and presenteeism, and the moderating impact of size on the relationship between psychosocial risks, presenteeism, and health, we took the original sample (4608) of the EQCOTESST.
Results:
The results confirm the associations between job demands, social support and effort-reward imbalance, and presenteeism. Also, the associations between presenteeism and health problems in SMEs’ context. Multi-group analyses show that the business’s size does not moderate the strength of the relationships between psychosocial risks, presenteeism and health.
Conclusion:
The current study highlights that SMEs are somehow protected from certain psychosocial constraints such as high job demands, and low social support, but are more exposed to others such as effort-reward imbalance.
Keywords
Introduction
Several studies focus on examining the determinants of presenteeism to understand, detect, and prevent presenteeism [1]. Researcher report that presenteeism is associated with psychosocial risks, such as psychological demand [2], supervisor support [3], group cohesion [4, 5], control or decision latitude [6], and pressure from supervisors or colleagues [4]. Gilbreath and Karimi [7], refer to the term “job-stress-related presenteeism” as a form of presenteeism whose antecedents are psychosocial risks. Nevertheless, work on presenteeism remains atheoretical [8, 9], particularly concerning the association between psychosocial risks and presenteeism.
Research on psychosocial risks is commonly based on Karasek and Theorell’s Demand-Control-Support (DCS) and Siegrist’s Effort-Reward Imbalance (ERI) models. However, it should be noted that both the DCS and the ERI models are proposed to predict stress-related health problems due to adverse psycho-social work conditions, but not for sickness behaviors such as presenteeism. Some studies confirm the predictive validity of these two models (DCS; DER) to explain absenteeism [10], but not presenteeism. Also, it appears that psychosocial risks are often studied independently, without trying to evaluate their relative importance and their interaction in the explanation of presenteeism. In fact, psychosocial risks are rarely studied in a logic of interaction and combined in the same theoretical framework to explain presenteeism.
Health status is also considered a determinant of presenteeism [11]. Research has shown that employees with health problems report more presenteeism compared to other employees [12]. Other studies show that presenteeism leads to diminished mental and physical health outcomes such as burnout [9], physical and psychological exhaustion [13], depression [14], coronary conditions [15], as well as a deterioration in individuals’ overall state of health [16]. Gustafsson and Marklund find that employees with lower levels of presenteeism experience better health at a later stage. In their systematic review, Stagen et Collins [17] suggest that there is a need for further qualitative and quantitative research to better understand presenteeism and particularly its impact on mental and physical health.
In addition, a review of the literature shows that most of the research on presenteeism was conducted in major organizations or in the public service, particularly in the health and education sectors [18]. Small and medium-sized enterprises (SMEs) are a field in which empirical research on presenteeism has never been conducted. Also, until now, there is minor empirical evidence regarding differences in psychosocial risk and presenteeism among employees in smaller and larger companies [19].
To sum up, this study has three objectives. Firstly, it examines the relations between psychosocial risk factors–identified in Karasek and Theorell’s De-mand-Control-Support (DCS) and Siegrist’s Effort-Reward Imbalance (ERI) models–, presenteeism, mental and physical health. These associations are tested in the context of small and medium-sized enterprises (SMEs). Secondly, it tests the differences in exposure to psychosocial risk factors and presenteeism according to company size. Finally, it examines the impact of business’s size (small, medium, large) on the relationships between psychosocial risks, presenteeism, physical and mental health.
The DCS and ERI models and their relevance to presenteeism
The DCS model
1.1.1.1. Relation between job demands and presenteeism: Job demands, including contradictory demands and time pressures [6], are positively associated with presenteeism [20]. Employees with a heavy workload are more likely to practice presenteeism to maintain a high standard of performance [21], or to avoid accumulating more work when returning from sick leave [6]. In their longitudinal study, Demerouti et al. [22] found that high demands in the workplace were associated with occupational burnout (emotional exhaustion) and presenteeism.
Studies show that in SMEs, staff cutbacks can create work overload for the remaining employees [23]. The resulting problems encountered in replacing or recruiting staff and in retaining those best suited for the job can often lead to increased workloads for those who remain [24]. DeKok [25] explains that absenteeism rates are lower in SMEs. Concerns of employees about how an absence on their part will adversely affect day-to-day operations, their belief that organizational tasks need to be performed every day or the feeling that they are indispensable [3] are all possible risk factors contributing to presenteeism in SEMs. Mahé de Boislandelle [26] shows that a minor event in a large company can produce negative effects in an SME. Thus, the absence of one employee can become a source of stress by cascading risk effects (one problem that leads to another [27]. In addition, because of labor shortage and the inability to replace employees, SMEs do not facilitate the management of absent employees and rarely offer solutions for temporary replacements, which leads to presenteeism. Large businesses handle the problem of absence better [25], and have the possibility of hiring reserve staff to guarantee the availability of labor and to prevent problems related to overwork. The multiple roles and tasks may be perceived positively, to the extent that employees use their expertise, make decisions, actively participate in the organization’s strategic direction, and develop a sense of responsibility [28]. However, the multiplicity of roles and tasks results in an overload, and employees and the owner-manager feel irreplaceable to conduct company activities and they renounce their right to be absent [29]. However, it is worth mentioning that, despite their organizational situation, SME employees seem to be more helpful [30]. In many cases, the employees know each other and share tasks at work, which favors the multiplicity of exchanges and mutuality at work [31], with low rates of interpersonal conflict [32].
