
Abstract
BACKGROUND:
Minimally invasive surgery (MIS) has many advantages for patients, however, it places surgeons at risk for Work-related musculoskeletal disorders (WMSD). Recently, the importance of prevention of such injuries and improvement of the ergonomics of the operating room is increasing.
OBJECTIVES:
To assess the prevalence of WMSD among minimally invasive surgeons in Israel, discuss the contributing factors and the overall awareness for ergonomic training. In addition, a review of the literature on the topic was conducted.
METHODS:
An online questionnaire was sent to the members of the Israeli Society of Endoscopic Surgery. The results were analyzed and summarized. For literature review, PubMed was used to search for English-language publications related to the issue.
RESULTS:
Of 83 respondents, the majority (77%) have considerable experience in MIS (more than 10 years). The prevalence of WMSD was 12% before beginning the practice of laparoscopy compared to 78% after 15–20 years of practice. Injury sites included back pain, neck and upper extremity (shoulder pain, tennis elbow and carpal tunnel syndrome) in 41%, 25% and 34% respectively. More than two thirds of responders unaware of possible ergonomic solutions and didn’t consider adopting any appropriate preventive measures.
CONCLUSIONS:
The incidence of WMSD among MIS surgeons is high and underestimated. There is a desperate need to prevent such morbidity among surgeons by increasing awareness and providing the means to improve their work environment. Surgeons should adhere to ergonomic recommendations for positioning of monitors, table height, posture, foot pedal placement and laparoscopic devices use.
Introduction
Work-related musculoskeletal disorders (WMSD) among surgeons and specifically among minimally invasive surgeons are underestimated and more prevalent than the common thinking. Traditionally, generations of surgeons were trained and educated to ignore and to accept physical difficulties and injuries as an integral part of their surgical practice. Normally, WMSD were brought to medical attention only in later stages when they affected their ability to conduct routine work.
Only in recent years the awareness to ergonomics in surgery started to gain momentum and comprehended as an important factor of our surgical practice in order to reduce fatigue and lower future risks of developing WMSD [1–6].
The term “ergonomics” is the process of designing or arranging workplaces, products and systems so that they fit the people who use them, while its aim is to improve workspaces and environments to minimize risk of injury or harm [1]. Today, ergonomics is an essential factor in many fields, such as office jobs, hi-tech industry, and even transportation. However, the application of ergonomics and ergonomic training programs in the field of surgery is still limited [1–3].
Problems with ergonomics in the field of minimally invasive surgery began to arise in the 1990 s when reports of injuries related to laparoscopic instruments began to emerge [4]. At the same time, the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) dedicated a task force for ergonomics in the field. Since then, research on improving the ergonomics of laparoscopic instruments began to dictate the design of the modern laparoscopic instruments [5, 6]. While the instrumentation became more ergonomic, the operating room itself failed to evolve, and remains far from being an ergonomic friendly environment [7, 8].
This study presents the results of a survey concerning the prevalence of WMSD among minimally invasive surgeons in Israel, discusses the contributing factors and the overall awareness for ergonomic training. In addition, a review of the literature on this underestimated issue was conducted.
Methods
An online questionnaire (Table 1) was sent to the members of the Israeli Society of Endoscopic Surgery by the Israeli Medical Association mailing list. The questionnaire was accessible between January 1st, 2019 and February 28th, 2019. The questionnaire included 12 questions on laparoscopic practice and related injuries. Completed questionnaires were sent back and compiled for later analysis.
Online questionnaire
Online questionnaire
For literature review, PubMed was used to search for English-language publications including the keywords: “work related musculoskeletal injuries/disease”, “occupational disease”, “ergonomics”, “Minimally Invasive Surgery”, “laparoscopy”, “surgeons’’, and “surgery”.
There were 83 respondents to the questionnaire. Results of the questionnaire are summarized in Table 2. The majority of responders have considerable experience in minimally invasive surgery (MIS): 59% had 15–20 years of experience in MIS, 18% had 10–15 years of experience and 23% had 5–10 years of experience. Of all the responders, 39% practice MIS in more than 80% of their procedures.
