
Abstract
BACKGROUND:
Case management interventions have shown to be effective to prevent musculoskeletal pain and disability, but a single definition has not been achieved, nor an agreed profile for case managers.
OBJECTIVE:
To describe the elements that define case management and case managers tasks for return-to-work of workers with musculoskeletal disorders (MSDs).
METHODS:
A comprehensive computerized search of articles published in English until February 16, 2021 was carried out in several bibliographic databases. Grey literature was obtained through a search of 13 key websites. A peer-review screening of titles and abstracts was carried out. Full text in-depth analysis of the selected articles was performed for data extraction and synthesis of results.
RESULTS:
We identified 2,422 documents. After full-text screening 31 documents were included for analysis. These were mostly European and North American and had an experimental design. Fifteen documents were published between 2010 to 2021 and of these 7 studies were published from 2015. Fifteen elements were identified being the commonest “return-to-work programme” (44.4%) and “multidisciplinary assessment/interdisciplinary intervention” (44.4%). Of 18 tasks found, the most frequent was “establishing goals and planning return-to-work rehabilitation” (57.7%). Eighteen referral services were identified.
CONCLUSIONS:
Despite there were several elements frequently reported, some elements with scientific evidence of their importance to deal with MSDs (e.g. early return-to-work) were almost not mentioned. This study proposes key points for the description of case management and case managers tasks.
Introduction
Musculoskeletal disorders (MSDs) are the second highest contributor to disability worldwide, being low back pain the leading cause of disability globally [1, 2]. Furthermore, musculoskeletal conditions account for the highest proportion of lost productivity in the workplace [1]. Its impact is significant in terms of health, wellbeing and economic costs in the European workforce, and it is a crucial determinant for a healthy aging [3]. In fact, MSDs are the commonest work-related health problems in Europe, representing half of the total sickness absence of at least three days of duration, 60%of permanent disabilities and generating an estimated cost of 0.5 to 2%of Gross Domestic Product [3, 4]. Consequently, one of the greatest health challenges is to reduce sickness absence due to MSDs and to support the return-to-work [5].
Interventions to prevent and manage MSDs need a biopsychosocial approach instead of the traditional biomedical approach due to their multi-causal origin [6]. The Biopsychosocial model was introduced by Engel (1977) and recognizes that the level of pain and disability are a result of interactions between physical, psychological, social and environmental factors that determine how the person will manage his/her own health [7]. Specifically, interventions for MSDs work-related must consider the biomechanical factors caused by workers’ movements (posture, duration, frequency, intensity, vibration, etc.), psychosocial factors (adaptative behaviour, psychological dema-nds, stress, decision-making freedom, social support, etc.), and organizational constraints (contradicting orders, dependence, procedures, etc.) [8]. Several multidisciplinary rehabilitation and case management programmes have been shown to be effective to reduce MSDs, symptoms (such as pain) and disability, and to improve work continuity and return-to-work [9–11].
Case management programmes trace back to the 1800s, but the exact starting point is difficult to determine. In the United States, the first reports date around 1860 and their objective was to respond to the lack of coordination in the humanitarian and health services provided to immigrants and those most in need [12]. Since then, case management programmes have been widely implemented in a great diversity of domains, such as the education sector, social work, mental health settings, social welfare systems, insurance and compensation systems and wide variety of healthcare settings [13]. In 2009 the Case Management Society UK (CMSUK) defined case management as: “a collaborative process that values, plans, implements, coordinates, monitors and evaluates the options and services required to meet individual health, assistance, educational and employment needs, using the communication and available resources to promote quality and cost-effective results” [14].
Although during the last decades different authors and organizations (e.g. CMSUK) have proposed their own updated and extended descriptions for case management, a single description of case management for return-to-work interventions has not been achieved, nor an agreed profile for case managers. This lack of an agreed definition hinders the understanding, comparability and quality analysis. It is then essential to provide evidence-based descriptions of case management and to clarify the tasks of the case managers to promote a scientifically sound practice.
