
Abstract
OBJECTIVE:
The aim of this study was to investigate the prevalence of metabolic syndrome (MS) among dentists in Riyadh, Saudi Arabia. The study also explored the causes of occupational stress among the participating dentists.
MATERIALS & METHODS:
The participants included a conveniently selected sample of dentists (N = 126; Males = 65; Females = 61). The participants’ anthropometric measurements/blood sample analysis were carried out and they completed a self-administered questionnaire. Data analysis included demographics, gender/age wise comparison using SPSS (p < 0.05). For the diagnosis of MS, updated criteria of the National Cholesterol Education Program was applied.
RESULTS:
Participants diagnosed with MS were 13 (10.3%), Males = 11(8.7%) and Females = 2(1.5%). Physical activity of 6 (15.8%) with MS was only 0–2 hours/week. 9 (14.5%) participants with MS declared positive family history for MS. The average systolic (117.55±11.33) and diastolic blood pressure (71.9±9.34) of the participants was found to be normal with no gender wise statistical difference. No gender wise statistical differences (p > 0.05) were observed for cholesterol, triglycerides and HDL. However, significant difference (p = 0.00) was found for the fasting glucose level (Males = 5.69±1.49; Females = 4.94±0.42). Overall mean scoring (3.00±1.11) for the stress showed that the participants fall into the average/moderate level of stress category (Males = 3.16±1.02; Females = 2.83±1.08). Almost two third (68.26%) of the participant’s responded that they were under some kind of stress.
CONCLUSIONS:
MS was found to be less frequent among the dentists working in the city of Riyadh. Overall, the dentists were under moderate level of occupational stress, with male dentists being more prone to work related stress.
Introduction
Metabolic syndrome (MS) is known as clustering of at least three of five abnormalities of metabolic origin [1–4]. The National Cholesterol Education Program’s Adult Treatment Panel III (ATP III) identified these abnormalities as central obesity, elevated triglyceride (TG) level, reduced high density lipoprotein (HDL)-cholesterol level, elevated blood pressure, and elevated fasting glucose concentration [4]. Metabolic syndrome deserves more clinical attention as it’s known as a multiplex risk factor for cardiovascular disease (CVD). It has been related to increased risk of sudden death and stroke [5, 6]. It is also associated with an increase in heart rate, left ventricular hypertrophy, arterial stiffness and atrial fibrillation [7–10].
MS has been first described with different definitions and diagnostic criteria which justifies the conflicting results regarding its prevalence. However, it has been considered as an important global health issue with prevalence of 20–25% worldwide [11, 12]. It has been increasing in both developed and developing countries. Increase in MS is mainly related to the rapid growth of type-2 diabetes and cardiovascular disease in the recent decades [1, 13].
The etiology for MS is not completely identified but it is indirectly affected by genetic predisposition such as age, pro-inflammation, dementia, hormonal changes and inactivity [14, 15]. Genetic is considered as an important risk factor in MS, and different ethnic groups have shown different prevalence rates [16]. Studies showed about 70% heritability demonstrated involving HDL genes [17]. However, there are other risk factors for MS include smoking, sedentary lifestyle, old age, postmenopausal status, obesity, high carbohydrate and soft drink intake, and low income [15, 18]. Moreover, insulin resistance and central obesity are the most important factors in its prevalence [12, 18–20]. Metabolic syndrome has also been associated and found to be a product of occupational stress [21]. Workers with chronic stress are associated with double the risk of developing MS [22].
Dentistry has been considered as potentially stressful occupation [23]. About 60% of dentists revealed being tense, depressed or nervy because of occupational stress [24]. Several causes of stress have been given such as administrative difficulties, attempts to establish a practice and dealing with different patients [25]. Treating a lot of patients, management of nervous patients and collecting payments have been identified as other sources of occupational stress [26]. Presence or lack of association between occupational stress and metabolic syndrome have been studied among different occupations and revealed different results. However, less is known about relation between metabolic syndrome and occupational stress among dentists [27, 28].
