
Abstract
BACKGROUND:
In the arboriculture sector, some activities are still manually performed by forestry workers, which result consequently exposed to a high risk of developing muscle skeletal disorders. The Italian Compensation Authority reported an increase of work-related tendinopathies and carpal tunnel syndrome in loggers, but screening protocols are not available yet.
OBJECTIVES:
The objectives were: a) to evaluate the prevalence of tendinopathies and carpal tunnel syndrome in a sample of loggers and b) identify a sound screening approach.
METHODS:
41 loggers and 41 paired control workers were recruited for a total of 164 hands. The protocol included 1) demographic data; 2) medical history; 3) identification of CTS symptoms through a questionnaire and a hand-chart; 4) upper limbs clinical examination; 5) Raynaud’s diseases questionnaire; 6) wrists ultrasound; 7) NCS of the distal median nerve.
RESULTS:
The prevalence of tendinopathies was statistically significant only in the non-dominant hand (75, 5% in the exposed group and 53, 6% in the non-exposed group). The prevalence of CTS was 32, 2% in the exposed group and 15, 5% in the non-exposed group. The questionnaire had a sensitivity of 56, 7% and a specificity of 75%. The hand-chart had a sensitivity of 30% and a specificity of 92%. The clinical examination had sensitivity of 30% and specificity of 80%. The ultrasound had a sensitivity of 70% and a specificity of 56%.
CONCLUSIONS:
Loggers are a population at risk of occupational hand and wrist disorders. The hand-chart could be considered, together with the questionnaire, as the best secondary prevention tool to diagnose CTS.
Introduction
About 10 million workers are employed in forestry worldwide, some working in the private sector such as lumberjacks, and others engaged in the public sector, dealing also with the management and conservation of the forest heritage. One third of the Italian surface is covered by forests, mainly managed by regional authorities and partially by private owners [1]. On the Island of Sicily, in the South of the Country, the total number of public and private forestry workers, mainly seasonal, is 28,000 [2].
Forestry workers are exposed to many risk factors such as awkward postures, repetitive movements, heavy lifting and vibrations [3, 4]. Despite an increase in mechanization, some activities like tree felling, delimbing and bucking are still carried out manually with chainsaws [5]. Hand-arm vibrating tools bring about an increased risk of upper-limb neurological, vascular, and musculoskeletal disorders known as hand-arm vibration syndrome (HAVS). Thus, in literature a greater prevalence of HASV together with other hand-arm pathologies such as tendinopathies and carpal tunnel syndrome (CTS) are reported [6–10].
INAIL, the National Institute for Insurance against Accidents at Work, reports that 63,16% of the total number of CTSs observed in the whole agricultural sectors are registered in silviculture, and also the burden of other tendinopathies is relevant [11]. Nevertheless, due to the lack of systematic workers’ health surveillance in the sector, the real incidence of these diseases is probably underestimated. Since research scarcely focuses on the forestry sector, it is fundamental to conduct studies addressed at refining approaches for early diagnosis and preventive strategies.
While tendinopathies are diagnosed using physical examination and ultrasound (with specificity over 85% but sensitivity less than 60%) [12], the diagnosis of CTS is not as straightforward. CTS’s diagnosis is primarily based on the medical history, the physical examination and various tools such as questionnaires, hand charts, ultrasound examination and nerve conduction studies, but none of these tools is sufficiently able to provide alone a certain diagnosis [13–15]. Nerve conduction studies (NCS) seems to provide the best results, with a sensitivity ranging from 80 to 90% and a specificity higher than 90% [13]. Physical examination, which consist especially of Tinel’s and Phalen’s tests, shows more discordant results according to different studies; sensitivity and specificity for Tinel’s sign range from 38 to 100% and from 55 to 100% respectively. Likewise for the Phalen’ test sensitivity and specificity ranges from 42 to 85% and from 54 to 98% respectively [16].
Ultrasonography (US) of the median nerve has a sensitivity of 77.6% and specificity of 86.8% [17], which could be further increased respectively to 95% and 100% using high resolution technique [18]. The specificity and sensitivity of the symptom questionnaire are reported as 92,6% and 61% respectively [19].