The objective of this study was to describe the elements that define case management and the tasks of the case management role for return-to-work of workers with MSD through a literature review.
Methods
The protocol of this study is available elsewhere [15]. This scoping review is based on the methodology described by Arksey and O’Malley [16] and the recommendations of Levac et al. and Colquhoun et al. [17, 18]. The steps to develop a scoping review can be grouped into five stages encompassing the whole process: (I) identification of the research question, (II) identification of relevant studies, (III) selection of the studies for the analysis, (IV) charting the data and (V) collecting, summarizing and reporting the results.
Identification of the research question
The main research question was defined as “How is case management described in the literature in the return-to-work for workers with MSD?” The sub-questions were: 1) what are the elements that describe case management in the literature in the return-to-work for workers with MSD?; 2) what are the tasks of the case managers?; and 3) what are referral services offered within these case management programmes?
Identification of relevant studies
This scoping study used scientific and grey literature. The scientific literature search was carried out in the bibliographic databases PubMed, Web of Science, Scopus, Cochrane Library, IBECS, EMBASE and LILACS, published in English until February 16, 2021. No limits on publication dates were considered. Different types of documents and study designs were included: research papers, reviews, protocols and commentaries/editorials. The search strategy was initially formulated for PubMed and was adapted for its use in the other databases. The descriptors and qualifiers of the specific thesaurus of PubMed database were used for greater precision. PubMed search strategy was transcribed on seven steps and studies were selected from the last search. Scopus database allowed synthesizing the search in a single transcript (Table 1).
PubMed and Scopus search strategies
PubMed and Scopus search strategies
Grey literature included “literature produced at all levels of government, academics, business, industry in print, and electronic formats, but which is not controlled by commercial publishers” [19]. The grey literature key websites searches were conducted until February 16, 2021. The organizational websites were: World Health Organization; Occupational Health and Safety Agency European Union (OSHA-EU); United Kingdom (UK) –Case Management Society of the United Kingdom (CMSUK) and British Society of Rehabilitation Medicine; United States of America (USA) –Occupational Safety and Health Administration (OSHA), Case Management Society of America, Agency for Healthcare Research and Quality, and American Case Management Association; and Australia: Rehabilitation Counselling Association of Australasia, Heads of Workers’ Compensation Authorities, Australian Society of Rehabilitation Counsellors (ASORC), Case Management Society of Australia and New Zealand, and Sira NSW.
All obtained titles and abstracts were analysed independently by three researchers (MS, JMG, and FP) using the Covidence systematic review software (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia).
The inclusion criteria were developed according to the PPC format for scoping reviews, where participants (P) were combined with concept (C) and context (C) [20]. Based on this classification, the inclusion criteria were: (P) workers (active workers/unemployed workers) with MSDs (or mixed populations i.e. MSDs and another pathology); (C) studies that described a case management intervention or the tasks of the case manager role; and (C) case management interventions focused on return-to-work, whether it was analysed in isolation or in conjunction with another result (e.g. return-to-work and keeping the employees at work). Exclusion criteria were MSDs referred to acute trauma pathologies, surgical interventions in its acute phase, rheumatic pathologies; and military personnel since they are a sample with unique features that differ from most occupations.
Articles that met the inclusion criteria were read in full text by three independent researchers (MS, JMG and FP) to make the final decision of inclusion in the full review. At full-text screening, articles were excluded when both reviewers considered they did not fulfil the inclusion criteria. A senior researcher (CS) resolved any discrepancies. We identified the articles that were part of the same study. Of these, we selected only the article that included the description of case management or the tasks of the case manager role more broadly (i.e. the methodological paper). Therefore, there were three scenarios: 1) articles describing case management; 2) articles describing the tasks of the case manager role; and 3) articles that include the two descriptions above.