1.1.1.2. Association between job control and presenteeism: According to Saijo et al. [33] job control was the DCS factor most related to presenteeism. Johansson and Lundberg found that the more an employee’s job decision latitude was high, the more likely he or she was to practice presenteeism. However, Aronsson and Gustafsson confirm that employees with low levels of decision latitude are more prone to presenteeism. Workers with limited levels of control are often found in lower line positions and may earn lower salaries, so are likely to feel more financially insecure and, as a result, may still go to work when they are sick [6]
Research has however shown that SMEs, and small enterprises (SEs) in particular, are often production units under a one-person management [34]. The simple organizational structures of SMEs demand the active involvement of their owner-managers in managing all operations, with low delegation of control. SMEs employees are basically dependent on their managers’ vision and behaviors. The SME is a mega-person as opposed to the mega-structure company [32]. The manager’s behavior, values, and beliefs mark their employees’ behavior, decision, and choices (social mimicry).
1.1.1.3. Association between social support and presenteeism: Generally, employees with good social support in the workplace are less exposed to presenteeism [6]. They trust the colleagues who will replace them during an absence and will help them to deal with what is likely to be a demanding workload on their return to work [6]. However, Caverley et al. [3] observe that having good-quality relationships with colleagues and managers can be a motivation to do engage in presenteeism. As a result, presenteeism may be adopted in close-knit work groups where employees may decide not to call in absent, out of empathy with their colleagues [3].
In the case of SMEs, the smaller size of SMEs and their simple structures facilitate social contacts between colleagues and owner-managers and promote a supportive work climate [32]. Employment relationships in SMEs are characterized by an affective, physical, and social proximity between owner-managers and employees with more degrees of informality [35].
The ERI model
Siegrist’s Effort-Reward Imbalance model of 1996 extends the assessment of psychosocial factors to include the concept of employee recognition, focusing particularly on the intrinsic motivations of employees, a factor that can potentially play a major role in workplace health [36, 37]. The theoretical basis of this model posits that efforts put by employees into their work one part of a reciprocal agreement under which they are given compensation (monetary reward, respect, and status) in return for those efforts. In situations where the work effort required is experienced as demanding while corresponding rewards are paltry, the resulting imbalance can lead to potential pathological reactions, either physical or psychological [37].
Despite several research studies on employee recognition in the workplace and its impact on mental and physical health [38], little research has been done on the impact of employee recognition on presenteeism. Research concerning reward and recognition in SMEs is also limited [39]. SMEs’ reward systems are complex [40], due to the rare, informal, and unstructured performance evaluations [40]. Other studies point to the unstable and short-lived nature of many SMEs [41], environments where the workforce is usually younger and less educated, and jobs far from secure [42]. In addition, the limited prospects for promotions [42] and the financial vulnerability of SMEs mean that employee reward systems are difficult to apply [42]. SMEs cannot offer competitive remuneration and offer mostly bonuses, commissions, and profit sharing as incentives. However, some studies noticed that SMEs highly valued non-material benefits (intrinsic motivation) [43]. Even where there exists an effort-reward imbalance, employees in SMEs continue to go to work when they are sick, both to maintain their jobs and ensure the survival of the business.
Presenteeism and mental and physical health
Presenteeism and depressive symptoms
The assessment of depressive symptoms is based on two indicators: a mood of depression and anhedonia (the loss of interest or pleasure in activities) [44, 45]. Studies have shown that people with depressive symptoms, particularly those who attribute those symptoms to their work, are more likely to engage in presenteeism [44]. These studies indicate that depressive symptoms increase levels of presenteeism, but presenteeism can constitute a potential risk factor for employee health [16]. The longitudinal research of Lu et al. [46] confirms the association between presenteeism and mental health. The longitudinal study of Gustafsson and Marklund [47], using a 10-item mental wellbeing scale which incorporated depression items, finds that presenteeism affects mental wellbeing, including depression. Cocker et al. [48] note that SMEs may experience the antecedents and consequences of depression more intensely than larger organizations, although research does show that, compared to employees of large enterprises, people working in SMEs have a higher likelihood of developing occupational diseases [49]. This leads us to formulate the following hypothesis:
Presenteeism and psychological distress
The term “psychological distress” covers a range of psychosomatic disorders, including anxious-depressive reactions, cognitive disorders, fatigue, irritability, and anxiety [50]. Ashby and Mahdon [51] notice that presenteeism is significantly associated with anxiety. Employees with a high level of presenteeism reported high levels of anxiety. The literature on the subject reveals that work-related diseases are more common in SMEs [52]. This would seem to indicate that existing mental health problems in SMEs risk becoming increasingly severe when employees engage in presenteeism.
