
Abstract
BACKGROUND:
Occupational blood and body fluid exposures (OBBFEs) are one of the biological risks run by health professionals, especially in hospitals.
OBJECTIVE:
The objectives of this study were to assess the occurrence and reporting of occupational blood and body fluid exposures (OBBFEs) in university hospital medical staff and to investigate factors associated to declared OBBFE and factors associated to reported OBBFE.
METHODS:
A self-administered questionnaire has been e-mailed to all junior and senior medical staff in four university hospital centers in one administrative region of France in 2017.
RESULTS:
292 of the 1,228 respondents declared at least one OBBFE. More than two-thirds (70.2%) were under-reporters and more than half (53.8%) non-reporters. Younger subjects, surgical specialties and other associated work accidents were risk factors for OBBFE. Considering the reporting procedure too complex was a risk factor for underreporting.
CONCLUSIONS:
Underreporting by hospital medical staff was a persistent phenomenon, with a high rate. The OBBFE reporting procedure needs rethinking.
Introduction
Occupational blood and body fluid exposures (OBBFEs) are one of the biological risks run by health professionals, especially in hospitals [1–4]. Over a 20-year period, from 1996 to 2016, health professionals in the University Hospital Center of Lyon, France reported around 18,000 OBBFEs: 40% for the nurses, 23% for the medical juniors and students, 9% for the medical seniors and 8% for the paramedical staffs. The Center’s OBBFE detection system reported a decrease in annual incidence of more than 30%, from 1,000 cases in 1996 to 700 in 2015 [5]. Nurses report more frequently than medical staff [6], whereas the latter show 4-5-fold greater risk according to Gańczak et al. [7], and 2-fold according to Nagao et al. [8]. Unfortunately, few data are available for medicalstaff.
Occupational health monitoring includes work-accident reporting as indicator of individual health status. Physicians’ health, and especially mental health status is a major concern [9], and can be approached by investigating sudden events such as work accidents.
In case of OBBFE, a specific procedure is advised, with immediate post-exposure care and assessment of the need for emergency preventive treatment and serology monitoring [10]. The OBBFE should also be reported as a work accident [11]. Analysis of work accidents, including OBBFEs, enables preventive measures to be taken to reduce or eliminate possible repercussions [12, 13].
Quantitative and qualitative analyses both need reporting of OBBFEs for having good comparisons with other data or for having relevant screening of risk factors and multiple causes of those OBBFEs. Underreporting OBBFE concerns all hospital staff and is difficult to analyze. For medical staff, previous studies found reporting rates ranging from as low as 2.3% [14] to as high as 75% [15]. These findings need to be taken with caution, as they usually did not take account of all the kinds of OBBFE and because reporting varies from country to country. Some studies found rates of 10.4% for needle or sharp instrument wounds compared to 0% for mucosal or cutaneous projection [16]. Another exposure recording network, EPINet, set up in the USA in the early 1990 s, found a 26.8% rate of skin wound reporting by surgeons and 54.1% by medical physicians [17]. A lower rate of 9.8% was found in Taiwan by the same network [18]. According to an older study, the real number of OBBFE needs multiplying 25-fold compared to registry data [19].
Underreporting is a bias that has to be borne in mind in analyzing OBBFE, especially when designing individual or collective preventive measures.
The objectives of this study were to assess the occurrence and reporting of occupational blood and body fluid exposures (OBBFEs) in university hospital medical staff and to investigate factors associated to OBBFEs and factors associated to reported OBBFEs.
Materials and methods
Study design
A cross-sectional multicenter study described the prevalence of blood exposure accidents declared by the medical staff and the prevalence of OBBFEs reported by the medical staff to the occupational health services in 2017.
The OBBFEs were counted as declared when they were declared in the questionnaire, and the OBBFEs were counted as reported if they were also declared to have been reported by the medical staff to the occupational health services.
Data were collected by an anonymous self-administered questionnaire emailed to all medical staff in four university hospitals in the Auvergne-Rhône-Alpes Administrative Region of France: Lyon, Grenoble, Clermont-Ferrand and Saint-Etienne.
