
Abstract
BACKGROUND:
The perceptions and trends of magnification use in dentistry need to be determined since magnification significantly enhances clinical practice.
OBJECTIVE:
To assess perception and practices of Operative and Endodontic specialists currently working in Pakistan, regarding use of magnification.
METHODS:
A structured questionnaire administered for this analytical cross-sectional study recorded demographics, trends of magnification devices used in practice and their perceived advantages and disadvantages by the specialists with close-ended questions and three-point Likert scale.
RESULTS:
Out of 91 forms, 77 responses were received (response rate of 84%). Most participants had 1–4 years of practical experience, were employed at both faculty and clinical positions, were more interested in operative/restorative procedures and used TLL (through the lens loupes) at low magnification. Use of magnification devices was learnt mostly during post-graduate training and was used daily or weekly for complicated cases. Noteworthy perceptions included improved treatment quality and standard of care. However, they were also perceived as irritating, increasing treatment time, with adverse effect on eyesight with prolonged use. No statistically significant correlation was found between the variables recorded (p > 0.05).
CONCLUSIONS:
Most specialists used magnification devices in some form and were abreast with their advantages. Proper training and continued dental education courses can help dispel any observed misapprehensions.
Keywords
Introduction
Before the introduction of magnification in dentistry, dentists usually relied on tactile sensitivity and radiographs while performing clinical procedures, including endodontics [1]. Procedural errors were dealt mostly through dentists’ mental imaging and patience, resulting in an increased chance of iatrogenic mishaps, errors and increased treatment time. With the introduction of magnification devices in dentistry, not only Endodontists but other dental specialists gradually incorporated the routine use of loupes, dental operating microscope (DOM) and other magnification aides into their clinical practice. High visual acuity is possible with these devices, which is considered an asset while performing dental procedures on patients. Apart from improved vision, other potential ergonomic benefits for the clinician include an improved posture which subsequently reduces musculoskeletal stress [2, 3]. Currently, magnification devices are even being used for simple dental procedures ranging from scaling and polishing, caries removal, preparing crown margins to more complicated ones including locating canals, repair of perforation and furcation, placement or removal of post and grafting procedures involving bone and soft tissues [4].
Among the various magnification devices that have become available over time, the dental operating microscope (DOM) offers highly superior visualization while performing endodontic surgery [5]. DOM was introduced to the Endodontic specialty by Dr Gary Carr in the 1980s [6]. An endodontist could benefit from the use of a Dental operating microscope (DOM) in detecting hidden or extra canals. It also helps during retreatment cases for removing posts, fractured instruments and repairing any mishaps like ledges and perforations [4].
The objective of this study was to assess the perception regarding advantages and disadvantages of magnification use, as well as the practice of Operative and Endodontic specialists trained and currently working in Pakistan, related to the use of magnification devices. The vast majority of Operative and Endodontic specialists in Pakistan acquire their postgraduate diploma (Fellowship of College of Physicians and Surgeons or FCPS) after completing their clinical training in training centers recognized by the College of Physicians and Surgeons, Pakistan (CPSP). Even though there are studies assessing the practices of magnification use by endodontists from other regions [7, 8], currently there is no published data on use of magnification devices by Operative and Endodontic specialists in Pakistan [6, 9]. The results of this study will help to identify the trends of use of magnification devices by Operative and Endodontic specialists and if any misconceptions are found hindering the use of such devices, then recommendations can be made to incorporate the routine use of magnification devices in the future training of Operative and Endodontic specialists. Factors identified as deterrents to magnification usage would be identified and suggestions to ensure availability and incorporation of routine magnification may be put forth.
Methodology
A structured questionnaire was designed and administered for this analytical cross-sectional study. The questionnaire was composed of items that were compiled after extensive literature search of published studies with similar methodologies recording trends of magnification use and perception among dentists and dental specialists [6, 9–13]. All such studies were downloaded, and each item of every questionnaire was carefully reviewed. The common themes and items were collated to develop the questionnaire which had three components. The first component was to record the demographics of the respondents including the duration of their clinical practice and their current professional responsibilities. The second component comprised of closed ended items to assess trends of magnification use in clinical practice of the participants. Closed ended items were used to acquire specific responses which would be convenient to analyze. The third component was based on a three-point Likert scale. This part assessed the perceived advantages and disadvantages of the use of magnification devices by the specialists.