Presenteeism and physical health. Presenteeism and MSDs
Musculoskeletal disorders (MSDs) are the result of an imbalance between what people’s bodies are physically capable of and the occupational demands and requirements of their workplace [53]. Gustafsson and Marklund [47] conclude that both presenteeism and absenteeism are predictors of future physical health complaints (e.g., pain in upper/lower back, shoulders hips, and wrists). More analysis revealed that employees with sickness, reporting both high presenteeism and absenteeism, had a higher risk for physical complaints [54]. In contrast, Lu et al. [46] found that there is limited evidence to propose that presenteeism may affect future physical health. Other studies have demonstrated the negative consequences of presenteeism on the physical health of employees [55]. The study carried out by Taloyan et al. [56] supports these findings by adducing that presenteeism is a potential risk factor for physical health in the workplace.
Presenteeism and self-perception of health status
Self-perception of health status is the term used to describe the self-assessment (or self-perception) employees have of their overall health, their judgement as to whether they are in a bad, reasonable, or good state of health [44]. Studies based on cross-sectional data suggest that higher levels of presenteeism are associated with poorer self-rated health [6]. Results show that presenteeism is a determinant of future poor self-rated health [9]. A review by Schultz and Edington [57] found that chronic health conditions are associated with presenteeism (productivity loss). Studies have shown that presenteeism can be both an indicator of greater levels of stress as well as a factor contributing to increased stress and psychological strain, both of which in turn affect employees’ self-perception of their health status [16].
Associations between different aspects of physical and mental health
Many epidemiological studies identify comorbidity between MSDs, psychological distress, and depressive symptoms [58]. Some of these studies find that chronic pain can lead to different forms and degrees of psychological distress, notably to depression [36]. In their longitudinal study, Dworkin et al. [59] show that depression and anxiety are predictors of a later development of chronic pain. Rajala et al. [60] confirm the fact that MSDs (in the form of neck pain) are more frequent in people with depressive symptoms. In terms of the relation between employee perceptions of their overall health status and their mental and physical health (especially psychological distress, depressive symptoms, and MSDs), Vézina et al. [44] report that 21% of employees suffering from work-related depressive symptoms describe themselves as being in bad health, whereas, among those with no depressive symptoms, the negative self-perception of their health status is 5.6%. There is also a higher prevalence of MSDs among employees with negative perceptions of their health status [44]. This leads us to propose the following hypotheses:
Impact of company size on psychosocial risks, presenteeism, and health
Some studies show that psychosocial and injury risk is greater among workers in SMEs, especially in small businesses [61]. SMEs are characterized with higher levels of job insecurity and employment cut-backs, and more acutely experience concerns about workplace health and safety (WHS) and human resources management [62, 63]. SMEs offer different working conditions from those in larger enterprises [63], with higher numbers of unionized employees and more stable job environments [19]. Some studies show that, because of their size, small enterprises are more exposed to problems health, injuries, and psychosocial risks [19].
Lechat and Torres [64] emphasize that the effect of the absence of the owner-manager in SMEs will not have the same impact in large organizations. Mahé de Boislandelle shows that a trivial event in a large company can produce negative effects in an SME. The absence of one employee can become a source of stress by cascading risk effects (one problem that leads to another) [27]. Due to the possibility of a butterfly effect of the theory of chaos, the effects of psychosocial constraints on presenteeism could be exacerbated. Similarly, presenteeism could have stronger effects on health in SMEs. The smaller the size of the firm, the more significant is the impact.
Figure 1 presents the conceptual model of this study. In addition to all the hypothesized relationships, the model includes associations between job demand, control, social support, and reward effort imbalance. These associations have been supported in previous studies on absenteeism [65] and mental health [66].

Proposed psychosocial determinants and correlates of presenteeism in SMEs.
Sample composition and data collection method
This study is based on data obtained through the Québec survey on working conditions, employment, and workplace health and safety, known by its French-language acronym, the EQCOTESST. The initial survey sample consisted of a total of 4,608 employees in enterprises in the Canadian province of Québec. Data were collected using a computer-assisted interviewing system (CATI). The survey sampling frame was established using random telephone number generation (RNG). The researchers sent letters of presentation on the survey in French and English to households corresponding to the phone numbers generated. To test the association between psychosocial risks, presenteeism, and health, only people working in SMEs of between 2 and 199 employees were included in the sample, giving a total of 2,525 SME employees surveyed. To better understand the differences in exposure to psychosocial risk and presenteeism, and the moderating impact of size on the relationship between psychosocial risks, presenteeism, and health, we took the original sample (4608) of the EQCOTESST.
