
Abstract
BACKGROUND:
Hotel room cleaners are disproportionately exposed to hazards that increase risk for poor health outcomes. Interventions are needed to improve the health of these workers. Yet we know little about the expressed needs of hotel room cleaners nor do we know about managers’ perspectives on how to best optimize employee health.
OBJECTIVE:
We aimed to develop an understanding of perceived intervention needs among hotel room cleaners and to assess managers’ views on the acceptability of the proposed interventions.
METHODS:
We used a community-based approach to recruit study participants. We conducted five focus groups among hotel room cleaners and individual interviews with hotel managers. Interviews were audio-recorded, transcribed, and analyzed using content analysis.
RESULTS:
The workers expressed needs centered on pay, workload, appreciation, ergonomics, chemical and biological hazards, nutrition, smoking cessation, exercise, mental health and stress management. In addition to echoing the workers’ expressed needs, managers emphasized employee retention and financial literacy.
CONCLUSIONS:
To our knowledge, this is the first paper to include both workers’ and managers’ accounts on intervention approaches that will optimize health and wellbeing. This paper offers a guide for future program development among hospitality workers. Effective interventions need to be integrated, encompassing the individual, intrapersonal, organizational, and policy levels.
Keywords
Introduction
Hotel workers, specifically hotel room cleaners (HRCs), are integral to the ever-expanding hospitality and tourism industry in the US [1, 2]. These employees are often exposed to a range of occupational hazards which lead to negative health outcomes [3–7]. HRCs (also known as hotel housekeepers) experience higher rates of occupational injuries (7.87 cases per 100 workers) compared to other workers in the industry such as banquet servers, steward/dishwashers and cooks/kitchen workers (2.82, 5.97, 5.99 cases per 100 workers, respectively) [8]. Likely as a result of these hazards, between 47 and 68% of room cleaners reported chronic pain (i.e. back, neck, and shoulders) [9–11].
Interventions targeting hotel workers [12–19], including the recent California ergonomic standards [20], for HRC have focused on decreased injury claims, decreased anxiety, and improved cardiovascular disease risk indicators such as body mass index [12–20]. However, aside from the California ergonomic standard, only one of these studies alluded to worker input in the intervention’s design or implementation [18]. There is a dearth of participatory action approaches in addressing the health and wellbeing of vulnerable workers. Such approaches ensure active engagement, foster intervention success, and improve sustainability [21]. Interventions targeting hazards and wellbeing among hotel workers, particularly HRCs, would benefit from taking into account worker-specific suggestions, and expressed needs. We report findings from a study on expressed intervention needs from HRCs and hotel managers.
Theoretical framework
This study is informed by the Social Ecological Model (SEM) which comprises the micro (individual-interpersonal), meso (intrapersonal), exo (neighborhood, community), and macro (cultures, policies) systems. With SEM, we need to consider the individual, interpersonal, institutions/organizations, community and structures, policies, and systems levels factors. By integrating individual characteristics and context, SEM provides us the opportunity to take a holistic approach to understand our stressor-outcome relationship and thus will allow for a comprehensive and well-tailored intervention encompassing all aspects of workers’ lives [22]. This framework, anchored within a participatory action lens, informed the interview guide to identify worker’s expressed intervention needs across multiple SEM levels.
Methods
Recruitment
Following approval from an Institutional Review Board (IRB), flyers were distributed in hotels throughout two major cities. We also recruited participants through snowball technique.
Setting
Two English focus groups were conducted at two hotels (in a conference room and a breakroom) with managers’ permission. No managers were present during the interviews. The three Spanish focus groups were conducted in a participant’s home.
Measures
Interviews were guided by the SEM, which enabled us to explore intervention needs at multiple levels. Probing questions related to participant’s concerns about their health, at work, outside of work, and at home. Examples include: What is the number one thing you are worried about the most right now?; How do you feel about your overall health?; What resources are in place at work right now that target the health of workers?; What are the key topics that would matter to you the most in a program?; and What is the ideal time and location that would work for you, if you were to participate in a program?