All Operative dentists and Endodontists who had successfully completed their fellowship training (FCPS) in Operative Dentistry, had been awarded their post-graduate diploma from the College of Physicians and Surgeons, Pakistan (CPSP), and were currently involved in clinical practice in institutional or private setups within Pakistan were included in our study. Those practitioners, who were not currently doing clinical practice, were practicing abroad or those who did not consent to be part of the study were excluded.
After approval from the ethical review board, the structured questionnaire was uploaded on Google forms and piloted by administering it to 10%(10 specialists) of the total number of specialists fulfilling the inclusion criteria (N = 101). These specialists were not included in the final sample of the study. In the light of the feedback received during the pilot process, and any discrepancy or ambiguity observed in the items, the questionnaire was modified. The internal consistency of the questionnaire was also assessed as part of validating the items, which showed Cronbach’s alpha of 0.76.
The finalized questionnaire and consent form were then administered to the remaining specialists fulfilling the inclusion criteria across Pakistan (n = 91) by sending a Google Form link using WhatsApp. The data was collected electronically during the period between April and May 2020. Any queries related to the questionnaire items were addressed on e-mail. The forms were individually scanned by the researchers to identify any missing data.
Data analysis
SPSS 20.0 was used for data analysis. Descriptive analysis was done by calculating percentages for categorical data. To determine relationships between categorical variables, chi-square test was used, keeping level of significance at p < 0.05.
Results
A total of 77 responses were received (response rate of 84%). Data for the years of experience after the completion of postgraduate training showed that the majority of respondents (37.7%) had 1–4 years of relevant experience. While looking into the professional responsibilities of the respondents, it was seen that 58.4%of the specialists were appointed on both faculty and clinical positions (See Table 1).
Demographic data of participants (FCPS trained Operative and Endodontic specialists)
Demographic data of participants (FCPS trained Operative and Endodontic specialists)
Table 2 shows area of interest, the type of magnification devices used by the specialists, preferred level of magnification and frequency of magnification devices used in the practice of Operative and Endodontic specialists.
Participants preferences for clinical procedures, magnification device, level of magnification and frequency of use
Only the respondents who affirmed their use of magnification devices (n = 58) subsequently responded to the questions regarding the frequency of using magnification devices based on the nature/complexity of procedure (Fig. 1) and the type of procedures for which they used magnification devices (Fig. 2). It was seen that the majority of participants who used magnification utilized it for locating hidden canals, negotiating calcified canals, retrieval of broken files, bypassing ledges, perforation repair and crack detection.

Frequency of magnification use by respondents employing magnification devices based on nature of procedure.

Procedures for which participants (n = 58) reported using magnification.
Majority of specialists reported having the opportunity to learn magnification use during their post graduate training, followed by trial-and-error (Fig. 3).
