
Abstract
BACKGROUND:
The current state of research indicates pregnancy-related discrimination as a potential stressor during pregnancy for women at work, which may result in perceptions of occupational stress.
OBJECTIVE:
The aim of this study was to examine women’s perceptions of pregnancy-related stressors at work, problem- and emotion-focused coping strategies as well as attributed consequences for mental, physical and social dimensions.
METHODS:
The survey was completed online with a cross-sectional study design. Inclusion criteria for the study participation were being currently pregnant and engaged in paid work (regardless of full-time or part-time work). Women were recruited via social media and with the support of pro familia.
RESULTS:
Results indicate that 79 (53.4%, n = 148) participating women experienced pregnancy-related stressors at work. The most relevant kinds of stressors were intrapersonal stressors and interpersonal stressors related to employers or colleagues. The most prevalent coping strategy was to seek social support or advice from gynaecologists. Attributed physical consequences were exhaustion, fatigue and sleeping disorders. Mental health consequences were named in terms of feeling emotionally upset and having fears related to the baby’s health.
CONCLUSIONS:
Family-friendly support policies need to be further developed and topics like pregnancy-related stressors need to be addressed in an occupational context. Especially the perspective and knowledge of employers on the topic needs to be strengthened, e.g., to ensure an ongoing communication between employers, HR and employees during pregnancy. Further research is needed which provides representative data, analyses employer’s experiences and their attitudes in managing pregnancies as well as consequences for women when returning to work.
List of abbreviations
Comparative Analysis of Social Mobility in Industrial Nations
Human resources
large for gestational age
absolute number
Preterm birth
small for gestational age
Research question
Background
In general, having children is no longer a reason for parents to drop out of the workforce as shown by several indicators. In 2019, the overall employment rate for women aged 15-64 was 72.8%. In comparison, the rate of employed mothers was 74.7% representing an almost two percentage points higher rate [1]. Furthermore, also in 2019, two-thirds of all employed mothers with at least one child under 18 worked part-time (66.2%, compared to 6.4% for men). However, the dual burden of childcare and a job in the current COVID-19 pandemic plays an additional role for 6 million women in Germany [1].
Annually, about 350.000 women remain employed during pregnancy in Germany. However, only half of the pregnancies (about 170.000) are reported to local authorities. This may indicate a lack of consideration of pregnancies in an occupational context, especially in small and medium-sized businesses [2]. Moreover, expecting women report that their pregnancy is often not explicitly considered by employers or colleagues, which may result in conflicts, mobbing and attempts to dismiss. The experiences women gain at work during pregnancy have an intrinsic effect on further career decisions, which are often a result of past support and appreciation [3]. The way in which women are perceived in society and in the workplace may change with the transition to motherhood regarding social identity, stigmatization and possible discrimination [4]. King and Botsford [5] illustrate that both individual as well as interpersonal experiences play an important role especially in the context of (delaying) pregnancy disclosure atwork [5].
The current state of research concerning stressors during pregnancy at work indicates pregnancy-related discrimination as the most relevant stressor [6–8].Taken as a whole, discrimination refers to actions, decision-making processes or policies that affect individuals or groups negatively [9]. Discrimination due to pregnancy includes, for example, not employing women due to their pregnancy, treating them disadvantageously or dismissing pregnant employees [9]. Adams et al. [8] differentiated negative experiences during and after pregnancy at work into the following categories: feeling forced to leave the job, financial aspects, negative experiences on opportunities, job status or security, health and welfare impacts, negative comments on pregnancy, declined flexible working requests and other negative experiences [8].
The prevalence of discrimination at work related to pregnancy is widely spread. Cross-sectional research describes between 30 and 49% of surveyed mothers experiencing discrimination during or after their pregnancy (as well as during parental leave or when returning to work) [6, 7]. Results from the UK indicate that 77% of expecting women report negative (discriminatory) experiences at work during pregnancy [8]. Moreover, a possible stressor during pregnancy could be attributed to intrapersonal factors, in which several expectations to fulfil a role may interfere, for example, the role of a parent and the worker’s role [10]. Adams et al. [11] examine views of pregnant and employed women from an employers’ perspective including difficulties in organising a substitution during maternity leave (18%), managing part-time or flexible working during or after pregnancy (17%) or uncertainty about whether women on maternity leave will return to work (26%) [11]. All in all, mothers who experience discrimination at work are also less likely to engage in the workforce, to be attached to the workplace or to return to their jobs after pregnancy. 32% of those who reported discrimination looked for other jobs orresigned [7].