Data collection
Each participant provided written consent. The interviews ranged from 60 to 90 minutes. A certified Spanish translator moderated the Spanish focus groups. During each focus group, additional research team members observed and took notes, paying close attention to the dynamics of the conversations as well as non-verbal cues. Managers who expressed interest in the study participated in individual phone interviews. Each individual phone interview was audio-recorded. At the end of the interviews, each participant received a $50 gift card for their time.
Data analysis
All the interviews were transcribed verbatim. Graneheim and Lundman’s approach guided the data analysis [23]. Each transcript was read, and key passages were highlighted. Interpretive and condense meaning units were developed from each of the highlighted passages. Lastly, themes were developed. To assure rigor, each transcript was analyzed by two coders, who after coding met with a third research team member to discuss and address any discrepancies.
Results
Participant characteristics
Two English and three Spanish focus groups were conducted among HRCs and six individual phone interviews were conducted among hotel managers. Each focus group comprised between four and six individuals. One HRC and two managers were male. Focus group participants reported experiencing chronic pain (n = 11), diabetes (n = 4), hypertension (n = 3), asthma (n = 2), depression (n = 2), and high cholesterol (n = 1). Health issues among managers include sinus problems, back pain, hypertension, and chest pains.
Room cleaners’ expressed needs
Participants noted intervention needs that could be divided into two categories: 1) work specific and 2) health related. Each category is detailed below.
Work-specific needs
Work-specific needs included increased pay, workload balance, strategic planning, increased opportunity for work hours, and employee appreciation or motivation programs.
3.2.1.1. Increased pay. Participants observed that the current pay rate does not suffice to pay bills which was a point of stress. For example, one participant stated, “I would say that my ends are not met right now. My bills are like double what I make. So that’s kind of stressful” (E2P2). Participants reiterated that increased pay would benefit their health. Those in the Spanish focus groups were especially forthright about how their low wage prevented them from keeping up with their medical expenses. Many reported that despite receiving assistance from local health clinics they struggled to make ends meet. One participant explained, “I receive help from the Health Clinic... I don’t get medical prescriptions, my pills cost a hundred and something” (S1P1).
3.2.1.2. Workload balance. Participants indicated the need for improved room assignments and more time to complete tasks. For example, a participant stated, “the biggest stress is when you are assigned too many rooms that you don’t know if you can finish them or not” (E1P2). Others described the physical demand associated with the high workload, reporting that they would often be over-exhausted from cleaning too many rooms. Participants reported having to clean even up to “thirty-five rooms in one day” (S3P4). And one participant in particular described, “when you get too many rooms assigned, your blood pressure increases” (S1P1).
3.2.1.3. Strategic planning. Participants also indicated the need for strategic planning relating to assignments and scheduling. Specifically, they expressed the need for more consistency in room assignments since the constant rotation in the room assignments results in loss of tip compensation. Participant 4 from the third Spanish focus group explained:
“When you’re assigned to the same section for 3, 4, 5 days, it’s not that you think you’re perfect, but they usually give you a tip, for sure. But then if you’re moved to another area, the person left in your place may not clean as well, or did not clean there before, and wasn’t even the one who had cleaned the room, that person gets it.”
3.2.1.4. Increased opportunity for work hours. Participants were not allowed to work more than 40 hours a week, which did not meet their financial demands and the need to care for their family. Several participants noted that their work hours significantly decrease during off seasons, with one participated stating:
“With the reduced hours we wonder if there will be any work to do. Because last year we barely made ends meet with one bi-weekly check considering that we were only dismissed one day...There’s stress because there won’t be much work to do. One of my paychecks is for rent and the other one for bills and I can barely make ends meet because there’s not much work to do there and I begin to stress out” (S2P3).