Dentists appear to be subjected to an even higher risk of adverse health effects, including MS due to their lesser physical activity [29]. Research studies have reported the dentists to be physically inactive and prone to obesity, due to the physical nature of the work and long working/clinical hours continuing from morning hospital work to the evening clinics [30]. The sedentary lifestyles of dentists as well as the occupational stress makes the dentists at a greater risk for developing chronic diseases leading to MS [31, 32]. Scarce information in the literature is found regarding the prevalence of MS among the dentists. Thus, the aim of this study was to investigate the prevalence of metabolic syndrome among the dentists in Riyadh, KSA. In addition, the study also explored the causes of occupational stress among the participating dentists. The findings of the study will help in identifying and solving the work-related health/stress issues and complications associated with it.
Materials and methods
This cross-sectional study was conducted at University Dental Hospital (UDH), King Saud University (KSU), Riyadh between October 2019 and February 2020. Before initiation of the study an ethical clearance was obtained from institutional review board (#H-01-R-002) of King Saud University Medical City.
The participants included a conveniently selected sample of dentists working at the UDH. The required information was planned to be collected by recording the anthropometric measurements of the participants, blood sample analysis and completion of a self-administered questionnaire by the participants. An invitation was sent to all the dentists working in the different departments of the hospital via emails, social media accounts and posters invitation placed all around the dental hospital. Dentists or faculty who were retiring, on leave, or on holiday were excluded. Using power analysis (G*Power 3.1.9.7, Germany) [33] with alpha < 0.05 and power of 95 % the minimum sample size calculated was supposed to be 100.
For the data collection all the willing participants were supposed to arrive at the data collection stations early morning with minimum 8 to 10 hours fasting. After formal written consent the participants first completed a stress-related questionnaire. The first part of the questionnaire was used for recording the demographic information and occupational characteristics of the participants. The questionnaire included questions from the short version (QPSNordic 34+) of the General Nordic Questionnaire for Psychosocial Factors at Work (QPSNordic). The questionnaire has been modified by excluding few questions which are not related to the sample. The version used in this study included 17 questions of five options, ranging from 1 to 5. According to the questionnaire, scores 1 to 2.5 were considered as a low level of stress (first level), scores 2.5 to 3.5 were considered as the average level (second level), and scores 3.5 to 5 were considered as a high level of stress (third level). Nordic questionnaire has been used in similar studies with success [34, 35] and was chosen to examine the level of job stress, because it included various variables such as job demands, role expectations, social interactions, control at work, and leadership.
After completion of the questionnaire, the participants’ blood samples were collected at collection unit at the UDH for the analysis of fasting blood glucose levels, serum triglycerides and high-density lipoprotein (HDL)-cholesterol. The samples were collected in fasting condition, and 15 cc blood was taken from each subject.
After the blood sample collection, the participants underwent examination/anthropometric measurements for metabolic risk factors. The measurements included recording of the blood pressure (BP) by a qualified medical nurse using a mercuric sphygmomanometer device (YuWell, Jiangsu, China) for measuring systolic and diastolic pressure. Each person was requested to sit for 10 minutes in a waiting area, then the BP been taken. The BP was taken twice in 5 minutes’ intervals and the mean of the two measurements was considered the actual value.
Anthropometric measurements, included height in centimeters (cms), weight in kilograms (kg) and waist in (inch). Height and weight for each participant were measured with a scale (Seca 769, Hamburg, Germany) while the scapulars were normal and no footwear. For the waist measurement, the person was requested to stand with normal exhalation and the measurement taken using a meter tape between twelve ribs and iliac crest. All measurements were taken by one qualified nurse to avoid any variability with the measurements. The body mass index (BMI) was then calculated by dividing weight in kilograms by the square of height in meters (kg/m2) for the participants.