Research from Ireland and Australia indicates different coping strategies are applied by pregnant employees. When dealing with stressors encountered at work, they contacted managers, supervisors or human resource (HR) departments, trade unions or solicitors, made formal complaints, looked for a new job or legal advice, resigned, discussed it with friends, family or colleagues, or took no action [6, 7]. Results from Ireland indicate that the large number of 72% of pregnant women who gain experience of discrimination do nothing about it, while about one in five women confides in their manager or supervisor [6]. Reported reasons for taking no action include that discrimination is not perceived as severe enough, women are afraid of contacting someone officially or they believe that taking action would not change the situation [7].
As a consequence, about three-quarters of pregnant women experience negative effects on their mental health, in combination with loosing self-confidence and motivation at work [7]. Moreover, the most common reported consequences for health of unfair treatment as a stressor during pregnancy at work are specific illness or injury, premature or low birthweight, nausea or faintness, bleeding, hospitalization, high or low blood pressure, leg, back or foot problems, fatigue or exhaustion, as well as stress and anxiety [6]. Nearly half of the participating women (48%) experience stress and anxiety at work during pregnancy, which is the most prevalent adverse outcome. Fatigue, tiredness or exhaustion is reported by 24% [6]. Additionally, job strain during pregnancy is evaluated as a predictor of increased depressive symptoms (β= 1.63, 95% CI = 0.29; 3.07). Indirect effects of discrimination and job strain on depression by accumulating perceived stress are stated as well, though effects were lessprecise [12].
Recent research underlines the relevance of these results for concerned children: high levels of occupational physical activities are significantly linked to small-for-gestational age (SGA, birth weight < 10th centile for their gestational age) and positively related to preterm-birth (PTB, deliveries before gestation week 37). No clear results are found for psychosocial stressors at work referring to SGA or PTB [13]. Results from Larsen et al. [14] indicate no clear association between job strain and PTB or SGA referring to a large prospective birth cohort from Denmark. However, high levels of job strain was linked with significantly lower odds of being born large for gestational age (LGA, birth weight 90th percentile or above for their gestational age) [14]. Taking the health status of 7-year-old children into account additional research from Larsen et al. [15] shows that self-reported high strain during pregnancy was associated with a 15% higher chance of developing atopic dermatitis. In addition, an association between active jobs and asthma among 7-year-old children was observed based on Karasek’s Job Strain Model (women were split up into four job strain categories including low strain (low demands, high control), active (high demands, high control), passive (low demands, low control), and high strain (high demands, low control)) [15].
Concerning stressors at work during pregnancy, the topic is still understudied in the German context [16]. In 2018, the German law on maternity protection which dated back to 1952 has been firstly reformed. Employers are obliged to employ expecting or nursing women in a safe way adjusting working conditions including machinery, tools and equipment, to be adequately protected from any risk to health. In the context of risk assessment, which is required by law, employers must take into account special pregnancy-related protection needs [17]. Compared to the results obtained in the UK, Australia and Ireland [6–8], law in Germany differs regarding maternity protection/leave and parental leave. The influence of the perception of pregnancies in the society may vary as well in the analysed countries. Thus, results from other countries are only transferable in a limited way. In addition, the demographic change has noticeable effects in Germany. Every second person in Germany is older than 45 and every fifth person is older than 66 [18]. However, after many years of decline, birth rates rise again since 2012. Reasons for an increase in births by 2016 may include increased immigration and family policies (e.g., introduction of parental allowance and expansion of childcare). The demographic echo could also play a role (effect that baby boomers cyclically cause baby boomers again) [19].