3.2.1.5. Employee appreciation and motivation programs. Participants desired an approach to motivate the workers as it would be beneficial in managing stress and maintaining a healthy workplace. For example, a participant explained that motivation was key to managing stress, saying, “I think that many places do something in the morning to motivate people... It would help manage stress...That in itself helps you deal with stress better” (E2P6). She affirmed that a reward system would benefit employee motivation and positive mental health outcomes. She described her past experiences on how motivation tactics improved her mood:
“I used to work cleaning houses, and the lady in charge would celebrate all the moms on Mother’s Day, take us out to eat to a restaurant...The place they chose is not as important as making sure they show us how much they appreciate us.” (E2P6)
Health-related needs
Health-related needs include ergonomics, nutrition, exercise, smoking cessation, mental health and stress management.
3.2.2.1. Ergonomics. Participants stressed that existing training did not adequately focus on ergonomic methods and as a result would suffer musculoskeletal injuries. One participant brought up the fact that employees would repeatedly ask management for ways to avoid injury. Participants observed that even after multiple injuries, there were few attempts to implement ergonomic training programs. Furthermore, participants suggested implementing a program to prepare them for the rigors of the day and to reduce chronic pain. Without such programs, participants resort to taking pain medication on a regular basis. One participant stated, “I have to take pills every morning so that I can stand the pain” (S2P4).
3.2.2.2. Nutrition. Participants reported having difficulties with their dietary regimens. This was of particular concern for those whose regiment was crucial for their health (i.e. with diabetes). One participant noted that her “sugar is acting up” and that she doesn’t fully understand her diagnosis or how to adjust her diet accordingly. Another participant, who was recently diagnosed with diabetes mentioned that she was provided an informational brochure on nutrition but did not know how to initiate the necessary change:
“Teach me how to eat healthy or you can do some information about it...For somebody that knows nothing about this disease and trust me I know nothing...but I would love to learn more about it.” (E1P4)
3.2.2.3. Chemical and biological hazards. Participants experience daily contact with biological and chemical waste, such as bodily fluids and needles left by hotel guests. Yet for many there are no specific procedures in place to protect themselves. For example, one participant reflected that she was not taught how to deal with chemical mixing and spent every work shift working with them, saying, “we don’t know what sort of chemical reaction these liquids will have by getting mixed with one another” (S2P4). Another participant discussed injuries resulting from prolonged chemical exposure due to a lack of safety protocols. She explained, “This hand was much damaged at some point, and now I can’t touch any strong chemicals or soaps because my hand will get extremely dry” (S3P2). This participant directly noted the need for an education program to address this need.
3.2.2.4. Exercise. Participants highlighted the need for programs on physical activity. Many affirmed that they did not know how to properly exercise and that physical stress management techniques would be beneficial. Also, participants suggested that implementing an exercise program would improve their strength and reduce injuries related to pushing, pulling, and lifting heavy objects. For instance, one participant asked for time delegated to stretching or yoga before starting the shift so they would be better prepared to deal with the heavy lifting they would face in their shift. She stated: “I think it would be good if we were given about 15 minutes, before starting to work [for] stretching muscles and all that” (E1P4).
3.2.2.5. Smoking cessation. Many participants reported being chronic cigarette smokers, with some having started at early ages. They noted that a workplace program would be the most effective due to the amount of time employees spent there. One participant said about a program, “yes to see how I can quit smoking” (E1P1). Other participants viewed smoking as a way to deal with stressors encountered in their workplace, yet desired to quit. For example, this participant who reported smoking a pack and a-half of cigarette a day stated: “I need to find something else to start destressing myself and I don’t smoke weed, I just smoke cigarettes, but, that’s not the answer, what I’m doing either” (E2P3).
3.2.2.6. Mental health and stress management. HRCs are often operating on a tight schedule, which combined with other stressful workplace factors, often lead to increased anxiety. One participant stated: “Well, it affects you because you gain weight due to stress at work and then sometimes we don’t eat. I was still fat, so I believe that it’s all due to the same stress at work” (S2P1). Participants noted that a class could help improve mental health status, explaining, “So that we can learn how to love ourselves” (S2P4) and “...to help us improve our self-esteem” (S2P2). Further, meditation was proposed by more than one participant as a method for dealing with overbearing emotions from workplace stress.