Charting the data
The relevant data from each selected article were extracted by three independent researchers (MS, JMG and FP), and were summarized using a data extraction form. Subsequently, a cross examination of the retrieved information to guarantee its accuracy and completeness was carried out. The data extraction sheet collected the descriptions of case management, the role or tasks of case managers and the referral services. Moreover, the variables of year of publication, country, study design and targeted population were also collected.
Collating, summarizing and reporting\\ the results
A summary of all relevant information was per-formed to answer the research questions. Results were collated, summarized and thematically re-ported, identifying the common elements in the case management descriptions, the tasks of case managers and the referral services.
Results
Our searches identified 2,402 documents through database searches and 20 from grey literature. After exclusion of duplicates, 2,318 citations were screened for eligibility, of which 2,047 were excluded because they did not meet the inclusion criteria, and the full text was not available for two articles. We screened the full text of the remaining 269 articles. After full-text screening, 226 articles were excluded for not defining case management or the tasks of case managers, and 12 articles were identified as being part of the same study of other articles and were also excluded. These 238 excluded references are reported in Supplementary Table 1. Finally, 31 documents (29 scientific literature and two grey literature) were included in the review and were thus analysed (Fig. 1).
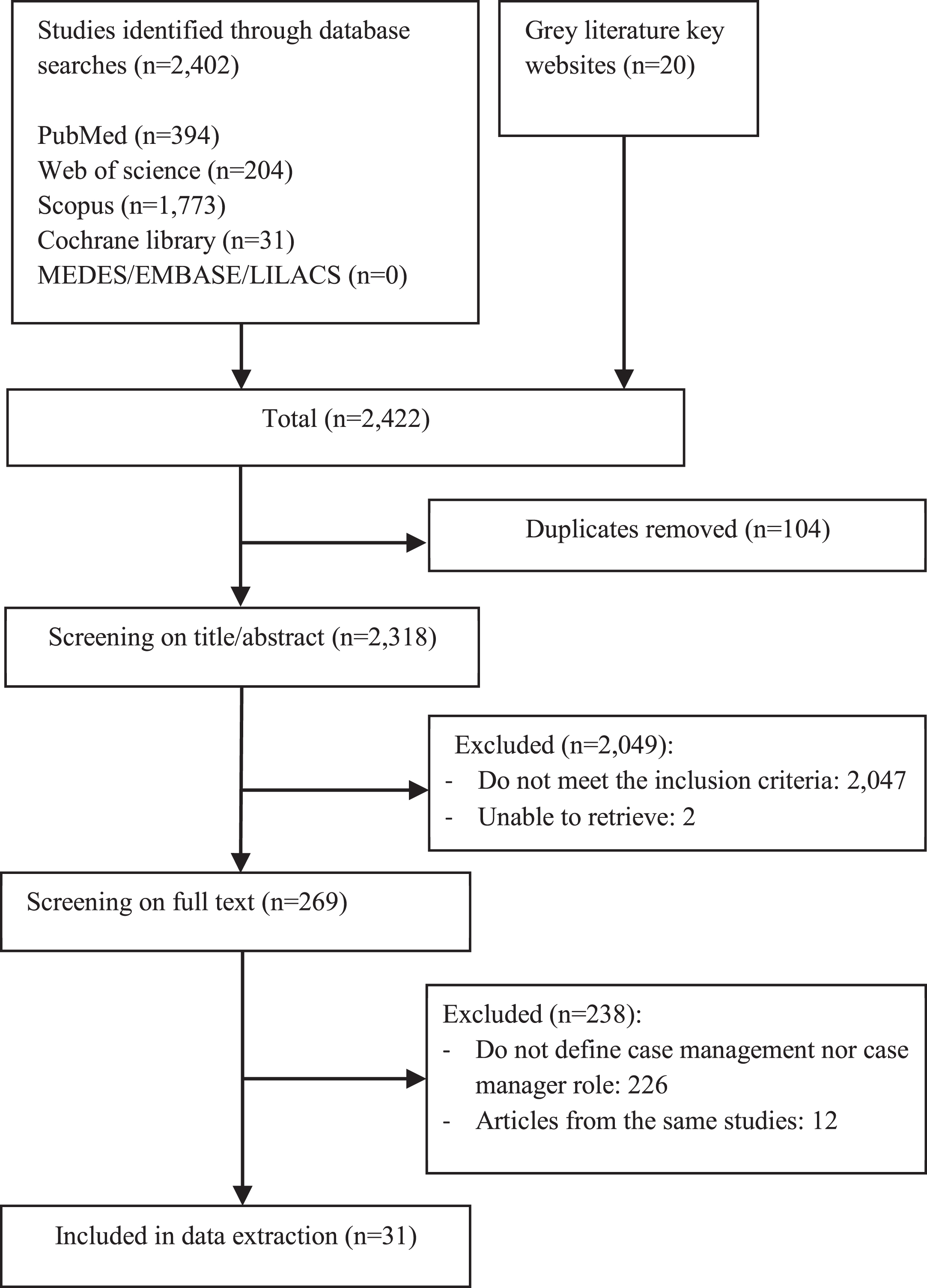
Flowchart of the search strategy and study selection.