Since the gold standard for diagnosis, NCS, cannot be performed in the periodical workers’ health surveillance at the workplace, and workers better tolerate other approaches, it is fundamental to identify an alternative adequate for screening activities and secondary prevention. This was the first aim of our study. A second objective has been evaluating the prevalence of tendinopathies and carpal tunnel syndrome in a sample of forestry workers.
Methods
A total of 65 workers were randomly selected among the loggers active in the province of Enna, employed in the Department of Forestry of the Region of Sicilia (“exposed”). The subjects were asked to participate to the study by the Health and Safety manager of the Forestry Department, who sent them an official invitation by e-mail. Twenty-four workers declined the invitation. As for the controls, 41-paired subjects engaged as clerks in the public administration of the Region were asked to participate and accepted. Among the 106 subjected asked to participate, the response rate was 77, 35%. The present cross-sectional study involved a total of 82 male subjects (41 loggers and 41 clerks).
Before the beginning of the survey, each participant was informed about methods and objectives of the study and signed an informed consent to participation. The protocol was previously approved by the Ethical Committee of the University Hospital G. Martino of Messina.
Selection criteria for the loggers group included: a) age between 18 and 65 years; b) a minimum of three years of working experience as chainsaw operator; c) no musculoskeletal surgery or any upper limb related diagnoses within the last three years from the start of the survey. Controls were paired for age, gender and BMI. Eligibility criteria was not being involved in any activity that might cause a biomechanical overload of wrists or having had any musculoskeletal surgery or upper limb related diagnoses within the last three years prior to the beginning of the data collection.
The study protocol included: 1) demographic data collection (gender, age, working experience); 2) Possible presence of a secondary job. In case of affirmative answer, the sector of the secondary job was identified as follows: primary sector (extraction and production of raw materials), secondary sector (manufacturing), tertiary sector (services); 3) anthropometric measurements (height, weight); 4) medical history; 5) identification of CTS symptoms through the administration of a questionnaire and a hand chart [20, 21]; 4) clinical examination of the upper limb through Tinel [22], and Phalen[23] test; 6) administration of a questionnaire addressed at pointing out the presence of Raynaud’s disease [24] and, where appropriate, cold test [25]; 7) ultrasonography (US) imaging of the wrists; 7) nerve conduction study (NCS) of the distal median nerve.
All objective testing was carried out at the participants’ workplace. In particular wrist was investigated by US and the possible presence of CTS through: (i) NCS, which is the diagnostic gold standard; (ii) the clinical examination of the upper limb, the clinical questionnaire, the hand chart, and the wrist US, which have been all used as secondary prevention tools. The study protocol anticipated the assessments of both limbs in each subject, upon identification of the dominant side. Statistical analysis was performed separately for dominant and non-dominant limbs, for a total of 164 observations.
CTS Questionnaire and hand chart
The questionnaire was used to collect information regarding the duration and characteristics of symptoms (constant vs intermittent and onset), and symptom’s functional impact on working ability, if any. This section was completed with a hand chart [20, 21], where the workers were asked to colour the areas affected by symptoms such as tingling/numbness, burning, weakness, or pain. Workers were also asked to rate the severity of their symptoms on a Visual Analogic Scale from a minimum of 0 (absence) to a maximum of 10 (severe). The questionnaire was considered positive for CTS in those who reported the presence (severity≥1) of at least one of the four symptoms evaluated in the last month before the examination in the first three fingers of the hand.
Clinical examination
The clinical examination consisted of Phalen’s and Tinel’s tests, performed on both limbs. The assessment was positive in case of presence of at least one sign in one limb.
Raynaud’s disease questionnaire
The possible presence of Raynaud’s disease was investigated through an algorithm that included two questions (1. Are your fingers unusually sensitive to cold? 2. Do you observe the presence of changes in the colour of your fingers after exposure to cold?) and some diagnostic criteria. In case the worker responded affirmatively to these questions, upon the identification of at least 3 diagnostic criteria, a cold test would have been performed [24].