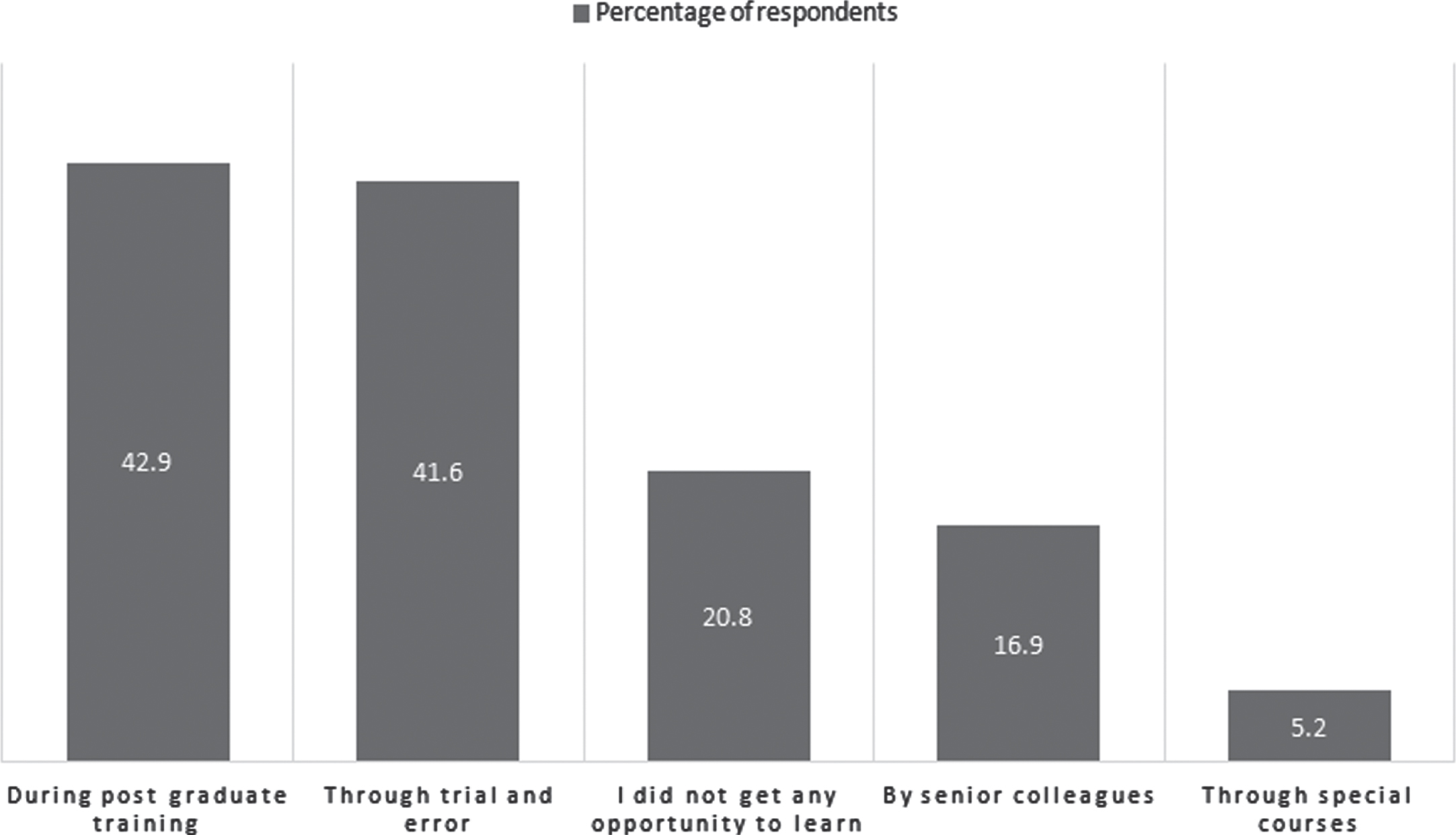
Responses related to learning opportunity for magnification devices.
No statistically significant difference could be found between the years of experience and the preference for level of magnification, the frequency of use of magnification devices, as well as the current responsibilities of the participants (p > 0.05).
The responses of the Operative and Endodontic specialists for the perceived advantages and disadvantage of the usage of magnification devices were categorized into themes and are given in Table 3. The themes included treatment quality, types of procedure, length of procedure, learning curve and difficulty of use, maintenance and sterilization of magnification devices, effect on posture and vision as well as expense of using magnification devices. In summary, the majority of participants agreed that use of magnification improved treatment quality, especially in complicated and retreatment cases. They also agreed that a trained assistant is needed if magnification devices are to be used efficiently. Also, there was agreement that magnification use maintains good posture and prevents fatigue, but it adversely affects eyesight and there is tendency for dependence with constant use. However, there was divided perception as to the time needed for positioning, the hassle involved in disinfection of such devices and their expensive. The participants disagreed that the treatment time becomes longer with magnification devices, it is difficult to get accustomed to their use and their maintenance is difficult.
Summary of the perceived advantages and disadvantages of magnification devices by Operative and Endodontic specialists
This study focused on acquiring data regarding the trends of using magnification devices by Operative and Endodontic specialists in Pakistan. Through this study, the trends of practice and perceptions regarding the use of magnification devices by these specialists was explored, in order to assess the frequency of magnification use, the magnification devices being utilized and how specialists perceive the use of such devices. Even though most studies assessing the trends of using magnification in dentistry have focused on the use of dental operating microscope (DOM), our study has attempted to identify the current practices of Operative dentists and Endodontists regarding use of various magnification devices [14].
The majority of the responders in our study were found employed at faculty positions as well as working in private practice. This is the usual trend seen in FCPS trained specialists, since faculty positions in dental institutes in Pakistan require the completion of postgraduate studies for induction as faculty, as outlined by the regulations of statutory council locally. Specialists who reported using magnification devices described using them daily or weekly, and majority of the specialists utilized them for complicated procedures. It is encouraging that a large percentage of Operative and Endodontic specialists working in Pakistan use some form of visual magnification device during the procedures they perform, albeit daily, weekly or monthly. The dental practitioners who seldom use magnification can be encouraged to make magnification use part of their daily practices based on the evidence highlighting the advantages of magnification devices. From the results of our study, it was also seen that the more experienced specialists were using magnification for almost every procedure.