Table 2 shows the characteristics of the included documents. Of the 29 documents, 18 included a case management description [21–26, 51], 26 explained the tasks of case managers [21–32, 48–51], and 29 included referral services [21–34, 45–51]. Full definitions are provided in Supplementary Table 2. Sixteen studies were published before 2010 and 15 were published between 2010 to 2021, of these, seven studies were published from 2015. The majority were European (n = 16), mainly from the United Kingdom and Denmark, also the Netherlands, Switzerland, Sweden, Finland and Spain; and North America (n = 10) mainly from the United States, and also from Canada. Three studies were from Australia and two others from Asia (China and Malaysia). Most studies (n = 17) had an experimental or quasi-experimental design, three were observational (cohort or cross-sectional), four were reviews (three narrative and one systematic), three were editorials, there was two case-studies, two reports, and one article with mixed design. The target population were workers on sickness absence in 19 studies, and active workers were included as well in 12 articles.
Characteristics of studies and summary of case management identified elements, the tasks of the case managers role and referral services
Doc: type of document; SA: sickness absence; RTW: return-to-work; RCT: randomized controlled trial; CBT: Cognitive-Behavioural Therapy. N/R: Not reported.
Eighteen studies reported a description of case management and a total of 15 elements were identified in these descriptions: (1) return-to-work programme and (2) multidisciplinary assessment or interdisciplinary intervention were both found in 8 articles (44.4%). Coordination (3) was mentioned in 7 articles (38.9%). The elements (4) addressing multiple factors (medical, work environment, claims), (5) development of a plan, and (6) individual approach were reported in 5 documents (27.8%). Four documents included (7) interaction with providers and stakeholders, and (8) vocational intervention (22.2%). The (9) identification of barriers, and (10) support, coaching and empowerment were identified in three articles (16.7%). Two articles reported (11) early return-to-work, and (12) solving problems/mediating (11.1%). One article reported (13) keeping employees at work, (14) motivational interviews, and (15) work disability screening (5.6%) (Table 3).
Elements identified in case management descriptions reported in 18 studies
Elements identified in case management descriptions reported in 18 studies
RTW: return-to-work.
Table 4 shows the 18 tasks of case managers identified in 26 documents. These tasks are listed as follows, from highest to lowest number of mentions: (1) establishing goals and planning return-to-work rehabilitation (n = 15, 57.7%); (2) working with community health professionals (n = 12, 46.2%); (3) supervising or coordinating the RTW process (n = 11, 42,3%); (4) communicating/interacting with managers and human resources and (5) offering/referring the employee services/adaptations or therapeutic (n = 10, 38.5%); (6) to follow-up, assess, support and guidance (n = 8, 30.8%); (7) interviewing and advising/evaluating (n = 7, 26.9%); (8) ensuring the earliest RTW/ accelerating the RTW process (n = 6, 23.1%); (9) monitoring RTW (collecting data, presenting a report) (n = 4, 15.4%); (10) addressing risk factors and barriers that hinder the ability to RTW and (11) identifying worker’s needs/expectations and disability perceptions (n = 3, 11.5%); (12) instructing patients stay active and avoiding static-work, (13) considering if sick-listed person should be granted a disability benefit and (14) remaining patients at work (n = 2, 7.7%); and (15) assessing if the sick-listed employee is able to RTW, (16) making a workplace visit, (17) providing education the worker and (18) providing education to the employer (n = 1, 3.8%).