Ultrasonography
As above mentioned, workers exposed to biomechanical overload may be at risk to develop wrist tendinopathies. The current evidences related to the use of US for studying tendinopathies in the forestry sector are very poor. Some authors use US to investigate wrist flexors [12], but also use of vibrating tools, such as chainsaw, might impact on the whole hand. In this view, in our study we focused both on wrist flexor and extensor tendons. In addition, we evaluated the radiocarpal joint and the median nerve at the proximal carpal tunnel (at the level of the pisiform bone). The investigation consisted in the collection of static images in both dorsal and ventral wrists.
A trained sonographer performed the US examinations according to the European Society of Musculoskeletal Radiology’s criteria [26], with a portable device (Venue Scan, Venue 40, GE Healthcare®) at the loggers workplace. Diagnostic criteria for tendinopathies such as tendinitis or tenosynovitis was the presence of at least one of the following changes: increasing in the tendon’s size, presence of hypoechoic areas in the tendon’s structure, presence of calcific metaplasia or increasing in the anechoic signal of the synovial space [12].
The classification of the results regarding median nerve assessment was based on its cross-sectional area [27, 28] as follows: “negative” if the area was less than 0,10 cm2, “positive” if it was greater than 0,10 cm2.
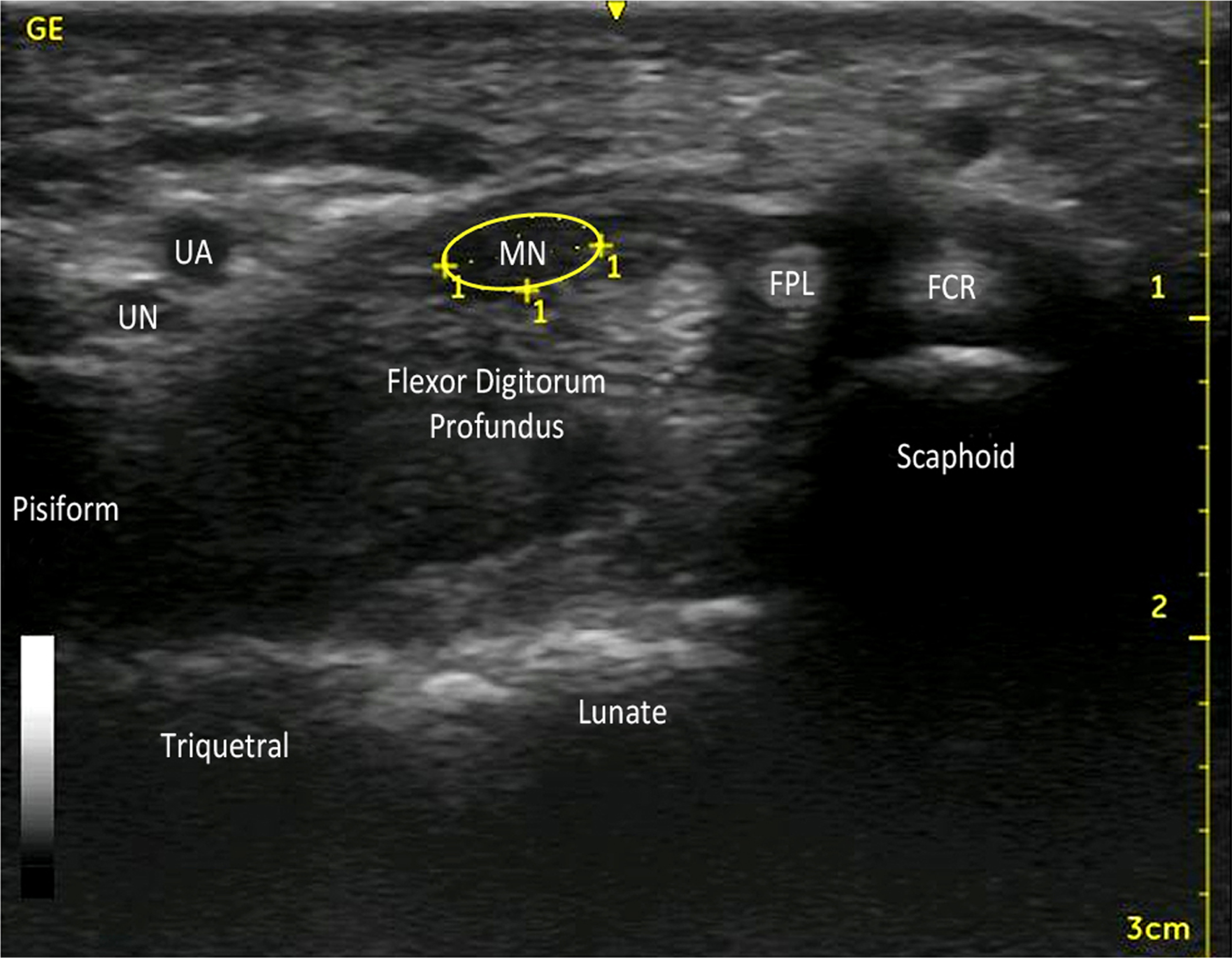
Ventral wrist (proximal carpal tunnel). UA: Ulnar Artery; UN: Ulnar Nerve; MN: Median Nerve; FPL: Flexor Pollicis Lungus; FCR: Flexor Carpis Radialis. Circled in yellow the Median Nerve’s cross-sectional area, considered negative if < 0, 10 cm2 and positive if≥0, 10 cm2.
The NCS was performed using a portable electroneurography device (model Medelec Synergy®) and disposable surface recording electrodes on both hands of each participant. The examination was conducted by a neurologist who, although aware of the label of each subject (i.e. loggers vs office workers), was blinded to the results of the remaining assessment. For each participant, we studied the motor and sensitive component of the median nerve bilaterally. In case the test showed evidence of carpal tunnel syndrome (CTS), the subjects underwent an electroneurographic study of the ulnar nerves to exclude an underlying polyneuropathy. All electroneurographic examinations were performed with the subject sitting next to the operator and forearm resting on a rigid surface in a supinated position. Normality values, diagnostic criteria, and fittings for conduction were used, following contemporaneous standards [29].
Median neuropathy at the wrist was defined by sensory peak latency > 3.5 ms and motor distal latency > 4.4 ms. No abnormalities on the ulnar nerves examined were found.
Data analysis
The statistical analysis was performed using the program SPSS PC version 25. Statistical significance was set for a P-value≤0.05. Pearson’s X2 was used to assess specificity and sensitivity of the protocol’s tools and to evaluate the prevalence of both tendinopathies and CTS. US investigation was conducted considering all 164 hands (82 dominant hands and 82 non-dominant hands), while CTS’ analyses were conducted considering 130 hands (63 dominant hands and 67 non-dominant hands) as 34 hands could not be examined using the NCS.
Results
The present study involved 41 exposed workers paired with 41 non-exposed workers for a total of 82 subjects. The subjects in the exposed group were aged between 46 and 65 years while controls were aged between 44 and 64 years. The working experience ranged from a minimum of 18 years to a maximum of 43 years in both groups. BMI was 27, 5 in the exposed group and 26, 6 in the non-exposed group. All 82 workers were right-handed. The most represented secondary job was in the primary sector (46%) for the exposed group while for the non-exposed group was in the tertiary sector (46%).
The prevalence of tendinopathies diagnosed with US was 68, 2% in the exposed group and 62, 2% in the controls. This difference did not reach the level of statistical significance (P > 0,05). As for the difference between dominant and non-dominant hand, we failed to find a statistically significant difference between exposed and controls for the dominant hand. Surprisingly, we found a statistically significant difference in the prevalence of tendinopathies in the non-dominant hand between the study groups (75, 5% in the exposed and 53, 6% in controls, P = 0,038).