Managers’ expressed needs
Many of the intervention needs the managers identified mirrored those of the room cleaners. However, the managers’ focuses were primarily for the workers and less for themselves, especially when it came to health needs. Similar to the HRCs, the managers highlighted the need for training on ergonomics, nutrition, smoking cessation, and better pay. They observed that the high rates of smoking among the employees was affecting their health:
“But I would love to see a program that would help them, that would get them some classes to help them not smoke as much or just completely stop smoking. Because I think when I see them and their health, I think the smoking has a lot to do with it.” (M1).
For themselves, managers identified the need for employee retention, appreciation, physical activity and financial literacy. Given the physical demands of hospitality work, there is high employee turnover and managers reflected on how this high turnover rate leads to stress, underscored by the following statement: “I get the most worry or stress just if somebody was to call off and I didn’t have enough staff. Or if the counts go way up and I don’t have enough staff or no one to help me” (M4). A clear employee retention program would be beneficial. Managers also highlighted the importance of appreciation and positive feedback from employees and upper management.
Furthermore, managers expressed a desire for increased physical activity since most of their workday is spent at a desk. One manager explained, “I work at my desk mostly, when we have crazy busy days, I’m usually running around a little bit more, but I do have to force myself to get up and get moving” (M3). Suggestions included employer-subsidized gym discounts. Lastly, the managers communicated the need for programs on financial literacy, specifically related to how to save and invest money. For instance, one manager stated, “As far as investing money, I would like to learn about stocks and selling trade and stuff like that, you know, as far as investment” (M5).
Proposed mode of delivery: Room cleaner and manager perspectives
Most participants in this study indicated a strong preference for small group, in-person, hands-on programs as opposed to non-interactive materials. As described by one participant, “if it’s a brochure you’re just going to toss it over there and you’re not going to read it. This way everyone can provide their point of view, and then you get to learn things you didn’t know” (S2P4). Managers echoed the desire for in-person program activities, with demonstrations, saying, “so it’s visual...and they pay more attention. And a lot of times I will get them involved and I’ll ask them questions or this and that” (M4). Several participants stated that they would like a group intervention to encourage support, with ten or fewer agreed upon as an ideal size. Also, many participants agreed that a daycare would facilitate their participation in the interventions.
Concerning the timing of programs, participants were conflicted between weekdays or the weekend. Many in the focus groups suggested that non-work-related interventions could take place outside of the workplace, such as a community center, private home, church, or restaurant. This preference stemmed from stress associated with the workplace, “it’s stressful at work after being there working so then, we don’t want anymore” (S1P3). However, one group unanimously agreed that it would be better to have a program at work after their shift was over, and for there to be incentives such as food. One manager thought that a program would be best implemented in 15-minute chunks each day during the morning meeting. Another manager suggested a program during work hours to increase participation.
Management support was viewed as a critical yet potential challenge to intervention delivery. Participants in different focus groups either expressed that they felt supported by their managers or felt that management did not care about their health and would not authorize an intervention. Some feared that their managers would not support a program. In contrast, most of the managers expressed support and enthusiasm for a health promotion program: “I would love [for] somebody [to] come in and show them how to turn their body right and how to bend right ‘cause a lot of people don’t know how to do that” (M2).
Discussion
This study identifies perceived intervention needs among HRCs and managers. These findings address a unique gap in the literature as one of few endeavors to incorporate accounts from both workers and managers. A grassroot, participatory action approach where interventions stem from the individuals’ expressed needs is more likely to have buy-in, be accepted, adapted, and sustained long-term [21].
Adams and colleagues’ recent review identified only eight interventions targeting the health of hotel workers [24]. They noted that many of these studies lacked rigor and failed to reach statistical significance. However, they highlighted the clinical relevance of these programs in promoting the health and wellbeing of this worker group. Previous interventions among hotel workers have focused on stress reduction [17], cancer prevention [15, 19], healthcare access [18], cardiovascular health [20], injury prevention [13, 14], and weight management [16]. Of these few interventions, only one took into account the workers’ expressed needs [18]. Our findings support the recent work by Zhang and colleagues which combined findings from their literature review and participant interviews to propose nutrition, smoking cessation, stress reduction, and exercise programs [25]. Participants from our study echoed the interventions highlighted by Zhang et al, and expressed additional needs such as increased pay, motivation and improved workload all of which can affect health outcomes. That workers reported lack of chemical and biological hazard safety training was especially troubling given the high exposure this worker group faces.