The questionnaire was online during 2 months at the end of the first quarter of 2018. Two reminder emails were sent, between days 9 and 14 and between days 37 and 44. In one center, no reminder emails were sent following the initial e-mail.
Population study
The target population was the medical staff (medical physicians, surgeons, odontologists and pharmacists) of whatever status, seniority and specialty, working in one of the four university hospitals, with an active work email address provided by the hospital IT department. This population was separated in two groups for the descriptive analyze: senior and junior. A senior staff is a doctor who practices medicine after his PhD of medicine. A junior staff is a 6th year and higher of medicine student who works in a hospital in a specific speciality for learning practice. Junior medical staff were not consulted in one of the centers.
Other staff (paramedical, medical students, midwives, and technical, non-medical and administrative staff) were excluded.
Questionnaire
The questionnaire has been created for this study. It contained several groups of questions: OBBFEs exposure risk; Declared OBBFE in 2017, according to type of OBBFE (needle wounds or cuts, mucosal projections (onto oral and/or ocular mucosa), or cutaneous projections (onto wounded or diseased skin)); Reported OBBFEs according to type of OBBFE in 2017; OBBFE circumstances affecting reporting (conditional); Reported OBBFE related data; Psychosocial conditions at work (0–10 numerical scale); Risk awareness (viral seroconversion rate) and procedure (deadlines); Demographic and professional characteristics including specialties: medical, surgical and others specialties (psychiatric, public health, occupational and pharmacy specialties) and function (junior, senior and graduate hospital senior status).
The questionnaire was drawn up using the LimeSurvey application (version 2.05) and uploaded to the University Institute of Occupational Health and Medicine of Lyon website. The study had review board approval (CPP Ouest V) and was in conformity with data protection requirements (Commission Nationale de l’Informatique et des Libertés: CNIL).
Statistical analysis
A comparison according to the status of the medical staff (senior versus junior) was performed. Qualitative variables were compared on Chi-squared tests and quantitative variables on student or Kruskal-Wallis tests.
The two variables of interest were occurrence of OBBFEs (called declared OBBFE) and reporting all OBBFEs (called reported OBBFE). First analysis performed prevalence ratios for factors associated with having at least one OBBFE in 2017, in univariable and multivariable steps. Second analysis performed prevalence ratios for factors associated with none or not all reported OBBFEs (n = 205), versus all reported OBBFEs (n = 87), in univariable and multivariable steps.
Prevalence ratios (PR) assessing association between the variables of interest and explanatory variables were estimated on log-binomial regression models and the statistical package’s GENMOD procedure.
Modeling strategy was similar in both analyses: univariate analysis of association between variable of interest and explanatory variables, and multivariate analysis of explanatory variables with p-values ≤10%. Descending selection was applied. The significance threshold was set at 5%. All analyses were performed with SAS software, version 9.4.
Results
The population targeted by the study totaled 6,477 senior and junior medical staffs. 1,495 medical professionals participated and 1,228 questionnaires were fully filled out. The participation rate was thus 23.1%, and the complete response rate 19.0%.
292 (23.8%) of the 1,228 respondents declared having had at least one OBBFE in 2017 (Table 1), with a significant difference according to the status (32.6% for the junior and 21.2% for the seniors, p < 0.0001). The total of OBBFEs declared was 869 for the year (588 for the seniors and 281 for the juniors). OBBFEs were mostly needle wounds or cuts: 578 (66.5%), compared to 240 (27.6%) mucosal projections and 51 (5.9%) cutaneous projections, and incidence of each type of OBBFE were significant different according to status. There was no significant difference of the mean of declared OBBFEs between seniors and juniors (Fig. 1). Mean incidence of OBBFE was 2.98 (standard deviation sd = 3.46) per medical health workers, including 1.98 (sd = 2.26), for needle wounds or cuts, 0.82 (sd = 1.71) for mucosal projections and 0.17 (sd = 0.91) for cutaneous projections.