Measurement instrument
The main questionnaire used for the EQCOTESST survey includes measurement instruments applied to a number of variables ranging from working and employment conditions, and respondent and job characteristics to presenteeism and mental and physical health [44]. Most of the statements used to measure the three variables of the DCS model were taken and adapted from the Job Content Questionnaire (JCQ) [67, 68]. Numerous studies have established the psychometric qualities of this instrument ([49]. The workload demand variable was measured through six statements, five of which were taken from the short version of the JCQ [68]. Respondents were asked to choose from four possible answers on a scale of 1 (strongly disagree) to 4 (strongly agree). The reliability level (0.72) of the measurement instrument was judged to be satisfactory for the workload demand variable. Five statements taken and adapted from the JCQ (Karasek, 1985) were used to measure job decision latitude. The reliability level (0.61) of this measurement instrument is close to the threshold limit value. Seven statements were used to measure social support in the workplace, six of which were taken from the JCQ and the seventh based on a Copenhagen survey on psychosocial factors in the workplace (COPSOQ) (“In my workplace, I feel I am part of a team”) (our translation), [50]. The reliability level (alpha de Cronbach 0.83) of the social support measurement instrument was also judged to be satisfactory.
Employee perceptions on effort and reward were measured using eight statements, six based on Siegrist’s Effort-Reward assessment instrument and the two others on the Copenhagen survey on psychosocial factors in the workplace (COPSOQ) [69]. In this case also, the reliability score (alpha de Cronbach 0.81) was deemed satisfactory.
Presenteeism was measured using the following question: “In the past 12 months, have you ever gone to work even when you felt you should have stayed away because you were sick? Yes, No (Never)”. Respondents who answered Yes were then asked a follow-up question to ascertain the number of total days they had been at work while they were not well: “In the past 12 months, how many days in total did you go to work while you knew you were sick?”.
Six survey statements from the Kessler Psychological Distress Scale [70] were used to assess employee health status. These statements asked how often employees felt ‘nervous’, ‘hopeless’, ‘fidgety’, ‘depressed’, ‘that everything was an effort’ or ‘worthless’. Respondents were given a choice of five possible corresponding answers: ‘None of the time’, ‘A little of the time’, ‘Some of the time’, ‘Most of the time’ or ‘All the time’.
The questions used to measure musculoskeletal disorders (MSDs) were based on a questionnaire developed by Kuorinka et al. [71]. MSDs were considered with reference to four areas of a person’s body: the neck area, the back, the upper limbs, and the lower limbs. For each area of the body, respondents were asked to specify how often they experienced pain there. A four-point response scale was used: ‘Never’, ‘From time to time’, ‘Often’ and ‘All the time’ [44]. The reliability level (alpha de Cronbach 0.83) of the measurement instrument was deemed satisfactory.
Depressive symptoms were measured using an index based on two symptoms: feelings of depression (whereby depression in the form of sadness or melancholy is assessed) and anhedonia (the inability to feel interest or pleasure in most normal activities usually found enjoyable) [72]. A diagnosis of severe depression is made when an employee is found to have both symptoms [72].
Self-perception (self-assessment) of the overall health status was measured using the statement: “In general, would you say your health is: Excellent, Very good, Good, Fair or Bad?”.
Analyses
To test the theoretical framework of this research, structural equations modelling was performed using EQS 6.1 software. The maximum likelihood method was applied to estimate the model and corrected statistics were used to accommodate non-normed data. An assessment of the fit of the overall model was carried out using the S-Bχ2 index, the Normed Fit Index (NFI), the Non-Normed Fit Index (NNFI), the Comparative Fit Index (CFI, [73]), the Incremental Fit Index (IFI, [74]), the McDonald Fit Index (MFI), the RMSEA and the Root Mean-Square Residual (RMSR). The fit of a theoretical model with observed data is considered good when the values of the, NFI, NNFI, CFI, IFI, and MFI indicators are above 0.90, those of the RMR and the Root Mean Square Error of Approximation (RMSEA) indicators are below 0.08, and the value of S-Bχ2 is non-significant (p > 0.05).
Differences in exposure to psychosocial constraints were tested using ANOVA analyses, and the moderating effect of size was tested with multi-group analyses. We classified the initial sample in three groups based on the respondent’s enterprise size: small-sized (SS), medium-sized (MS), and large enterprises (LS). The classification is based on the number of employees: 2 to 50 employees is considered a small-sized enterprise; 51 to 199 employees is considered a medium-sized enterprise; and 200 employees and more is considered a large enterprise [44]. Small-sized businesses, medium-sized enterprises, and large businesses count for around 38.72, 16.08, and 45.20 of the total sample, respectively.