Individual characteristics of study subjects
Individual characteristics of study subjects
Prevalence of tendinopathies diagnosed with US in total hands, dominant hand and non-dominant hand
Considering both hands (130), the prevalence of CTS diagnosed with NCS was 32, 2% in the exposed group and 15, 5% in the non-exposed group (P = 0,024). No statistically significant difference was found in the dominant and non-dominant hand between the study groups.
Due to their hypersensitivity to the NCS, in some subjects neurography was not performed. In particular, in 14 subjects (9 loggers and 5 office workers) we could not evaluate both limbs, and in 6 subjects (4 loggers and 2 office workers) we could evaluate one limb only, thus resulting in data missing for 34 wrists (19 dominant hand and 15 non-dominant hand).
According to the questionnaire results, 15 % of the exposed hands and 9% of the controls’ hands were reported to be continuously symptomatic, while the rest were not. The average duration of the symptoms for the exposed group was 4.8 years while for the controls was 3.2 years. Nevertheless, the presence of the symptoms did not affect their workability.
Prevalence of CTS diagnosed with NCS in total hands, dominant hand and non-dominant hand
Finally, to the aim of evaluating the sensitivity and the specificity of each diagnostic approach, we compared the single tests’ results with the gold standard for CTS, that is NCS (Table 4). We found that:
The questionnaire had a sensitivity of 56, 7% and a specificity of 75% with a positive predictive value (PPV) of 40, 5% and a negative predictive value (NPV) of 85, 2% (p = 0,001). The hand chart had a sensitivity of 30% and a specificity of 92% with a PPV of 52, 9% and an NPV of 81, 4% (p = 0,001). The clinical examination had a sensitivity of 30% and a specificity of 80% with a PPV of 31% and an NPV of 79, 2% (p > 0, 05). The measure of the median nerve’s cross-sectional area had a sensitivity of 70% and a specificity of 56% with a PPV of 32, 3% and an NPV of 86, 2% (p = 0,012).
None of the workers under study gave positive answers to the questions related to Raynaud’s disease.
Correlation between protocol’s tools and NCS results. (1) Correlation between questionnaire results and NCS results; sensitivity = 56,7%; specificity = 75%; PPV = 40,5%; NPV = 85,2%; (2) Correlation between hand chart results and NCS results; sensitivity = 30%; specificity = 92%; PPV = 52,9%; NPV = 81,4%; (3) Correlation between clinical examination results and NCS results; sensitivity = 30%; specificity = 80%; PPV = 31%; NPV = 79,2%; (4) Correlation between ultrasound results and NCS results; sensitivity = 70%; specificity = 56%; PPV = 32,3%; NPV = 86,2%
Our study aimed to investigate the prevalence of tendinopathies and carpal tunnel syndrome in a sample of forestry workers and identify the best screening approach by evaluating sensitivity and specificity of the available tools in CTS’s detection.
The US results showed a higher prevalence of tendinopathies in the non-dominant hand of the exposed group, compared to the non-exposed group (P = 0,038). In line with Attebrant et al. [6], van Rijn et al. [7], Calvo et al. [30], Da Costa et al. [31] and Colombini et al. [32], this result suggests that the development of tendinopathies may be caused by the bimanual chainsaw’s use as it’s supported by the non-dominant hand, with the arm raised and the hand in grip position right above the engine.
The NCS showed a higher prevalence of CTS in the exposed group (32, 2%) compared to the non-exposed group (15, 5%) as expected. This data is in line with what has been reported by other authors [8, 33], confirming that forestry workers are a population at risk of CTS as previously stated by van Rijn et al. [7] and Attebrant et al. [6]. The prevalence found in our study is higher than what described in literature, but this difference can be attributable to a different experimental approach adopted. In particular, the study of Bovenzi and co-workers is focused mainly on hand-arm vibrations rather than other risk factors [33]. Additionally, the study group was investigated mainly with questionnaire and objective assessment, whilst NCS was conducted only in a selected group of workers and US was not performed [33].The questionnaire reported a sensitivity of 56, 7% and a specificity of 75% with a positive predictive value (PPV) of 40, 5% and a negative predictive value (NPV) of 85, 2%. This result is in line with the 66% false-positive rate found by our group in 2017 in the same population [34]. Given the specificity of the questionnaire, it could be considered as a useful secondary prevention tool, also according to what described by Franzblau et al. [35] in metalworkers, Masci et al [19] in milking parlour workers and Fischer et al. [36] in a population of patients after CTS surgery.