Questionnaire results
Questionnaire results
The prevalence of musculoskeletal disease was 12% before beginning the practice of laparoscopy compared to 78% after 15–20 years of practice (Fig. 1), it is important to note that this is based on the recall of past symptoms at the time of the survey and not based on follow up. The injury sites included back pain, neck and upper extremity (shoulder pain, tennis elbow and carpal tunnel syndrome) in 41, 25 and 34 percent respectively (Fig. 2). Approximately half of responders didn’t use orthopedic shoes.

Prevalence of WMSD before and after MIS practice n = 83.
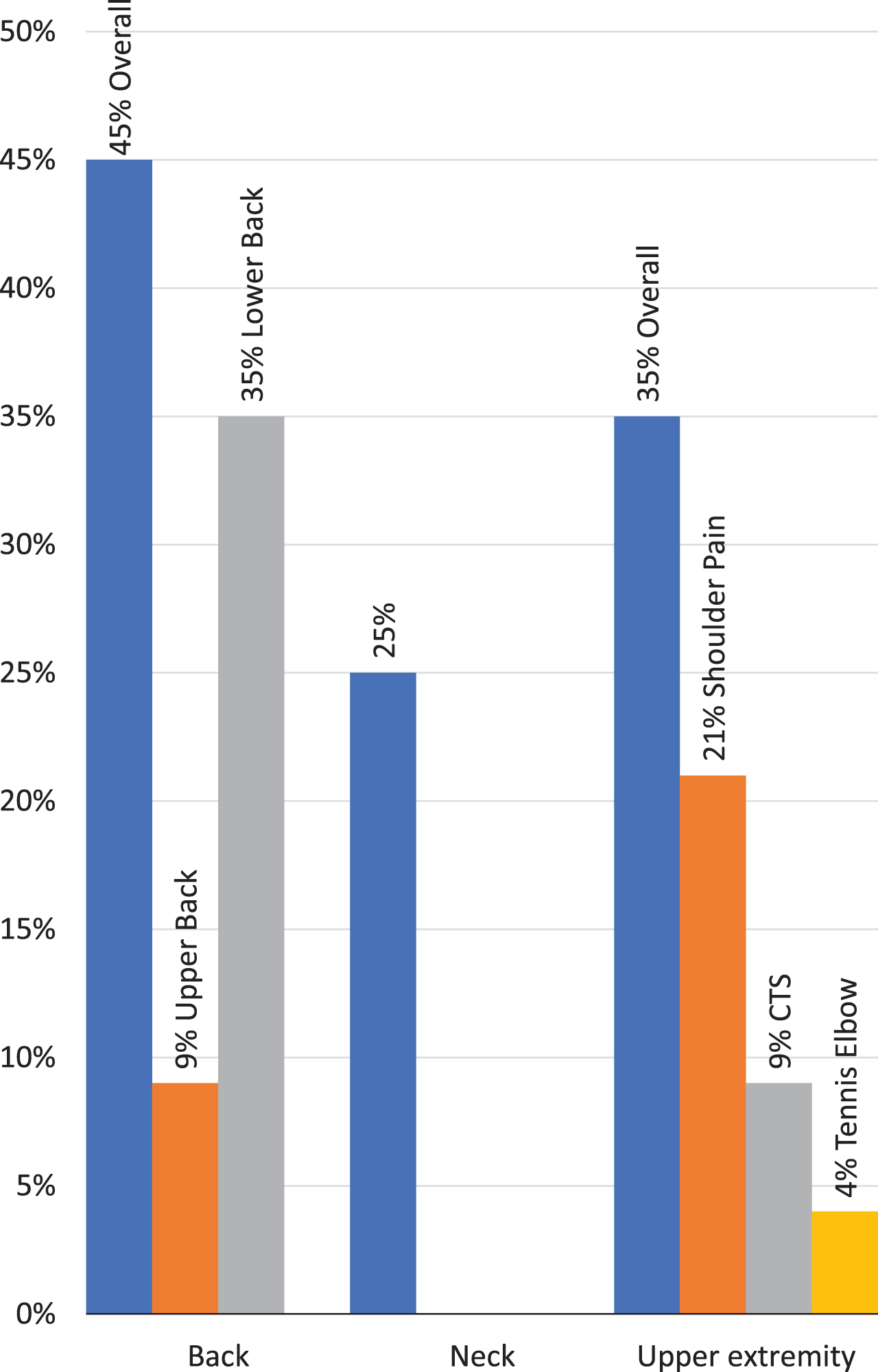
Reported WMSD sites (CTS- Carpal Tunnel Syndrome).