Tasks of case manager reported in 26 articles
Tasks of case manager reported in 26 articles
RTW: return-to-work.
We identified 18 different services offered as part of case management programmes in 29 articles (Table 5). Rehabilitation and mental health were the commonest services offered to workers, found in 17 (58.6%) and 16 (55.2%) documents respectively. Occupational physician was mentioned in 51.7%and general practitioner in 37.9%of the documents. Vocational rehabilitation and work modification were reported in 31.0%studies. Six studies included progressive return-to-work and cognitive behavioural therapy (20.7%), and five studies included the referral services of ergonomics and physical exercise/training/work hardening (17.2%). The 13.8%included nurse or occupational nurse, occupational therapy and social worker. Counselling and chiropractic were reported in 10.3%of documents, coaching in 6.9%and health promotion and medication or surgery in 3.4%.
Referral services offered in the case management of the 29 articles
Referral services offered in the case management of the 29 articles
RTW: return-to-work.
We systematically reviewed the literature to identify the described elements of case management, the tasks of case managers and the referral services offered, for the return-to-work of workers with MSDs. Through 29 scientific papers and 2 reports from grey literature, we identified 15 elements that describe case management, 18 tasks of the case manager role, and 18 referral services.
Eighteen studies reported a description of case management but only four used or adapted previous definitions. Li Tsang et al. [26] and Russo et al. [29] used the definition proposed by Maki [52] which includes five elements: return-to-work programme, multidisciplinary assessment, development of a plan, coordination and vocational independency. Moreover Beaumont et al. [21] published an editorial in support of the description proposed by Nicholson, who stated that case management is to “case-manage people who are on sick leave, working with community health professionals to ensure the earliest return of functional capacity and return-to-work” [53]. Lastly, Bishop et al. [22] used the description from Stapelfeldt et al. “goal-oriented approach to keeping employees at work and facilitating an early return-to-work” [54].
The described elements in this scoping review were mainly return-to-work programme, interdisciplinary intervention, coordination, addressing multiple factors and development of a plan. Development of a plan should include a detail of the measures that the employee will undertake, modifications to work equipment, working hours and review dates [55]. The element of identification of barriers can be especially important in complex cases for return-to-work in workers with MSDs [56] and can be separated into three basic categories: biomedical, ergonomic and psychosocial [57]. Moreover, an early intervention addressing psychosocial obstacles to recovery can be effective for reducing absence due to MSDs [56]. However, only two articles included early return-to-work, and only one mentioned keeping employees at work.
As mentioned previously, the Case Management Society UK proposed the following definition of case management: “a collaborative process that values, plans, implements, coordinates, monitors and evaluates the options and services required to meet individual health, assistance, educational and employment needs, using the communication and available resources to promote quality and cost-effective results” [14]. Although this definition is not focused on MSDs, it includes the use of resources and cost-effectivity terms, which are important issues to consider.