Theoretical framework of the study
To explore stressors for pregnant women in an occupational context, the transactional model of stress [20] is considered as a theoretical framework for the study. The model offers different starting points for the analysis and deduction of intervention possibilities, which can be adapted to target-group specific needs on individual and structural levels. The model aims at compensating imbalances, which are a threat to well-being. The cognitive-transactional process is divided into primary and secondary appraisal, which evaluates whether there is something at risk (primary appraisal) and what coping resources are available (secondary appraisal). When a stimulus is appraised as stressful needing actions to overcome the situation, coping actions become effective [20]. Two coping strategies are identified and described as problem- and emotion-focused approaches (overcoming the situation either by direct actions or by regulating own emotions) [21]. Ongoing work-related stress may result in negative physiological and mental outcomes like hypertension, muscle tension as well as clinicaldepression [22].
Objective
Guided by this framework, the study aims to identify and categorize different pregnancy-related stressors for pregnant women working in Germany. Moreover, women’s coping strategies are analysed (and identified whether they were problem- or emotion-focused). The third aim is to examine attributed consequences of the women’s perceived pregnancy-related stressors to their physical health, mental well-being and social aspects in short-term (Fig. 1).
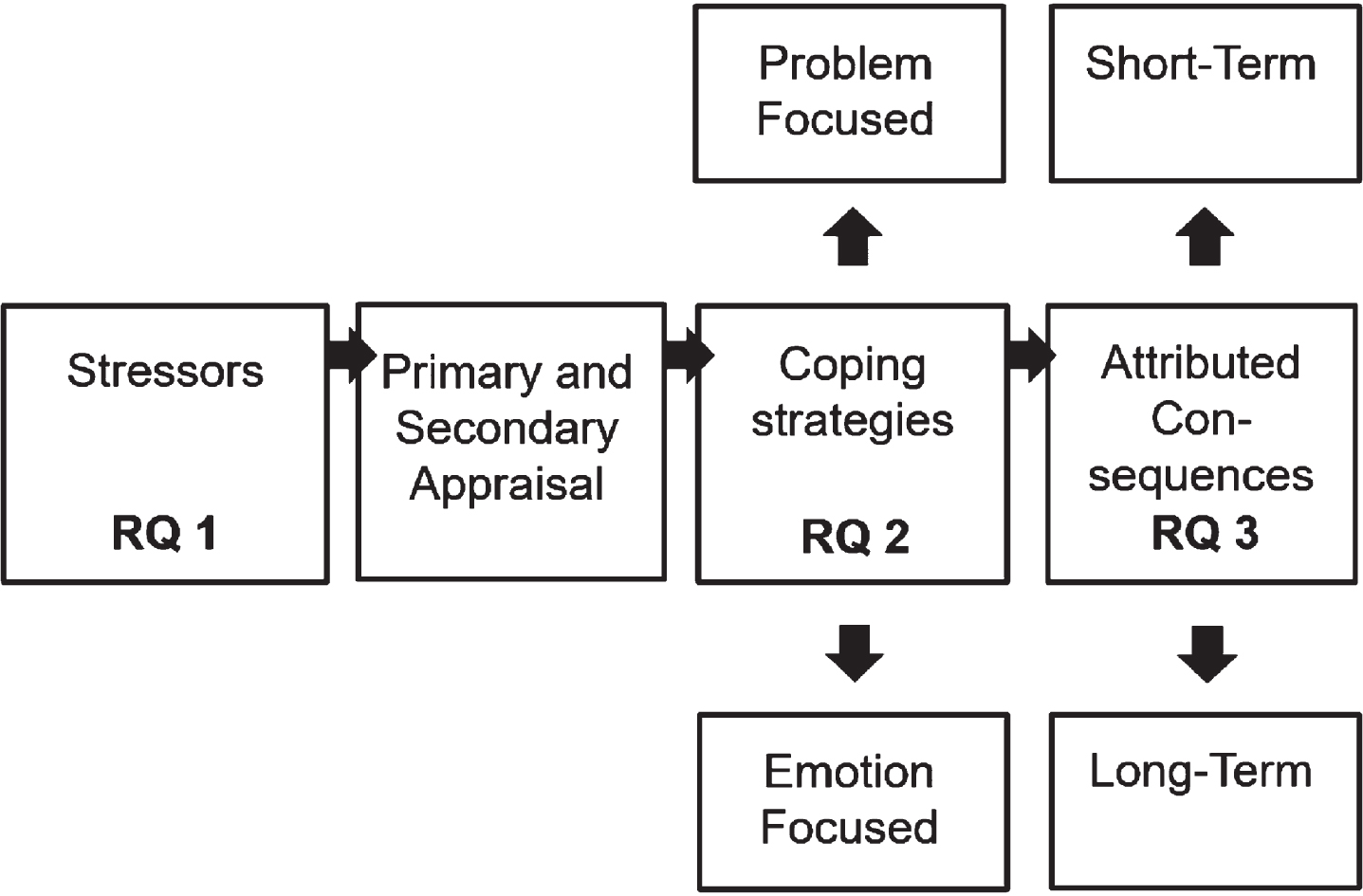
Based on the current state of research and the illustrated framework of the study, the following research questions (RQ) are derived highlighted in Fig. 1: What kind of pregnancy-related stressors are women confronted with during their pregnancy at work? How do women cope with pregnancy-related stressors at work? What are mental, physical and social consequences for women when experiencing pregnancy-related stressors at work?