Among those who reported having WMSD, only one third have diagnosed injuries and only 21% were treated accordingly. Despite the high prevalence of work-related injuries, most of the responders (69%) didn’t consider the adoption of ergonomic changes in the operating room in order to tackle WMSD and 70% were not aware or informed about the existence of ergonomic solutions.
When asked about the ergonomic disadvantages in the operating room, 52% reported monitor mal-adjustments and 36% complain of the position and posture during the operation. Interestingly, only 27% of responders believed that robotic surgery is a solution for ergonomic challenges of MIS, while 50% only considered it as a possible solution. The rest (23%) denied it as an option with this regard.
Most of the research on the prevalence of musculoskeletal injuries among surgeons is subjective, based on questionnaires sent to endoscopic surgical society members [1–6], with low compliance, thereby resulting in low power results. Some studies using EMGs have demonstrated high levels of muscle activity and fatigue levels of surgeons during various surgical procedures. These studies support the premise of WMSD as demonstrated by high levels of muscle strain and stress during laparoscopic surgery [9].
According to this survey, there is a high incidence of WMSD among laparoscopic surgeons, reaching as high as 78% after 15–20 years of experience, most commonly lower back, neck and upper extremity injuries. where most of them are non-diagnosed and untreated. Similar results were reported by Gutierrez-Diez et al. who found the prevalence of WMSD among surgeons of MIS in different specialties to be as high as 90%, with higher rates in more experience [10].
Intuitively, and in spite of the logical correlation between age and WMSD, it seems to be rather difficult to isolate experience and age in the association with WMSD because the two are natural confounders due to their correlation. However, in the wider ergonomic literature outside the operating room, such as Collins et al. [11], age had a poor association with WMSD symptoms.
Another interesting finding in the current study, is that the majority of surgeons were not aware of ergonomic solutions available.
A handful of systematic reviews regarding the prevalence of WMSD among minimally invasive surgeons have been published. In their review in 2017, Alleblas et al. found the prevalence of WMSD in the literature to be in the variable range of 20–100%, with an average of 74% [12]. However, they found a high level of inconsistency across study results, with an I2 value of 98.3%. A more recent review and meta-analysis by Epstein et al. found that the 12-month prevalence estimate for work related WMSD of physicians was comparable to workers in high-risk labor-intensive occupations, such as construction workers [13]. In a survey among members of the European Association for Endoscopic Surgery (EAES) [14], 87% of the respondents reported pain in the last 7 working days, while 62% reported significant pain. When asked about pain by operating modality, severe pain was reported in 22% of laparoscopic cases, as compared to 16% of open. Despite the high prevalence and the effect on their quality of life, only 26% of surgeons reported work-related pain to their employers. Of all the respondents, only 22% sought professional medical help, this is similar to the results of this study, where only 21% received treatment. In their study, 48% needed physiotherapy, 10% surgery, 12% support devices and 7% needed cervical traction. Moreover, 16% of those who sought medical help considered leaving the surgical profession due to the considerable pain [14].