Interestingly, while there was significant overlap, there were discrepancies between the managers and employees’ perceived needs (see Fig. 1). Such differences should be taken into consideration as they may drive program design and implementation. For example, given that both managers and employees identified smoking, nutrition, and ergonomic training as needs, these programs may be more easily adapted. The difference in the managers and workers’ expressed needs may be due to their job positions and experiences. For instance, the employees highlighted the need for better pay, which was also supported by the managers. However, for their own personal financial needs, the managers noted their desire to learn how to save and invest money.

Expressed intervention needs.
The SEM framework emphasizes the importance of multi-layered facets to fully grasp the magnitude of the phenomenon. Participants in this study highlighted several intervention needs that pervade multiple systems (Fig. 2). Individual level: Interventions such as exercise, smoking cessation, and healthy eating can be addressed at the individual level. In addition, importance of intrapersonal relationships was highlighted. Thus, interventions aimed at promoting supervisor/manager and worker relationship can be leveraged to not only facilitate trust, but to also empower workers and facilitate managerial support in worker health promotion. Organizational level: Workload, strategic scheduling, training, appreciation and positive feedback can be addressed at the organizational/systems level. Policy level: Participants highlights the clear need for policies that address issues such as living wages, improvement of work conditions.
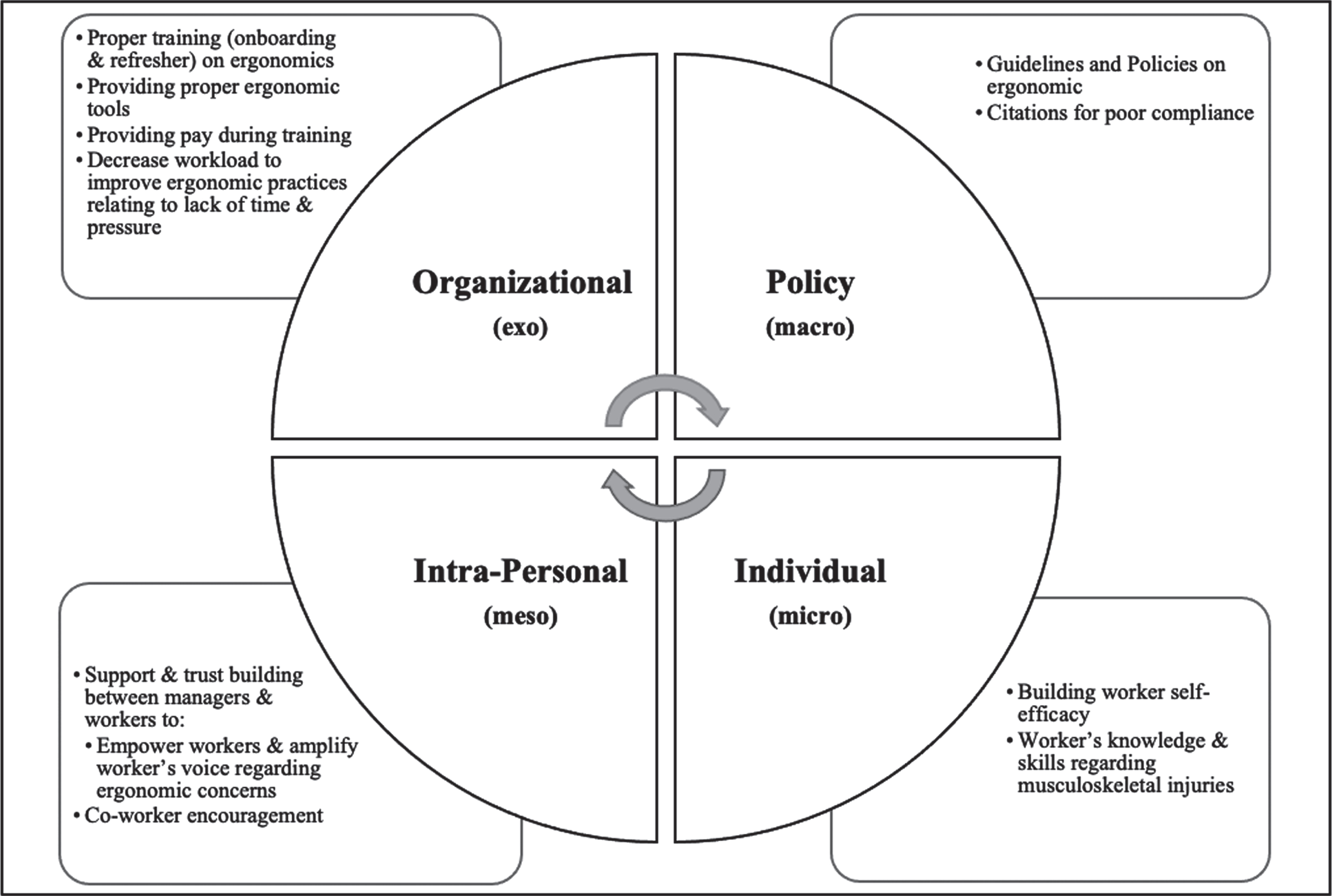
HRC’s and managers’ expressed needs informing future intervention: An example of an integrated approach to remediate musculoskeletal injuries/ergonomic exposure.
Based on the proposed intervention delivery modes, both workplace and community settings should be evaluated in future work. Overall, managers were highly supportive of a program to promote hotel workers’ health, and they proposed that programs take place during the workday. Many room cleaners did not propose this as a feasible option, likely either because they did not perceive their hours and assignments as modifiable, or because they did not believe they had manager support. Given these different viewpoints depending on role, it will be essential to include all key stakeholders (e.g. room cleaners, managers, and others) in both the development and implementation of future interventions.