Results
Testing the model
The test of model including only the hypothesized relationships was performed. The results yielded NFI, NNFI, CFI, and IFI index values of 0.774, 0.585, 0.781 and 0.783 respectively. All these values are below the acceptance threshold. Only the MFI value index was above the acceptance level (0.919). The RMR (0.086) and the RMSEA (0.094) values are all above 0.08. In addition, the value of the S-Bχ2 index (383.954) was significant (p < 0.001). Taken as a whole, these results indicate that the quality of the fit of the model with the observed data was not acceptable.
The results of the LM (score) test call for the inclusion of correlations between the variables in Karasek and Theorell’s theoretical DCS model and those of Siegrist’s ERI model. The literature in the field offers theoretical support for these changes. In effect, a number of studies show that a significant improvement in predictive power is obtained when the two models are used in combination [75]. Rydstedt et al. [76] identify highly significant associations between the components of the DCS model and the variables of the ERI model. A significant association can be established between job demands, control, social support and intrinsic and extrinsic employee recognition elements of the DCS model [76]. The study carried out by Harter et al. [77] shows that the DCS model is better able to predict absenteeism when used in combination with the ERI model. Yu Shan Fa et al. [78] report significant associations between all the variables of the DCS and the ERI models and depressive symptoms, in addition to a better predictive ability for depressive symptoms when the two models are combined. This same result was also observed in the study by Niedhammer et al. [10] who found a substantial increase in their ability to predict the appearance of depressive symptoms in workers when the two models were used in combination.
Consequently, correlations between the three variables of the DCS model and employee recognition were added to the initial model, with a resulting significant improvement in the fit of the model. For the NFI, NNFI, CFI, IFI, and MFI indices, values were 0.945, 0.895, 0.953, 0.954, and 0.982 respectively. The RMR and RMES values confirm the fit of the adjusted model.
The results confirm that correlations between the three DCS variables are all significant. There is a positive and significant association between job demands and job control (r = 0.165, t = 5.862). There exists a negative and significant association between job demands and social support (r = –0.048, t = –2.204), and a positive and significant association between social support and job control (r = 0.177, t = 7.542). In addition, the association between the three DCS variables and Effort-Reward imbalance are all significant (see Fig. 2).
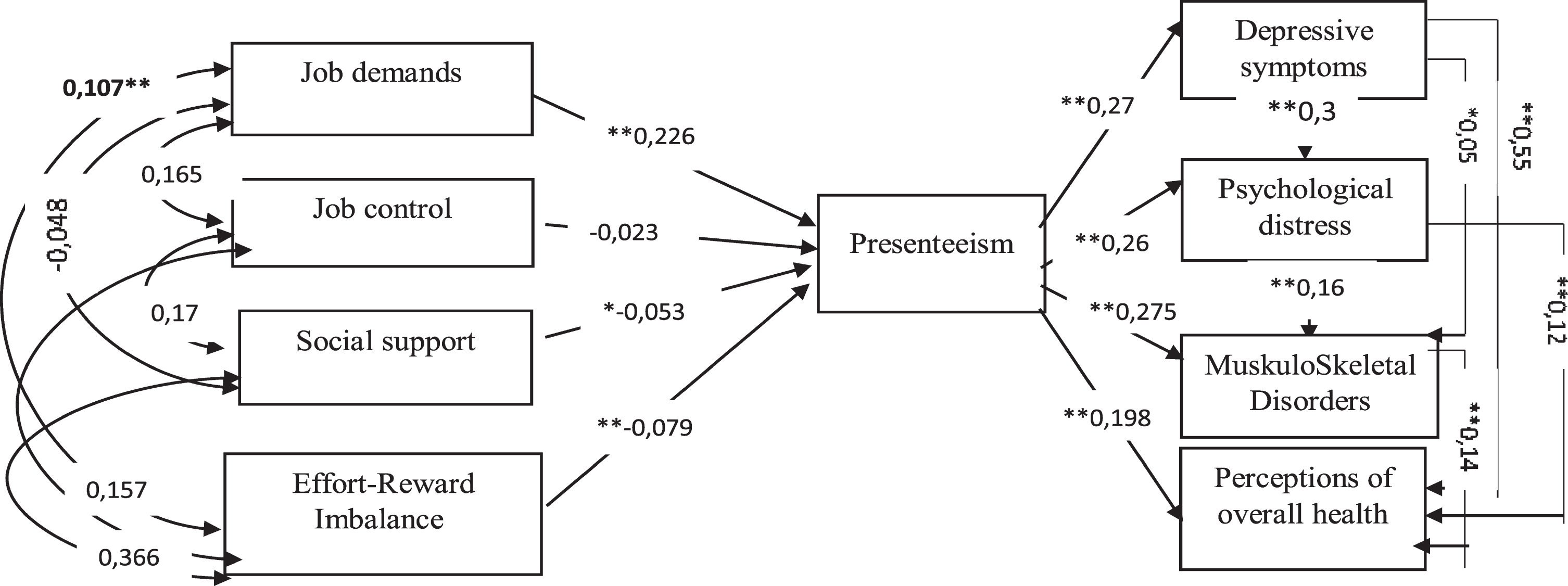
Results.