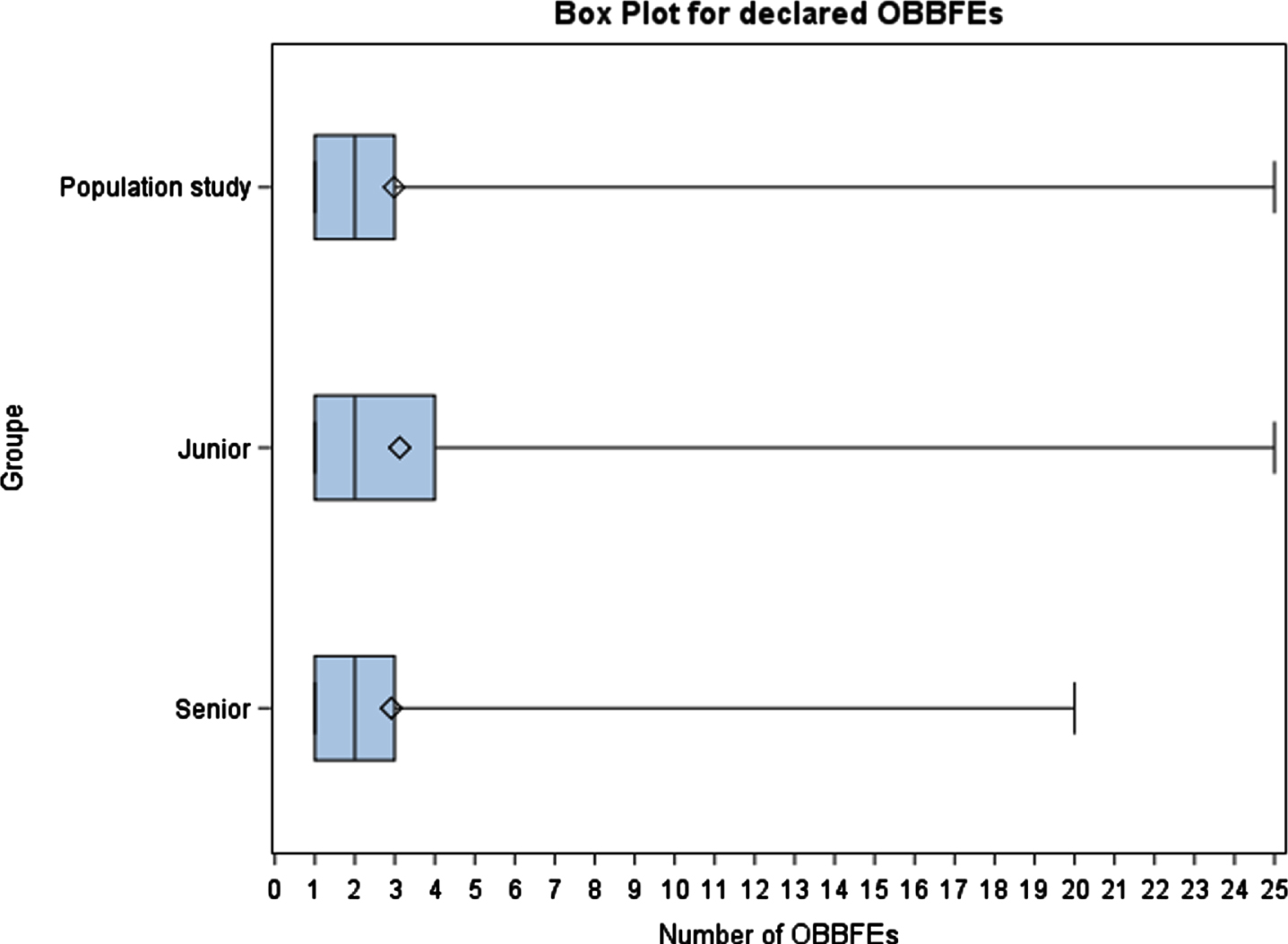
Boxplots for declared OBBFEs.
Description of declared and reported occupational blood and body fluid exposures (OBBFEs) according to function
p-value: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001.