In relation to the high incidence of back pain in this study, underdiagnosed discopathies should be considered as a possible etiology. An injury which could have a considerable deleterious effect both economically and professionally [13]. A study among members of the British Society for Gynecological Endoscopy found a prevalence of 15% of vertebral herniation secondary to laparoscopic work. Of those, 32% needed invasive treatment including micro-discectomy, facet joint injections or nerve root interventions [15]. They also found that the prevalence of injuries was directly associated with the weekly workload, years of practice and complexity of the surgical procedures performed.
There are several presumed causes for the physical strain during laparoscopic surgery, such as table and monitor mal-adjustment, limited ergonomics of the instruments and non-optimal placement of trocars. Furthermore, there is increased strain on the neck and back due to static positioning of the head and trunk with less weight shifting [16–18]. This corresponds with the results of this survey, where 52% reported monitor maladjustment as the main cause of strain and 36% complained about the position and posture during the operation. Even the platforms used in the operating room are designed for open surgery and are often not large enough to accommodate electrosurgical foot controls, consequently requiring the surgeons to bare all their weight on one foot [19]. Finally, EMG studies demonstrated increased deltoid, forearm and thenar muscle effort in laparoscopic knot tying and grasping compared to open [6].
Based on studies using EMG, video and posture analysis during laparoscopic surgery, several ergonomic recommendations were published [20–24]. These recommendations included postural changes such as: shoulder abduction should be less than 30 degrees and elbows should be held between 90-and 120-degree flexion [21] (Fig. 3), additionally, incorrect shoulder and elbow posture may result in excessive wrist flexion and as a result a risk for carpal tunnel injury, the neck should be flexed at an angle between 10 and 30 degrees, and excessive twisting and axial rotation should be avoided [23]. Proper operating table height (66–77 cm from the floor) and foot pedal alignment will allow the surgeon to make these postural changes [24]. Additionally, recommendations about monitor positioning, which should be between 10 and 30 degrees below and in front of the eye level of the main surgeon [22]. The implementation of micro-breaks to stretch, and prevention through conditioning and strengthening activities for core strength and stabilization such as Pilates and yoga in addition to focused muscle strengthening should also be considered [24]. The development of new novel innovations in the fields of posture support, arm support, robotic and non-robotic intuitive articulating instruments are aimed to further improve ergonomics of the surgeon within the operating room [25, 26].