The results of hypotheses test are shown in Fig. 2. They report a positive and significant effect (β=0.226, t = 10.205) of job demands on presenteeism, so confirming Hypothesis H1a. However, Hypothesis H1b is negated since the effect of job control on presenteeism is negative, but not significant (β= –0.023, t = –1.056). Hypothesis H1c is confirmed, given the negative and significant effect of social support (β= –0.053, t = –2.305) on presenteeism. Hypothesis H2 is also confirmed through the negative and significant effect on presenteeism of the Effort-Reward Imbalance (β= –0.079, t = –3.425).
In terms of the health correlates of presenteeism, the test results reflect it’s positive and significant (β= 0.274, t = 11.154) effect on depressive symptoms, thus confirming Hypothesis H3a. The effect of presenteeism on psychological distress is also positive and significant (β= 0.269, t = 12.741), which confirms Hypothesis H3b. The positive and significant effect of presenteeism on MSDs (β= 0.275, t = 12.403) confirms Hypothesis H3c. In addition, the effect of presenteeism on employee perceptions of health status is also positive and significant, so confirming Hypothesis H3d.
Finally, the associations between the different aspects of physical and mental health are all significant. The results confirm the effect of depressive symptoms on psychological distress (β= 0.321, t =12.741), musculoskeletal disorders (β= 0.550, t =2.367), and perception of overall health (β= 0.550, t = 2.419), thus supporting hypotheses H4a, H4b, and H4d, respectively. The results support the impacts of psychological distress on musculoskeletal disorders (β= 0.162, t = 6.827), and perception of overall health (β= 0.122, t = 4.968). Hypotheses H4c and H4e are confirmed. Finally, H4f stipulating the effect of musculoskeletal disorders on perception of overall health is supported (β= 0.142, t = 6.421).
Globally, the ANOVA analyses show several differences in exposure to psychosocial constraints according to the size of the enterprise. Table 1 reports the results of the ANOVA analyses. The level of job demands is higher for large enterprises compared to small-sized ones. The social support level is higher for small-sized enterprises compared to medium-sized and large enterprises. The Effort-Reward imbalance mean levels were higher for small-sized enterprises. However, no significant differences between medium-sized and large companies were found.
Means difference for psychosocial risk factors and presenteeism
Means difference for psychosocial risk factors and presenteeism
aThe Scheffe’s Method is used for post-hoc comparison to find out which pair of means are significantly different. bMeans of subsamples are significantly different according to Scheffe test (p < 0.01). ©SS (small-sized); MS (Medium-sized); LS (large-sized).
To test the effect of business size on the presenteeism level, a crosstab was conducted. The Chi-square test is significant (12.412; p = 0.015). This means that presenteeism depends on company size. Even though the differences are not important, small-sized company employees report less presenteeism. In fact, those who report to work while they are sick represent 49.9%, 54.8%, and 55.0% of employees for small-sized, mid-sized, and large enterprises, respectively.
We also investigated the moderating effects of company size on the hypothesized relationships (Fig. 1). The results reveal a well-fitting multigroup model (S-Bχ2 = 251.586; df = 74; NFI = 0.922; NNFI = 0.916; CFI = 0.943; RMSEA = 0.024). Table 2 reports the (β) values for the hypothesized relationships for each group (i.e., small-sized, medium-sized, and large enterprises) and the results of the LM test of equality of variance. To identify the parameters that are not equivalent across the three samples (small size, medium, and large), we examined the probability values associated with the univariate incremental chi-square values. The results reveal that all the probability values are higher than 0.05. Therefore, all the parameters are equal across the three samples, which means that the causal model developed in this study is not moderated by company size.
centerline The moderating effect of company size on the relationships between psychosocial risk factors, presenteeism, and health
centerline The moderating effect of company size on the relationships between psychosocial risk factors, presenteeism, and health
*p < 0.05; **p < 0.001; ***p < 0.001.
Indeed, the results of the general test of invariance report a non-significant moderating effect of company size on the relationships between presenteeism and its four psychosocial determinants (χ2 = 6.046; p = 0.642). The results also show a non-significant moderating effect of company size on the relationships between presenteeism and its consequences (χ2 = 9.927; p = 0.270).