Among 292 medical health workers who declared having had at least one OBBFE, 70.2% (205/292) reported OBBFE only partially or not at all (Table 1). In totally, 163 OBBFEs were reported: i.e., a reported rate of 18.75%; 108 (18.4%) by senior and 55 (19.6%) by junior staff. There was no significant difference of the mean of reported OBBFEs between seniors and juniors (Fig. 2). Senior staff reported a mean of 0.53 OBBFE each (standard deviation = 0.62), including in mean 0.54 needle wounds/cuts (sd = 0.64), 0.23 mucosal projections (sd = 0.49) and 0.11 cutaneous projections (sd = 0.47) per person. Junior staff reported a mean of 0.61 OBBFE (sd = 0.82), including in mean 0.53 needle wounds or cuts (sd = 0.63), 0.14 mucosal projections (sd = 0.49) and 0.33 cutaneous projections (sd = 0.58).
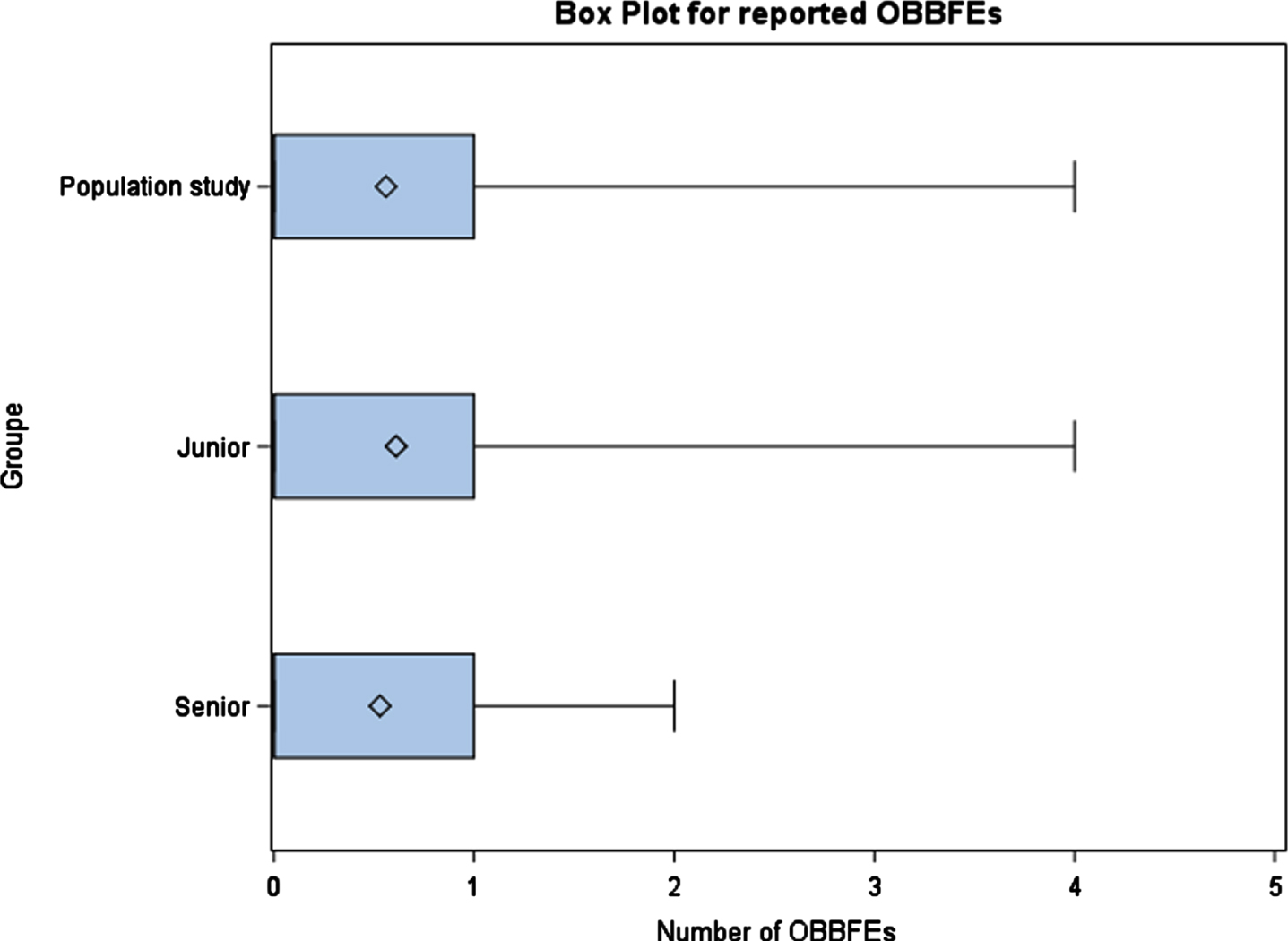
Boxplots for reported OBBFEs.