Study design
This cross-sectional study was designed to provide data on a national level concerning women’s experiences with stressors and conflicting situations at work related to their pregnancy, applied coping strategies as well as associated physical, mental and social consequences. Based on further conducted qualitative research in Germany [24, 25], a quantitative online approach was chosen to examine stressors during pregnancy in employed women.
Recruitment strategy
Expecting women were recruited via two different approaches. On the one hand, online communities addressing pregnancy issues via social media boards were used to spread the study. On the other hand, flyers using QR-Codes and a link to the survey were displayed at the German non-governmental organisation pro familia dealing with pregnancy, sexual and relationship issues, which offers advice on a regular basis.
Inclusion criteria for study participation were being currently pregnant and engaged in paid work (regardless of full-time or part-time work). Women who already gave birth or who were self- or unemployed were excluded from the study. Informed consent to participate in the study was obtained beforehand. At the beginning of the study, participating women were informed about the inclusion criteria, as well as within the flyer. In addition, filter questions relying on self-reports were used, for example, on the week of pregnancy and on the current employment status.
Participants
61.4% of expecting women were between 21 and 29 years old (n = 135). Compared to results of the Federal Statistical Office, the average age of a mother when giving birth to the first child was 31 years old [26]. Based on the CASMIN classification (internationally comparable education classification taking two characteristics into account: general education and vocational education), most of the women had a middle educational level (61%, n = 133) [27]. For about half of the participating pregnant women (n = 118), the current pregnancy was the first. About half of the participants lived in a relationship, but were not married (47.9%, n = 105)(Table 1).
Sociodemographic characteristics
Sociodemographic characteristics
1n=220; 2n=218; 3 - 4n=219. Sample size varies because of missing values.
Table 2 displays that most of the women had open-ended contract designs and full-time jobs (64.2%, n = 106). Moreover, about half of the pregnant women worked between 33 and 40 hours per week (53.9%, n = 89). About one quarter of the women worked in companies with 10 to 49 employees, another quarter was employed in companies with more than 250 employees (27.9%, n = 46 and 26.1%,n = 43).
Workplace characteristics
1,3 - 4n = 165; 2n = 161. Sample size varies because of missing values.
The following sociodemographic and workplace characteristics were assessed in the questionnaire: Sociodemographic characteristics: age, level of education, relationship status and having own children. Workplace characteristics: weekly working hours, job tenure, size of the company and the contract design (full-time or part-time as well as open-ended or limited contract design).
At the beginning, participating women were asked whether they experience any pregnancy-related conflicts at work (“Did you experience any pregnancy-related (open as well as subtle) conflicts at work as a result of your pregnancy?”, binary answer options served as a filter question). Afterwards, different kinds of stressors were assessed including stressors in relation to first-line managers/employers, (future) contract design, (in) adequate working conditions, physical and psychological changes, conflicts with colleagues, financial disadvantages, intrapersonal stressors and other stressors. At the beginning of each question, the respondents were asked whether this type of conflict existed (yes or no) and followed by various examples of the type of conflict (multiple answers were possible). Questions were self-constructed based on previously conducted qualitative research in Germany [24, 25]. Coping strategies of women were examined with self-constructed questions including problem- or emotion-focused strategies with the possibility to report multiple answers (“How did you cope with pregnancy-related stressors at work on an emotional level?”; “Did you take any action in response to pregnancy-related stressors at work?”). Attributed consequences were asked in three self-constructed questions also with the possibility to report multiple answers, firstly related to mental well-being, secondly related to physical health and finally related to private and social aspects (“Was your health negatively affected in a physical, mental or social way by your employment during your pregnancy?”).