Data analysis
All the recorded data was tabulated and analyzed using SPSS (Version 22, Ilinois, Chicago, USA) for the demographic details and statistical analysis using chi square test (p < 0.05). For the diagnosis of MS, updated criteria of the National Cholesterol Education Program [4] was applied. This has been validated in a large number of studies [36, 37] and the MS is identified according to these criteria when three or more of the following conditions are present in the same subject: waist > 102 cm (40 inch) in men and > 88 cm (35 inch) in women, fasting glucose ≥6.1 mmol/L (110 mg/dL), serum triglycerides > 1.695 mmol/L (150 mg/dl), HDL-cholesterol < 1.036 mmol/L (40 mg/dl) in men and < 1.295 mmol/L (50 mg/dl) in women, blood pressure ≥130 (systolic) or ≥85 (diastolic) mmHg or in treatment for hypertension.
Results
The demographic details of the participating dentists is presented in Table 1. The total number of participants were 126. The number of males and females participants were 65 (51.6%) and 61 (48.4%), respectively. The participants diagnosed with MS were 13 (10.3%), out of which 11 (8.7%) were males and only 2 (1.5%) were females. The physical activity of 6 (15.8%) out of the 13 participants with MS was only 0–2 hours per week. For the participants with MS, 9 (14.5%) declared positive family history for MS. These findings showed that less physical activity and family history are the contributing factors towards the progression of MS. Smoking was not a causative factor for the MS, however, the increase in age and working hours were the evident factors in the participants with MS (Table 1).
Demographics and prevalence of metabolic syndrome stratified by different variables (N = 126)
Demographics and prevalence of metabolic syndrome stratified by different variables (N = 126)
*P was significant at P < 0.05.
Table 2 describes the anthropometrics, biochemistry data and regression analysis of the study participants stratified by gender and age. The average systolic (117.55±11.33) and diastolic blood pressure (71.9±9.34) of the participants was found to be normal with no gender wise statistical difference, however, an increase in blood pressure was noted for the aged participants. No gender wise statistical differences (p > 0.05) were observed for cholesterol, triglycerides and HDL. However, significant difference (0.00) was found for the fasting glucose level, which was high for males (5.69±1.49) as compared to females (4.94±0.42). The fasting blood glucose also tended to increase in the aged participants. Even though the BMI was found to be in normal range for both the males and females (BMI = 18.5–24.9), interestingly females (21.52±8.21) showed high BMI values as compared to males (19.38±12.22).
Anthropometrics, biochemistry data and regression analysis of the study participants stratified by gender and age (N = 126)
*P was significant at P < 0.05.
Response of the participants to the questions related to professional stress are presented in Table 3. The overall mean scoring (3.00±1.11) for the stress showed that the participants fall into the average/moderate level of stress category, with males (3.16±1.02) being more stressed as compared to the females (2.83±1.08), though the difference was statistically non-significant (p = 0.061). Females tended to be under more stress because of the workload (Q2 = 3.48±1.04). According to the male participants the inequalities in how older and younger employees are treated at the workplace was very high (Q7 = 3.74±1.24). Both the genders agreed that they possess sufficient skills for performing their tasks (Q4), can manage the amount of workload assigned to them (Q9), there is no conflict among the coworkers (Q5) and that their management is interested in health and well-being of them (Q17).
Response of the participants to the questions related to professional stress on a *Likert scale (N = 126)
*5-point Likert scale used with the questions 1–7 ranging from never [1] to always [5] while questions 8–17 are ranging from always [1] to never [5].
Participants’ self-reported response to the questions regarding their job satisfaction are presented in Fig. 1. Almost half (40.47%) of the participants agreed that major satisfaction in their lives come from their job and they like to be absorbed in their jobs for most of the time (51.58%).

Participants response to the questions regarding job satisfaction.
Participant’s opinion regarding the generalized question about stress showed that majority (68.26%) of them were under some kind of stress these days (Fig 2).