Self-assessed exposure risk and actual occurrence of OBBFE were independent: no self-assessed exposure in 164 cases of OBBFE (13.4%), self-assessed exposure in 1,064 (86.6% p< = 0.0001). Self-assessment of exposure risk and reporting of OBBFE, on the other hand, were not independent: no self-assessed exposure in 5 cases of OBBFE reporting (1.7%), and self-assessed exposure in 197 (98.3% p = 0.2). Individuals considering themselves exposed to OBBFE risk were 80% more likely to report all OBBFE they underwent, although the difference was not significant (PR = 1.8; 95% CI [0.6 – 5.2]; p = 0.2).
In univariate analysis (Table 2), declared OBBFEs were associated to a lower age (prevalence ratio PR = 1.5 for 40–49 years old, PR = 2.0 for 30–39 years old and PR = 2.5 for 20–29 years old versus more than 50 years old). The medical status of junior (PR = 1.7) was significantly a risk factor as having a graduate hospital status (PR = 1.4) versus hospital seniors. Working in the surgical specialties was significantly associated with declared OBBFEs (PR = 4.3 versus medical specialties). People who worked on night duty were more at risk to declare OBBFEs (PR = 1.6), as well to be on-call (PR = 1.4) and to have declared other work accidents during 2017 (PR = 3.3).
Sociodemographic and professional factors associated to declared occupational blood and body fluid exposures (OBBFEs) and to reported OBBFEs
p-value: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001. ¶Others: Psychiatric, public health, occupational and pharmacy specialties.
These factors were not associated with OBBFE reported, except for surgical specialties, with 40% greater underreporting than medical specialties (p< = 0.0001).
Only a high level of stress was associated with an OBBFE (PR = 1.4) whereas ability to conciliate working life and personal life and autonomy were both protective factors (Table 3).
Psychosocial factors associated with declared occupational blood and body fluid exposures (OBBFEs)
p-value: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001.
Among the behavioral factors, underreporting was associated with perceived reporting procedure complexity, negative source-patient serology, fear of personal serology revealing seroconversion, failure to recognize the OBBFE as such, and all circumstances of OBBFE occurrence tested (Table 4).
Behavioral factors after an occupational blood and body fluid exposures (OBBFE) associated with underreported OBBFEs
p-value: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001.
On multivariable analysis, occurrence of at least one OBBFE in 2017 was significantly associated with younger age groups (PR = 1.7 95% CI = [1.2–2.3] for 20–29 years and PR = 1.6 95% CI = [1.1–2.2] for 30–39 years), surgical specialties (PR = 3.6 95% CI = [1.1–2.2]), and other work accident(s) during 2017 (PR = 1.5 95% CI = [1.3–1.8]) (Table 5).
Multiple factors associated with declared occupational blood and body fluid exposures (OBBFEs)
p-value: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001. ¶Others: Psychiatric, public health, occupational and pharmacy specialties.
On multivariable analysis, underreported OBBFE was significantly associated with perception of the reporting procedure as being unduly complex (PR = 1.3 95% IC = [1.1–1.6]). Deep needle wounds (PR = 2.6 95% CI = 1.8–3.6]) or solid needle wounds (PR = 1.2 95% CI = 1.0–1.4]) were not criteria for systematic reporting; no such associations were found for other circumstances tested on univariate analysis, such as source-patient with HIV or hepatitis C (Table 6).
Multiple factors associated with underreported occupational blood and body fluid exposures (OBBFEs)
p-values: *p < 0.05; **p < 0.01; ***p < 0.001; ****p< = 0.0001.