Statistical analysis
Quantitative answers were analysed in a descriptive way. The software SPSS (version 24) was used to evaluate the data. Open-ended questions were examined as well which aimed at identifying other kinds of stressors during pregnancy at work. To ensure a systematic and rule-guided analysis, an inductive approach was chosen for building categories [28].
Results
Stressors during pregnancy at work
148 women were asked about any experienced stressors at work due to their pregnancy, which applied to 53.4% (n = 79). This question served as a filter to examine different kinds of pregnancy-related stressors which are displayed in Table 3. The following percentages mainly referred to the sub-group of participants experiencing those kind of stressors. 46.6% (n = 69) did not have any experiences with pregnancy-related stressors.
Different kinds of pregnancy-related stressors at work
Different kinds of pregnancy-related stressors at work
1 - 2 n = 79; 3 - 5 n = 77; 6 - 8 n = 74. Sample size varies because of missing values.
Guided by the transactional model of stress [20], emotion-focused and problem-focused coping strategies of women reporting about pregnancy-related stressors were assessed (Table 4). A frequently reported aspect was to talk to social contacts (partners, family, and friends) (58.9%, n = 43) or retire from the situation (49.3%, n = 36). Problem-focused approaches included seeking help from social contacts like partner or friends (65.3%, n = 47) or talking to the gynaecologist about pregnancy-related problems (62.5%, n = 45). Furthermore, 25 women (34.7 %) contacted their employer regarding their concerns or set boundaries or priorities for themselves (38.9%, n = 28). Only three women report that they did nothing about the situation.
Applied coping strategies
Applied coping strategies
1n = 73; 2n = 72. Sample size varies because of missing values.
69 women (of those experiencing work-related stressors at work) reported negative consequences for mental health attributed to pregnancy-related stressors at work. Most of them express that they felt emotionally upset (73.9%, n = 51) or that they had fears about the baby’s health (66.7%, n = 46). Most prevalent consequences for physical health were exhaustion (65.2%, n = 45), listlessness (52.2%, n = 36), fatigue (50.7%, n = 35), sleeping disorders (50.7%, n = 35), headaches (43.5%, n = 30) and stomach pains (34.8%, n = 24). 15 women (21.7%) reported contractions or bleedings. Concerning social aspects most of the women faced consequences for the relationship with their partner or husband, which was strained by occupational stressors (47%, n = 31) (Table 5).
Attributed consequences of pregnancy-related stressors at work
Attributed consequences of pregnancy-related stressors at work
1 - 2n = 69; 3n = 66. Sample size varies because of missing values.
This study aimed at identifying different kinds of pregnancy-related stressors at work in Germany. Additionally, different emotion- und problem-focused coping strategies and attributed short-term consequences for mental, physical or social dimensions were analysed.
Stressors during pregnancy at work
One of the most important analysed stressor during pregnancy at work refers to negative pregnancy-related comments, which was reported by 63.3% of those who report stressors due to their employer or first-line managers. Cross-sectional results from Ireland indicate that 8.2% of pregnant and employed women complain about unpleasant comments from their employers, managers or colleagues [6]. In a study conducted in Australia, it is observed that negative attitudes related to pregnancies are more prevalent. 28% of the women report negative attitudes from employers or managers and 19% from colleagues [7]. Nearly the same number of pregnant women (about one in five) is highlighted as being affected by negative pregnancy-related comments by results from the UK [8].