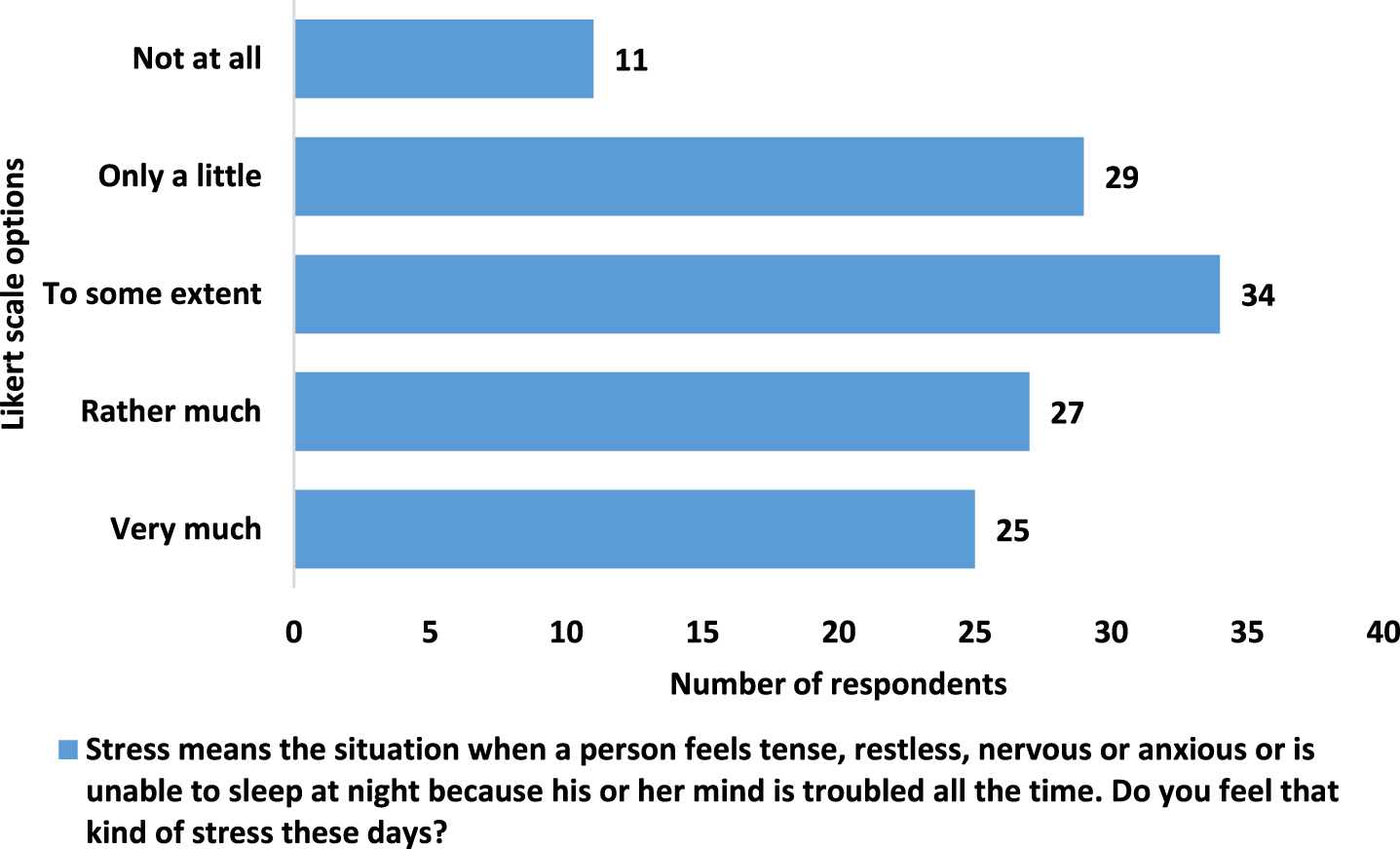
Participants response to question regarding stress.