For medical workers who did not report all their OBBFEs (n = 205/292), post-exposure action was taken systematically in 69.8% of cases and never in 0.5% (a single individual). Source-patient serology was performed systematically by 52.7% of underreporting respondents, and never by 13.2%. Personal serology was performed systematically by only 15.1%, and never by 48.8%.
There was a significant difference between junior and senior staff in risk awareness in response to the question about viral seroconversion rates for HIV (human immunodeficiency virus) (34.7% for seniors versus 8.4% for juniors, p< = 0.0001), HCV (hepatitis C virus) (38% versus 10.6%, p< = 0.0001) and HBV (39.1% versus 12.4%, p< = 0.0001). Post-exposure actions were generally well undertaken (i.e. immediately: 1,192/1,227; 97.2%), unlike serologic work-up on the source-patient (immediately: 537/1,227; 43.8%), without difference between juniors and seniors (p = 0.3). Post-exposure prophylaxis was implemented more efficiently by junior staff, only 2.2% of whom (6/276) did not know what time-interval was recommended, versus 13.6% of seniors (129/951), this difference being significant (p< = 0.0001). Timing of personal post-exposure serology (up to 7 days) was poorly known: 66/276 (23.9%) of juniors versus 128/952 (13.4%) of seniors, with a significant difference (p = 0.0005).
70.2% of medical staff with at least one OBBFE in 2017 did not report all of them and 53.8% reported none: i.e., more than half never reported OBBFE, and fewer than 1 in 5 OBBFE were reported. These rates are higher than in the literature. In a French study, 35% of junior and recently graduate Accident and Emergency Physicians were non-reporters [20], and the authors concluded that non-reporting is still a major issue; two-thirds of under-reporters esteemed the procedure too long, in agreement with the present findings. The main risk factors for OBBFE this study were being less than 39 years, surgical specialties and additional work accidents. Subjects likely not to systematically report solid needle or deep needle wounds tended to under-report, whatever the type of OBBFE actually sustained. Finally, procedural complexity influenced reporting.
The present findings were similar to those of a Swiss study, in which 67.1% of physicians (whether they performed invasive procedures or not) were underreporters, but for different reasons, mainly consisting in low risk of infection [21]. In the present study, source-patient serology negative for HIV, HBV and HCV was associated with underreporting (on intermediate analysis, PR = 1.3; 95% CI = [1.0–1.8]; p = 0.02), although this factor no longer emerged on multivariate analysis.
Classically in prevention, risk awareness may alter behavior, reducing the number of accidents [22]. Sustaining at least one OBBFE was strongly associated (PR = 8.9; 95% CI = [3.7–21.2]; p< = 0.0001) with risk awareness, although 5 of the 292 OBBFEs victims still considered themselves non-exposed. Although the difference was not significant, considering oneself exposed to OBBFE risk increased reporting by 80%. A previous study found that freedom from bad luck for infectious diseases was a sufficient reason for non-reporting [23], cited by 15.3% of non-reporters, and can be assimilated to poor judgment of repercussions. The proportion was similar in the present study, although the source-patient being considered not to be at risk or having negative serology did not finally emerge as a determining factor on multivariate analysis, unlike in several other studies [7, 25].
Younger age was a risk factor for occurrence of OBBFE, and seniority a protective factor. On the other hand, seniority is associated with underreporting [26]. In junior staff, it is less clear that relative seniority has a protective effect, as juniors perform ever more at-risk procedures during their increasing training [27]. Juniors were at greater risk of OBBFE (32.6%) in 2017 than seniors (21.2%) (p< = 0.0001), as previously reported elsewhere [28].
Surgical specialties were at 3.6-fold greater risk of OBBFE than medical specialties (p< = 0.0001). This pattern is constant over time; in 1999, Ippolito et al. [29] found an annual rate of 12 OBBFEs per 100 surgical posts, compared to 3.86 for medical posts, comparable to the present findings. Alongside this higher risk, however, surgeons were 40% more likely not to make a report; likewise, Panillio et al. found that medical specialists reported twice as often as surgeons [17].