In this study, presenteeism is viewed as a result of exposure to psychosocial constraints based on the DCS and ERI models. It is also viewed as associated with both physical and mental health. An integrative model based on structural equations is suggested and showed a good fit to the data, thus supporting our hypotheses that job demands are positively associated (H1a) with presenteeism, and negatively associated with social support (H1c) and effort-reward imbalance (H2). Job control (H1b) is not associated with presenteeism. In line with our hypotheses (H3a, H3b, H3c, H3d), presenteeism is, in return, positively associated with depressive symptoms, psychological distress, musculosqueletal problems and a poorer self-rated health. Contrary to large businesses, employees in small businesses benefit from more social support, less job demands, and tend to be less enclined to adopt presenteeism behavior. However, employees in small business are more exposed to an effort-reward imbalance compared to employees in large businesses. Contrary to expectations, the business’s size does not moderate the strength of the relationships between psychosocial risks, presenteeism, and health. However, there are significant differences in the perception of psychosocial risks and presenteeism between small businesses and large businesses.
This study has several contributions. First, it represents one of the rare efforts made to explore the DCS and ERI models related to the realities of SMEs while highlighting the importance of psychosocial factors to better understand the prevalence of the phenomenon of presenteeism. Though they are more often used to call attention to the causal effects of psychosocial risk factors on health, the DCS and ERI models are valuable tools to further our understanding of presenteeism in SMEs. This study confirms the predictive value of these two models, as well as the existence of a significant and direct correlation between workplace organization variables and presenteeism. Clearly, along with increases in job demands comes increasing presenteeism. These results are in keeping with findings of previous studies [6]
The results of our application of the two models to the SME sector identify job demands as the most important of the four psychosocial risk factors associated with presenteeism. This finding is particularly disturbing, given that high job demands are a characteristic feature of the majority of SMEs [79].
Our research also confirms the negative and significant effect of social support on presenteeism in SMEs. The less support employees receive from co-workers or their superiors, the more likely they are to engage in presenteeism. This finding confirms the role played by social support in inhibiting employee presenteeism [6]. The literature on the subject indicates that employees who experience strong social support in the workplace are more likely to stay away than to go to work when they are sick [5], a finding that is particularly applicable to SMEs with their social and often family-like character that encourages mutual assistance and support. Even so, a supportive social climate of this kind will inevitably be undermined by overly high workload demands, understaffing, and failure to replace sick employees, as well as insufficient financial resources to make sick leave payments to employees. This kind of work environment damages the positive effects of a climate of social support and makes employees more likely to engage in presenteeism.
The study confirms the theoretical prediction that an imbalance between efforts and the rewards received in return (in the form of monetary retribution, respect, or status) is a signal that presenteeism is likely to occur in SMEs. Even when employers are limited in what they can pay in employee salaries, the effort-reward imbalance in SMEs does not really appear to detract from the commitment of employees to their firms. Recognition of their collective interest seems to take precedence over their individual interests and goals; it is the continuing employment and stability offered by their place of work that constitute the rewards for their work. These results are consonant with the findings of Baker-McClearn et al. [80] whose research shows that the satisfaction, employees gain from their work, together with their feelings of belonging, are factors explaining their decision to engage in presenteeism. Because it explores the correlations between the different determinants of presenteeism, the present study also represents a valuable contribution to the literature in the field. The factors linked to presenteeism in the DCS and ERI models exert a mutual influence on each other.
This research demonstrates that presenteeism can be better understood when these two theoretical models are combined, and their resulting interactions carefully analyzed. This further confirms the findings of previous studies on the significant improvement in the predictive accuracy of the two models when used in combination [76].
A further significant contribution of this present research study lies in our analysis of the correlation between presenteeism and the mental and physical health of employees [45]. The results of our study clearly reconfirm the fact that presenteeist behavior is associated with psychological distress, depressive symptoms, and MSDs, as well as increases a person’s self-perception of being in poor health. While our research is based on cross-sectional data, the relationship may become bidirectional over time. Our results bear out the conclusions of studies that demonstrate the negative impact of presenteeism on employee health [16]. This study also reflects the telling associations between psychological distress, depressive symptoms, and MSDs. Each one of these risk factors has a significant association with employee perceptions of their health status. As a result, our study also supports the premise of a strong correlation between mental and physical illnesses.
This research shows that exposure to three out of four psychosocial risks depends on company size. Small-sized enterprises are characterized by high levels of social support (support of the supervisors and colleagues), which may have both positive and negative impacts on presenteeism according to previous studies [6]. In fact, employee’s and supervisor’s exchanges of ideas, communication, and socialization increase employee satisfaction and commitment to the organization. Despite their organizational and psychosocial environment, SMEs, particularly small-sized enterprises, also offer a stimulating social and organizational climate [30].
This result can explain why employees in small-sized enterprises are less exposed to job demands. In fact, employees seem to be more supportive [30]. Employees know each other and share tasks at work, which favors the multiplicity of exchanges and mutuality at work [32], with low rates of interpersonal conflict [32]. The low exposure to job demands and high social support in Small-sized enterprises explain, in part, why employees are less exposed to presenteeism.