Compared to results from Ireland, the nature of pregnancy-related unfair treatment is characterised by most of the women who reported unsuitable work or workloads (11.6%) [6]. In an Australian context, nearly half of the participating expecting women underline discriminatory experiences based on their safety and health during pregnancy, including irregular toilet breaks, high (and inadequate) workloads or transfer issues into a safe work environment [7]. Consistent with findings from this study, women who report stressors related to inadequate working conditions mostly refer to heavy lifting and continuous standing. The high relevance of stressors as a result of inadequate working conditions is also reflected in experiences of legal advice in Germany, which indicates that employers are often uninformed about their duties concerning a risk assessment of working conditions in Germany [29].
In addition, international research concerning pregnancy-related unfair treatment is described as having an impact on further career steps or (future) contract designs. For example, results from the Australian Human Rights Commission illustrate that 46% of pregnant and employed women face a negative influence on promotion or training opportunities [7]. This kind of stressor is also described in an Irish context and for the UK, including half of the mothers who report negative impacts on further career planning [6, 8]. Based on the conducted study, stressors related to (future) contract design, included to be threatened with dismissal, impacts on negotiations on future contract design, fail to gain a promotion or even dismissal. This could be attributed to the fact that there is an association between discriminatory behaviour not only concerning employer’s perception of working and expecting women in general but also to their obligations like adjusting working conditions [30].
However, this survey adds a new critical issue: results indicate that expecting women often deal with stressors on an intrapersonal level (78.4%), which referred to fears concerning the baby’s health, feelings of punishment for being pregnant or feelings of guilt towards colleagues about being pregnant. The occurrence of intrapersonal stressors may be explained by the opposing responsibilities of many women fulfilling their occupational role and their (upcoming) role as a working parent [10]. Further research is needed on the gestation week and its effects on work-related stress.
Applied coping strategies
To cope with pregnancy-related stressors, highpercentages of women retired from the situation or tried to think positive in an emotion-focused way. Moreover, the sample was characterised by women who seek help in a problem-focused way, like talking to their partner or friends. However, social support is known to have a positive, buffering impact in the context of occupational stress and consequences for health, which has been examined in several studies in the past [31, 32]. Other coping strategies are linked to the gynaecologist’s advice or are based on priorities or boundaries for themselves. The key role of the gynaecologist can be explained by the low-threshold character concerning both health-related issues and occupational questions for example concerning prohibitions of employment, because of the individual health status.
In comparison to international findings from Australia or Ireland [6], an elevated amount of women try to change something about the situation in the present study. In Ireland, at least 72% report not to do anything to change their situation at work. Only one in five state to talk to their manager or supervisor [6]. In the Australian context, 91% does not make a formal complaint after a conflicting situation related to their pregnancy at work [7]. Women classify experienced stressors as “not serious enough”, “it was too hard, stressful or embarrassing to take action”, or “they felt that they would not be believed, or nothing would change” (7, p. 35). For about one in four women, stressors are perceived as being too stressful or embarrassing to complain about the situation, and 22% think that changes would not occur if they complained. About one in ten fears consequences for further career steps [7]. However, a high prevalence of problem-focused coping strategies could be attributed to recruitment strategy and a possible selection bias, in which affected and committed women may tend to participate more often.
Attributed consequences
The most prevalent consequence for mental health reported in this study was “feeling emotionally upset”. This goes along with international findings in which stress and anxiety are reported to be the most prevalent consequences (48%) for mental health [6]. Results from Australia describe a higher prevalence of 72% who inform about stress and an influence on self-esteem and confidence [7]. This study adds an additional aspect for attributed mental health consequences, describing feelings of guilt or punishment because of the pregnancy.
In the context of attributed physical consequences due to pregnancy-related stressors at work, the most prevalent outcomes are exhaustion, listlessness, fatigue and sleeping disorders. These results go along with Russell et al. [6] who report that about one in four expecting women is affected by fatigue or exhaustion [6]. As possible attributed negative consequences for physical health due to pregnancy-related stressors at work, bleedings and contractions are described [6, 7]. Cross-sectional findings from Ireland describe only 2% of women reporting bleedings during pregnancy as an attributed consequence for physical health because of unfair treatment at work [6]. In the conducted survey, both are represented by 21.7% (n = 15). This could be traceable to a possible selection bias based on recruitment strategy with voluntary participation, especially women who are affected by pregnancy-related conflicting situations may tend to participate [33]. Furthermore, attributed social consequences like a strained relationship with their partner or husband, are described by nearly half of the women who experience stressors at work during pregnancy. This result goes along with Australian results who illustrate that 39% of the women who face discriminatory behaviour report an impact on their families [7]. In general, for future research, longitudinal study designs are needed, accompanying expecting women from the beginning of pregnancy, during maternity and parental leave. Likewise, more research is needed on the situation of self-employed women during pregnancy.