The reporting procedure is included in post-OBBFE guidelines, along with antisepsis and personal and source-patient serology. Some of these steps are poorly known or poorly applied, especially in the case of personal serology [30]. The reporting process itself was a major factor in underreporting in 2017. Stressful working conditions, along with time pressure, might be supposed to be limiting factors. As in other French and British studies [31, 32], the burdensomeness of the reporting procedure was mainly highlighted. Failure to report has consequences, in terms of health insurance (specific to work accidents), individual health (lack of requisite prophylaxis) and collective work-place health (failure to locate dangerous situations). While 62% of junior staff report OBBFE to their administrative department, only 51% report to the occupational health department [31], making accidentogenic situations harder to identify, being less often reported to the occupational health department.
Another factor for underreporting was that solid needle or deep needle wounds were not considered to be criteria for systematic reporting. Mucosal or cutaneous projections are known to be less often reported than skin wounds [16, 25], and this was also found in the present data, but underreporting of solid needle or deep needle wounds are another aspect of defective risk awareness: the risk of HCV transmission is known to be lower via a solid needle than a hollow needle containing arterial or venous blood. The depth of the needle wound is also an aggravating factor for HCV transmission [33]. Wound depth is the parameter most closely associated with risk of HIV transmission; hollow needles show weaker association [34]. Then, a recent study showed that splash sharps and needlestick injuries impacted on healthcare workers quality of life [35].
The present data point to significant conclusions regarding the occurrence of OBBFE, but no associations between psychosocial working conditions and underreporting emerged. Some studies focused on the traumatic consequences of OBBFE [36], and others on the relation between depressive symptoms and the occurrence of OBBFE [37].
Further prospective studies are needed to discern relations between individual management (work accident reporting) and psychosocial risks [38].
Numerous studies find a reduction in underreporting rates [15, 39–41]. Notably, in 2015, Yonezawa et al. [41] found increased reporting to be the only explanation for the continual annual increase in rates of sharp or blunt object wounds. In France, in the same year, the RAISIN-AES network [3] found a 23% fall in overall incidence of OBBFE. The role of underreporting in this is thus a good question. Further studies are needed to clarify present trends in OBBFE reporting.
The present study has certain strong points, being multicenter, with a large sample, but also some weaknesses.
The retrospective design incurs a risk of memory bias when subjects are asked about past events. A social desirability bias cannot be entirely ruled out with regard to a burning topic like infection risk in a hospital setting and the possible nosocomial consequences of transmission from caregiver to patient [42, 43]. The low response rate raises the possibility of recruitment bias, although it is not clear whether this would lead to over- or underestimation. Likewise, junior staff answering the questionnaire may have been working outside of the university hospital at the time of the study, as they move from one hospital to another.
The fact that the study dates from 2017 may be a limitation, but that it avoided exceptional health situations that would not reflect a generality but a specific case [44]. Finally, the cross-sectional design precludes causal analysis, as the time-sequence of events is lost: e.g., it was difficult to establish the links between other work accidents in 2017 and the OBBFE.
Conclusion
In conclusion, the present study highlighted the importance of individual (age) and occupational factors (specialty, work accidents) in the occurrence of OBBFEs and of organizational factors (reporting procedure) in underreporting in 2017. Risk assessment and perception by medical staff are predominant factors in managing biological risk.
Given its declared complexity, the reporting procedure needs rethinking, to remove this obstacle. Moreover, future research should focus in those factors that prevent the reporting. Then, research should also focus on the relationship of psychosocial and/or behavioral aspects with OBBFE risk in university hospital medical staff.
Implications for behavioral health
The importance of individual (age) and occupational factors (specialty, work accidents) in the occurrence of OBBFEs The importance of organizational factors (reporting procedure) in underreporting of OBBFEs in 2017 Risk assessment and perception by medical staff are predominant factors in managing biological risk The reporting procedure needs rethinking, to remove this obstacle of given its declared complexity Research should also focus on the relationship of psychosocial and/or behavioral aspects with OBBFE risk in university hospital medical staff
Conflict of interest
None to report.