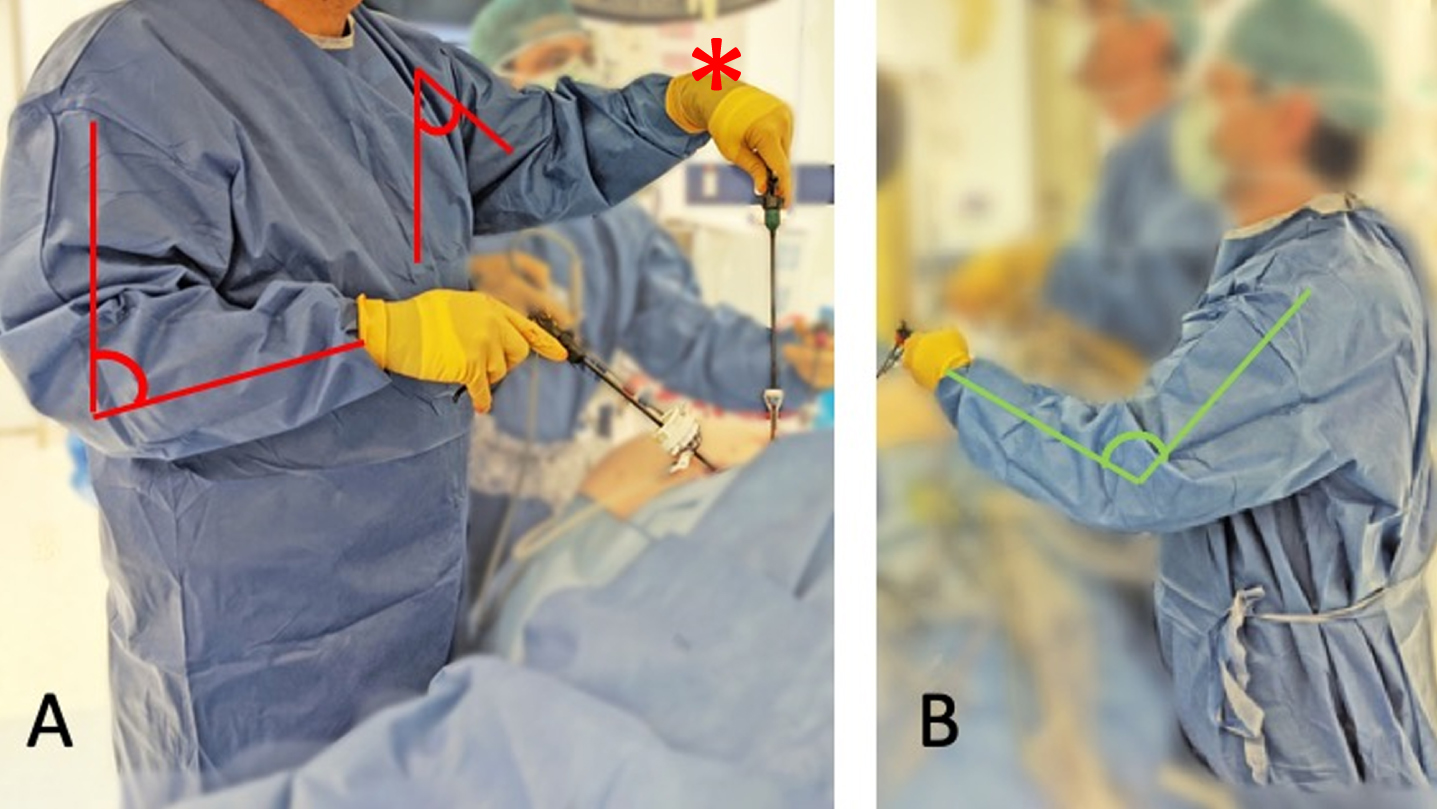
A-Incorrect shoulder abduction, elbow and wrist flexion, B- Correct elbow and wrist extension.
This study was limited by sample size, as with other studies based on questionnaires, which also lack the higher power results, therefore future studies may consider including more surgical specialties which perform laparoscopic surgery such as urology, and obstetrics and gynecology, in order to build a larger powered study. The literature review demonstrated a lack of studies in the areas of ergonomics for female surgeons, as well as those surgeons who operate on patients with higher BMI, which may further strain the surgeon. These areas necessitate further studies as well as potentially the development of devices for those with smaller hands or for larger patients.
It is interesting to note that while robotic surgery is thought to be less physically stressful on surgeons, studies comparing robotic to laparoscopic surgery, have demonstrated no superiority from one approach to the other. Rather different fatigue locations –laparoscopic in the forearm and robotic in the neck and shoulders [27]. Indeed, most of our responders (73%) were skeptic to the notion that robotic surgery would be a useful solution for the ergonomic problems imposed by laparoscopic surgery.
The incidence of WMSD among MIS surgeons is high and underestimated. Unfortunately, the awareness to the issue is still limited and most surgeons are not aware that the operating room has ergonomic limitations that need to be addressed.
There is desperate need to prevent such morbidity among surgeons by increasing awareness and providing the means to improve their work environment. Surgeons should take the time to determine the best positioning of monitors, table height, foot pedal placement and laparoscopic devices used that best suit them. Additionally, preventative measures should be stressed, including the implementation of conditioning and strengthening exercises, as well as incorporating micro-breaks into daily operating routines. Adhering to ergonomic guidelines and recommendations may decrease the risk for injuries and improve the surgeons’ quality of life and productivity.
Footnotes
Acknowledgments
The authors thank the members of The Israeli Society for Endoscopic Surgery.
Conflict of interest
None to report.