This research shows that employees of Small-sized enterprises are more exposed to effort-reward imbalance. It seems that the financial vulnerability and the absence of an evaluation system limit prospects for promotions and make more difficult the system of retribution (career opportunities and job security). Because of the lack of resources, Small-sized enterprises cannot offer competitive remuneration packages (global remuneration). But some studies noticed that SMEs highly valued non-material benefits (esteem, encouragement), because they cannot offer high salaries and social advantages to their employees. This study shows the importance of not considering SMEs as a homogeneous entity. Where does the utility of the concept of “Anti SME” developed by Torres [81]. In fact, SMEs are not automatically opposable to large companies. It seems that medium-sized companies operate like big businesses and have a similar psychosocial environment. Finally, the results show a non-significant moderating effect of company size on the relationships between psychosocial risks, presenteeism and health. This leads us to relativize the question of the specificity of the SME, in particular the impact of the size of the company on the practice of presenteeism.
The results show that the strength of the associations between RPS and presenteeism is not moderated by the company size. This implies that job demand, social support, and effort-reward imbalance, leads to presenteeism, no matter the company size (i.e., small-sized, mid-sized, and large enterprises). Future studies are encouraged to further examine these relationships and to consider other moderator variables such job category and business activity sector.
Limitations
As there have been almost no studies carried out in SMEs’ workplaces, further research is still needed to validate the hypotheses we have advanced, to improve our knowledge and understanding of issues such as exposure to psychosocial factors in the workplace, as well as presenteeism and its impact on health. Clearly, our findings should be interpreted with some caution. The analyses were based on cross-sectional data, so some longitudinal research would be extremely valuable to improve our understanding of how the phenomenon of presenteeism is evolving and to give us a better grasp of the different interactions involved.
Furthermore, in analyzing organizational factors under the framework used for the DCS and ERI models, the present study does not consider initial organizational factors or those which lead to increased presenteeism. It could also be useful to assess the role played by individual characteristics in employee choices about engaging in presenteeism. Aronsson and Gustafsson in fact show that individual standards and values can be different from those governing societies or organizations.
Moreover, exactly as has occurred in all other academic studies on the issue, our research focuses primarily on factors that explain presenteeism rather than on strategies to prevent it. Current academic research limits the range of options available to SMEs by proposing only highly circumscribed prevention measures that are also difficult to apply.
The goals of research on presenteeism should not be solely to determine the extent to which employees engage in the practice and to identify triggering factors. Research also needs to explore presenteeism prevention strategies and concrete steps for promoting occupational health. These may well be challenging issues to address in the SME context, given the absence of any specialized health structures, and their limited financial and material resources. Undeniably, such an approach creates an awkward dilemma for SME employees. Prevention strategies that encourage employees to stay away from work if they are sick are not particularly convincing if those same employees are fundamentally prevented from staying away because of problems surrounding their replacement.
Further research is still needed to better understand the unique contexts that characterize SMEs and to propose field-based preventive measures that would be more concrete and not solely theoretical in nature. To achieve this goal, future research activities will first need to focus on better assessing levels of presenteeism in SMEs and helping employees and owner-managers better understand the impacts of the phenomenon. There need to be more in-depth analyses on employee and owner-manager awareness of and concerns about the issue and, most important of all, on how different enterprises deal with employee presenteeism and whether there are effective prevention or training programs they already draw on to discourage the practice.
Conclusion
The current study highlights that SMEs, particularly small-sized enterprises, are somehow protected from certain psychosocial constraints such as high job demands, and low social support, but are more exposed to others such as effort-reward imbalance. The fact that presenteeism rates are lower in small-sized enterprises also supports the view that “small is beautiful”. However, the fact that the business size did not moderate the strength of relationships between presenteeism and its correlates suggests that SMEs should not be studied as a homogenic entity. Business size should not be the only focus, but perhaps be combined with for example business sector, structure, team and leadership processes. Nevertheless, the protected environment of small-sized enterprises in terms of presenteeism prevalence and psychosocial constraints raises questions on how presenteeism is studied as a negative phenomenon. In this respect, in their meta-analyses, Miraglia and Johns [82] point out that affective and positive experiences at work, and favorable attitudes towards work, promote the feeling of well-being at work. This well-being is often reflected in organizational citizenship behavior, and presenteeism could be an example of this behavior [82]. Presenteeism becomes, then, the behavior of satisfied and engaged employees [56], due to a stimulating work environment which could be exemplified in the context of SMEs.
Conflict of interest
None to report.
Funding
This work was supported by the Institut de Recherche en Santé et en Sécurité du Travail (IRSST) du Québec and by the Fonds de recherche du Québec - Société et culture (FRQSC) [184187].