Strengths and limitations
Several strengths and limitations of the study should be addressed. Initially, this study represents the first survey in Germany which analyses stressors and coping strategies during pregnancy at work on a national level with a cross-sectional study design. Another strength of the study is related to a limited recall bias. Women who participated in the study were pregnant and employed at that moment. If a woman had already delivered or was not employed (or self-employed) anymore, she was excluded from the survey. Therefore, possible conflicting situations at work as well as available coping strategies and attributed consequences due to these stressors at work were still present.
However, different limitations should also be addressed when interpreting the results. Firstly, the study is based on a cross-sectional design and are only analysed in a descriptive way (percentages mainly referred to the sub-group of participants experiencing stressors during pregnancy), wherefore they need to be interpreted with caution. Data cannot be interpreted concerning causal relationships, for example, concerning the relationship between stressors and attributed consequences of stressors during pregnancy at work. Moreover, the study only consists of a small sample size wherefore external validity is limited. Especially single expecting women are underrepresented in the sample with three participating women (1.4%). In contrast, about 22.6% are single parents in Germany in 2018 [34]. Additionally, the data is not representative due to the online-based recruitment strategy.
Data was assessed from expecting women in a self-reported way. Therefore, it cannot be ensured that women enrolled in the study were necessarily pregnant and employed. Additionally, only one perspective of stressors in an occupational context during pregnancy was assessed, employers or observers view is missing to interpret the situation as a whole. Concerning objectivity of self-reported perceptions of pregnancy-related stressors a possible response bias is expected [33]. Therefore, data can only be interpreted in a limited way concerning objectivity. Furthermore, different recruiting approaches have different advantages and disadvantages. Firstly, women were recruited via flyers which were displayed at the offices of pro familia in Germany. One of the main offers of pro familia is counselling on pregnancy, sexuality and partnership which may introduce a selection bias.
Secondly, women were recruited via social media and pregnancy-related groups introducing a possible selection bias. The biggest disadvantage results from the fact that the sample cannot be drawn at random. 25 groups concerning pregnancy related topics were chosen to recruit expecting women in an active way. However, experiences with samples relying on online-based recruitment strategies indicate high levels of diversity concerning, for example, occupation or age [35]. Moreover, a volunteer bias was introduced based on voluntary participation.
Practical implications
Based on the conducted research, several practical implications with a (public health) relevance for managing pregnancies in an occupational context can be drawn. Results indicate that there is a need for addressing employer’s attitudes and behaviour. First of all, one of the main aspects is lacking pregnancy-related acceptance, knowledge and consideration, which may result in distancing employers or less appreciation of expecting mothers. Results of the study highlight these tendencies. Therefore, the first implication is described as: On the one hand, employers and management professionals are obligated to inform themselves concerning maternity protection and their obligation to maintain safe working conditions. The relevance is also emphasised by the German law reform on maternity protection in 2018. On the other hand, businesses should be supported with clear-structured guidance material from public and private agencies, for example by providing information online or by means of (low-threshold) counselling services, which are especially relevant for small and medium-sized companies. Information on employment rights as well as the development of health and safety information, also in a sector-specific way, are described as beneficial not only for employers but also for employees [6].
Moreover, the study indicates that negative pregnancy-related comments at work are a common reported stressor. The experiences women gain at work during pregnancy play an important role concerning further career decisions. Therefore, the second implication is addressed as: Employers should sensitise both first-line managers and employees concerning unfair treatment during pregnancy at work. HR management professionals should be obligated to seek information related to pregnancy-related discrimination and intervene with trainings and supervisions to inform about this topic.