Among the tools we included in the protocol, the sensitivity of hand chart was 30% and the specificity 92% with a PPV of 52, 9% and an NPV of 81, 4%. These results are very close to the ones found in the studies conducted by Katz et al. who found a specificity of 90% [37] and 73% [20]. We can assume that this tool might be considered the more suitable choice to evaluate CTS symptoms and perform screening activities among the workers, as also supported by Levine et al. [21] and Werner et al. [38].
The clinical examination had a sensitivity of 30% and a specificity of 80% with a PPV of 31% and an NPV of 79, 2%. These results are similar to Kuhlman and Hennessey’s findings, pointing out a sensitivity of 23–69% and a specificity of 66–87% [39], and with those of Franzblau et al. [35]. This last study in particular, evidenced that less than half subjects with confirmed CTS resulted positive to clinical signs. We finally can agree with Brüske et al. [16] in saying that the usefulness of clinical signs is limited for screening purposes, where main aim is the identification of early and very mild changes.
The measure of the median nerve’s cross-sectional area had a sensitivity of 70% and a specificity of 56% with a PPV of 32, 3% and an NPV of 86, 2%. The specificity and sensitivity pointed out by our study is however minor compared to the findings of Fowler et al. [17] (86,6% and 77,6% respectively) and to the 97% sensitivity found by Mhoon et al [40], but our study’s specificity is greater than the 43% found by Nakamichi et al. [41]. In line with Mhoon et al. [40], Torres-Costoso et al. [42], Billakota et al. [43] and El Miedany et al. [44], we suggest that US could be used as a diagnostic tool for CTS’ screening directly at the loggers’ workplace, in place of evaluate them at the hospital.
As we noted performing this study, NCS isn’t well tolerated by all workers because some may feel pain during the examination. Therefore the US, with a sensitivity of 70%, together with the hand chart performed in the workplace could represent a good screening tool. This might allow the avoidance of NCS and hence pain for the worker. This is very important for a screening tool which should be acceptabile for the populations under study and limit at the minimum the annoyance.
We did not find any difference in prevalence for Raynaud’s phenomenon as it was absent in all the workers under study. Our results are in agreement with Bovenzi et al.’s study [33] which did not find differences in the prevalence of cases in both exposed and controls. His study in fact reported some cases that can be attributed to the different climatic conditions existing in the north cold mountain climate compared with the warm climate of Sicilia. The presence of Raynaud’s disease should be investigated further as its total absence is against what’s described in the literature by Nilsson et al. [45] and by Shen et al. [46].
This study has some limitations, our sample of 82 workers is quite small and the exclusion of some subjects from the NCS contributed to diminishing the sample’s size. We assumed that each hand was independent from the other, but this is not necessarily true and may have induced a bias in our results. Besides, US investigations are operator-dependent and often influenced by their ability and experience.
Conclusion
The study confirms that forestry workers are a population at risk of occupational hand and wrist disorders, and further studies are advisable. Further surveys might be conducted with an experimental approach protocol able to integrate questionnaire, hand chart and US.
In fact, the questionnaire together with the hand chart allow to quickly and easily evaluate many workers and to exclude those not worthy of further clinical investigation. US, with a sensitivity of 70%, represents a protocol second step which grant to identify wrist-hand disorders and avoid negative tested workers to undergo NCS (US NPV:86%). The questionnaire should be addressed also at pointing out possible cases of Raynaud’s disease.
Footnotes
Acknowledgments
The authors would like to acknowledge the Forestry Department of the Province of Enna and the Health and Safety managers whose collaboration was crucial for the realization of the study.
Conflict of interest
The authors declare no conflict of interest.