Given the complexity of the workers’ exposures and needs, complex interventions are likely necessary [26, 27]. These interventions are more likely to succeed if they are tailored while having some basic standard components and are theoretically driven [28]. Theoretical models should guide these efforts, such as the job demand-control-support model, which operates within three dimensions, the demands placed on employees, their decision-making latitude or control, and the workplace social support offered to them. Target mechanisms of change could include employee knowledge, skills, and attitudes regarding health- or work-related content. Future studies are needed to explore needs at the higher organizational level inclusive of inputs from general managers and/or human resources as well as policy level (e.g. current labor law, immigration law, OSHA worker rights and protections) to guide integrated and comprehensive interventions.
This study had a small sample size. Consequently, the findings may not be generalizable to other worker groups. However, this sample size allowed us to reach saturation which is acceptable for qualitative studies. Also, only six managers participated in the study and in contrast to the workers they were interviewed individually. Future studies are needed to incorporate more input from management. Another limitation is that we did not collect information about participants’ age, education level, and marital status. Further studies are needed to highlight whether and how needs vary based on these demographic factors. Notwithstanding these limitations, this work contributes to the push to shift from exploratory to translational research [29]. This push aims for tangible impacts on the health and wellbeing of vulnerable workers. This current study is a step toward this as it identifies action-based needs and lays the foundation toward the implementation of effective and sustainable interventions.
Conclusions
This is one of the first studies to engage HRCs and hotel managers in formulating interventions that match their needs. Much of the current literature on interventions for this population has neglected to involve workers in the design or development process [24]. This study addresses this gap by highlighting unmet needs expressed by HRCs. Despite some discrepancies in worker versus manager identified needs, approach and perceived organizational support, there were some overlapping components that can be leveraged to maximize worker and organizational level outcomes.
Conflict of interest
The authors declare no conflicts of interest.
Funding
This project was supported by the University of Michigan Institute for Research on Women & Gender (IRWG).