The case manager is the person on charge of carrying out the case management, fulfilling a range of tasks, and always looking for a balance between the return-to-work achievement and the available resources. The main tasks of case managers reported by the literature were the establishment of goals and the rehabilitation plan for return-to-work, which requires an agreement with the worker to get a successful return-to-work [55]. Secondly, to work with community health professionals, the supervision or coordination of the return-to-work process and the communication or interaction with managers and human resources, were tasks that clearly align with the elements of the descriptions mentioned before, along with ensuring the earliest possible return-to-work, helping to keep workers at work, addressing risk factors and barriers that limit the capacity to return-to-work, and monitoring return-to-work (collecting basic data or presenting a report). In addition, we found 10 other characteristics focused on the case manager-worker relationship which usually fit in the biopsychosocial approach, such as instructing patients to stay active and avoid static-work, considering whether a sick-listed person should be granted a disability benefit, identifying expectations and perceptions about disability, making workplace visits, providing education to the worker and the employer, assessing whether the sick-listed employee is able to return-to-work, interviewing, advising, evaluating, carrying out follow-up assessments, providing support and offering guidance or referring the employees to services, and facilitating workplace adaptations, which are crucial for successful implementation [56].
Finally, the case manager will need to identify the appropriate referral services for each worker (i.e. long-term sickness absence worker may require more support and specific services). Eighteen referral services were identified. Some of these services are usually included in the structure of health systems, such as the general practitioner, the occupational physician or nurse, rehabilitation or surgical procedures. In addition, for most services described in this scoping review there is wide evidence of their effectiveness in interventions for return-to-work such as cognitive-behavioural therapy [58], vocational rehabilitation [58] and progressive return-to-work and job modifications [59]. However, a few other described interventions with limited evidence for the return-to-work process, such as general mental health [60] and physical exercise [58, 61]. Hence, offered services in a case management programme should address the physical, psychological, social and setting areas, and be based on the available scientific evidence.
Strengths and limitations
This scoping review was an attempt for the first time to our knowledge to classify and evaluate the elements of the description of case management, the tasks of case managers and the referral services for the return-to-work of workers with MSDs through the scientific and the grey available literature. Also, we did not limit the type of documents, nor the year of publication.
Our review has some limitations. First, we could not find the full text of two documents and we cannot rule out the possibility of having lost other relevant information. Moreover, there may be a country bias since most articles came from the United States and the United Kingdom because of language restrictions, and therefore, these countries and their contexts may be over-represented.
Key points
Based on the information on case management elements, tasks, and services analysed in this scoping review, we present several key points for the content of case management and the tasks of case managers. We have incorporated the commonest elements of case management along with the new ones identified in this review that are less common but necessary for the management of musculoskeletal disorders: (1) case management for the return-to-work of workers with musculoskeletal disorders must be a tailored and multidisciplinary intervention to keep the working-age population at work or to promote an early return-to-work, framed in the biopsychosocial model; (2) case management needs to be tailored to the requirements of the specific workers’ compensation or other return-to-work framework in place in each particular country; (3) the role of case managers covers a wide range of tasks from the follow-up/controlling the return-to-work process to a biopsychosocial perspective; (4) generally, case managers’ tasks include the assessment, coordination, organization, implementation, referral to services, monitoring and evaluating the rehabilitation plan, involving multiple factors; (5) to incorporate a biopsychosocial approach, the tasks of case managers should also include the guidance, empowerment and education of both workers and employers, the identification of physical, psychological and social barriers and facilitators, and the interaction with the stakeholders involved in the health, work, psychosocial or administrative settings; (6) the case manager needs to identify the appropriate referral services for each worker, and usually complex cases will require more services.
Conclusion
This scoping review identified and reported the described elements of case management, the tasks of case managers and the referral services offered, for the return-to-work of workers with MSDs. Despite several elements are frequently reported, some elements with scientific evidence of their importance to deal with MSDs, such as early return-to-work, identifying barriers or keeping employees at work are almost not used. There is a need to establish an agreed definition of case management for MSDs. Finally, this study proposes several key points for the content of case management and tasks of case managers.
Footnotes
Acknowledgments
We want to thank Andrew N March for providing a grammatical revision of the text, and Anna Amat for her collaboration during the first part of this scoping review. The work was supported by the Instituto de Salud Carlos III-FEDER (reference number PI14/01959 and PI17/00779). The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Conflict of interest
The authors report no conflicts of interest.