This study provides an analysis of health status with particular attention and emphasis on prevalence of metabolic syndrome among the dentists from different age groups and gender, working in UDH-KSU Riyadh. We also were able to endorse a link between dentists and metabolic syndrome and in particular with their working hours/areas and level of stress as effecting components. The stress related questions were designed based on some previous studies [33, 34] and keeping in view the objectives of the present study. Although prevalence of MS in various work professions have been reported in the literature, similar studies among the dentists are scarce. Due to the physical nature of the work, physical inactivity, sedentary lifestyles, stressful work in a closed room and long working/clinical hours, the dentists are prone to suffer from stress, MS and its related complications [36]. The results of this study will help in identifying the possible reasons for these work-related complications and may contribute in finding the solutions in order to prevent these complications.
Over the past decade, and in the recent past as well, an amassing evidence emerges suggesting that the healthcare professionals’ work and services may be associated with an increased risk of developing illnesses and hence been explored [37–40]. The enormousness of this connotation, however, seems to be intensely affected by the inadequacy of current literature’s exploration and least efforts to determine its grade of severity.
The strength of our discoveries lies in having establish an association between dentists’ work satisfaction, level of stress and the metabolic syndrome for which we used both a clinical approach like data gathering through anthropometrics and biochemistry and survey measures with a questionnaire.
Present study established that the increase in age and working hours were the obvious reasons in the participants for having MS. Aging is well-thought-out as a biological progression considered by a progressive weakening in physiological functions and metabolic courses that drive to morbidity and mortality. Aging, the development of insulin resistance and cardiovascular disease seem to be accelerated in the metabolic syndrome [41, 42]. Majority of our participants from both genders and various age group have shown a low prevalence of MS, however, those who found to suffer from MS were on the higher side of the age group (i.e., 51–60).
Health professionals in general and the dentists in particular have to undergo and comply with the heavy and fast paced and sometimes ironic needs of caring the patients. This makes dentists prone to hassle and the long working hours become sources of stress. Dentists are more disposed to professional burnout, anxiety, and depression [43].
The present cross-sectional study of dentists (male and female) also observed whether there has been any stress and depression associated/related to the profession. Our study found that there was a mild to moderate level (as overall mean) of stress related to the participants’ profession. Similar finding also reported that the long working hours are significantly related to stress [44]. However, such finding could be interpreted in the context of relationship between MS and depression also as a cross-sectional study of middle-aged male exhibited a positive association between depression and MS. Our finding showed the female participants to be having more stress as compared to the males. In 2016, Kulkarni et al. reported that the females commonly encountered professional burnout resulting in stress [42].
In our study the participants (both male and the female) agreed that they possess sufficient skills for performing their tasks, this finding could be an outcome of working experience in an well reputed organization as UDH-KSU, where the selection criteria of the faculty and staff is professionally robust. Another potential reason could be the experience of the participants in the term of their working years as the participants have a sufficient range (i.e. minimum 1–10 and maximum 10–20 years) of working experience. Similar findings were reported in another study which reported significant relationships between management, age and work experience [45].
Conducting study among the limited number of dentists in one city is a limitation and the authors are aware of it and recommends applying the findings of the current study with caution. Though the present study provided some information regarding the work related physical complications and stress complications of the dentists working in a city, there is a need for conducting further detailed studies to be carried out across the country and all over the globe to highlight and address this important subject of work related complications. The factors affecting the physical and psychological health of the dentists needs to be explored/investigated further and addressed to make the dentists job free of work related complications.
Conclusions
Although metabolic syndrome is less frequent among the dentists working in the city of Riyadh, frequent medical exams and investigations should be implemented to rule out the possibilities of emerging/newly developed cases and complications of the existing established ones. Overall, the dentists were under moderate level of work related stress, with male dentists being more prone to work related stress as compared to female dentists. Future research on larger scale focusing on the working conditions and lifestyles are recommended in this group.
Footnotes
Acknowledgments
The authors are thankful to the participating dentists for their participation and time. The authors also are thankful to Mr. Nasr Maflehi for helping in the statistical analysis. The research project was approved by the institutional review board of King Saud University Medical City (Reg # H-01-R-002). The study was funded and supported by College of Dentistry Research Center (CDRC) and Deanship of Scientific Research at King Saud University.
Conflict of interest
The authors declare no conflict of interest for this research project.