The way pregnant women gain experience at work during their employment biography has an intrinsic effect on further career decisions. Being employed after maternity protection or parental leave is often a result of past support and appreciation [2]. Therefore, communication with employers or first-line managers during pregnancy and parental leave plays an important role. As a result, returning to work after pregnancy can be facilitated: To avoid pregnancy-related stressors and promote coping strategies, an ongoing communication and informational exchange between employers, HR and employees should be guaranteed during pregnancy (as well during maternity or parental leave). It is recommended to negotiate future changes and own wishes concerning the design of work with employers already during pregnancy and when returning to work, for example concerning communication during maternity/parental leave. Moreover, point of time and length of parental leave as well as flexible arrangements of work like working in part-time or trust-based working hours can be discussed.
In addition, companies should emphasise measures fostering the compatibility of family and career, which can have a positive impact on the reduction of time strain and psychological stress [36]. For example, the availability of part-time opportunities positively influences an employee’s return to work after giving birth, is important to the women’s well-being and is also associated with a lower incidence of crisis pregnancy [6]. In general, special attention should also be paid to women facing a higher risk of crisis pregnancy like younger ones, non-married women, women expecting their third or subsequent child and disabled women [6]. In this context, the offers should be tailored to the exact needs of the employees in a target group-specificmanner: Measures relating to working hours and organisation (e.g., part-time, individually agreed working hours, flexible daily and weekly working hours, trust-based working hours, mobile working, teleworking, job sharing or sabbaticals) can be used for this purpose, as well as parental leave and parental assistance (e.g., special consideration for parents, for example, when planning vacations, further support for parents, part-time or employment in phases during parental leave, explicit encouragement for male employees to take parental leave or part-time, financial benefits above the statutory level), childcare or family services (time off work due to children’s illness, further support for childcare, parent-child rooms in the company, temporary childcare or company childcare) or information and advice services (for example, part-time work during parental leave) [37]. The introduction of parental allowance in Germany represents a further component. It facilitates that women are more likely to return to work earlier and family and housework tasks are shared more equally. Overall, the greater involvement of partners in parenting contributes both to womens’ return to work and to a closer bond between partners and children [38].
Moreover, the sample is characterised by a lot of women seeking help in a problem-focused way, with an important role of the gynaecologist’s advice. The gynaecologist serves as a low-threshold contact person about pregnancy-related occupational questions for example concerning prohibitions of employment issues. To address coping strategies, the third implication considers: Gynaecologists need to be aware of their relevance as a contact person for women experiencing pregnancy-related stressors at work. Therefore, not only physical dimensions of health should be considered, but mental and social aspects should be reflected as well. Furthermore, gynaecologists should be informed about other problem-focused approaches in order to strengthen women’s coping strategies with offers on a regional level (e.g., legal advice, contacting employee organisations or counselling services).
Conclusion
All in all, this study is one of the first, which assessed stressors and coping strategies during pregnancy at work as a result of the pregnancy in a cross-sectional study design in Germany. Participating women reported most commonly intrapersonal stressors concerning fears related to the baby’s health or a preterm birth. In occupational context conflicting situations in relation to employer and colleagues were the most common ones, which were often based on negative pregnancy-related comments. Furthermore, several consequences were attributed to mental and physical health status of the expecting women. The most important consequences for mental health mentioned in the study dealt with being emotionally upset and having fears concerning the baby’s health. Physical health was affected by exhaustion, listlessness and sleeping disorders. Reducing mobbing issues and informing employers more holistic about pregnancy-related obligations are a main aspect due to the need of support or advice. Concerning possible negative (or discriminatory) experiences at work during pregnancy, more research is needed to provide representative results on a national level, claiming generalisability. Further research should address employer’s knowledge about maternity protection, maternity pay and implications for health in a German context. Furthermore, experiences during parental leave and return to work need to be highlighted as well.
Ethics statement
Ethical approval was inquired by the Medical Ethics Committee in Hamburg, Germany. Before starting the online survey, the participants were introduced to the purpose of the study and were asked to sign a declaration of informed consent. All participants took part in the survey voluntarily.
Conflict of interest
The authors declare that they have no competing interests.
Footnotes
Acknowledgments
The authors would like to thank all women who participated in the interview study and especially pro familia for supporting the promotion of their online study.