Our study showed that the majority of the participants used through the lens loupes (TTL) and simple loupes, with low level of magnification (3x–8x) which is suitable for most operative procedures. These devices are relatively inexpensive and easy to use. This was similar to another study done on students and residents in Saudi Arabia, where loupes were the most widely used form of magnification [6]. In contrast, in our study DOM was used by very few practitioners. The routine use of DOM may be less in Pakistan due to difficulty in access to this magnification device as well as it being highly expensive, requiring high maintenance. The level of magnification required for various clinical procedures depends upon the operating field of the procedure. Procedures with limited operating field require higher magnification such as that provided by a DOM [14]. The procedures for which magnification has been used most commonly by participants who affirmed the use of magnification devices included locating hidden canals and negotiating missed canals, as well as retrieval of broken instruments. The advantage of using magnification devices like the DOM in Endodontics is enhanced access to the chamber floor, which aids in localizing canals. Also, complete cleaning of the canals can be ensured before placement of the obturating material. Visibility is significantly improved for removing any posts or repairing perforations because of increased illumination. Finding and treating extra canals is facilitated especially in maxillary and mandibular molars. In fact, it has been recommended by the American Association of Endodontics (AAE) that the use of DOM could greatly assist in locating the MB2 canal in maxillary molars among other endodontic specific procedures [5]. Use of DOM along with the micro-surgical instruments allows for a more conservative approach while performing periradicular surgery and makes complicated cases easier to manage [14], as agreed by the participants of our study. It is a good indicator that specialists believe in the benefit of magnification towards procedure quality and ultimately improved prognosis. They were found aware that magnification use, especially in the field of endodontics, is considered the standard of care [6]. A survey done on clinical faculty showed that 91%of the participants using magnification believed that the use of a magnification device provides significant benefits for patient as well as clinicians [10]. There are many studies supporting the improved outcomes of those endodontic procedures in which magnification was used [12, 15]. This was especially found true in cases where the MB2 canal of maxillary molars was missed during the primary root canal treatment [16].
Specialists included in our study agreed that magnification can be used for all procedures. However, at the same time they were also of the opinion that most routine clinical procedures can be done without it. This contradictory understanding for magnification used could be the reason for a diminished regular use of magnification devices in the practices of Operative and Endodontic specialists in Pakistan and may be based on various factors that were identified in this study, including possible effect on eyesight, requirement of trained assistants and the expense of magnification device purchase and maintenance, discussed further on. Even though the use of magnification devices is not a novel idea in dentistry, however in the context of the Diffusion of Innovations theory given by Rogers, perhaps the necessity is to disseminate the advantages and utility of these devices in our professional community subsequent to the reluctance observed in dental specialists in taking advantage of this technology [17]. This can be accomplished in academic settings and through professional seminars and conferences, so that magnification practices can be adopted by a larger number of practitioners. This would aid in modifying the current acceptance of Operative and Endodontic specialists towards the routine use of magnification.
No significant concern was conveyed by the specialists regarding the increase in the overall length of the procedure when magnification is used. The explanation for this observation could be that most specialists reported using simpler magnification devices which do not require significant time for adjustment or positioning. Most of the specialists included in the study found the use of magnification devices irritating. An essential reason could be unfamiliarity with the proper use of magnification devices. There is a learning curve to using magnification devices, which becomes steeper as the devices become more sophisticated and advanced. Any minor hand movement feels exaggerated under magnification, and hand-eye coordination needs to be re- established [18]. However, there was an agreement that overall, it is not difficult to learn how to use magnification devices. It has been found the dentists who are already habitually using any form of simple magnification devices like loupes, find it easier to transition to higher magnification devices like the DOM [19]. Also, there was no clear demarcation in the responses regarding the difficulty in positioning patients and themselves when using magnification devices during procedures. The ambiguity could be due to the different types of magnification devices being used by the specialists who participated in this study.
The efficient practice of dentistry requires professionally trained dental assistants, which ensures the smooth execution of dental procedures. Our study participants were of the opinion that to effectively use magnification devices, dental assistants also need to be suitably trained. Their training could include adjustment, maintenance and cleaning of magnification devices that the dental specialist may be using. A properly trained dental assistant would support the practice of the dentist by ensuring the timely availability of the magnification device as and when needed.
Responses related to maintenance and disinfection of magnification devices were variable. Most participants considered that it was difficult to maintain the optimum working of magnification devices. The result could be that specialists may be using a variable range of magnification devices from the low maintenance simple loupes to DOM, which requires significant maintenance. In order to minimize contamination, optimum working distance, use of high-volume suction and use of protective covers over loupes should be used [19]. Manufactures’ instructions should be followed for maintenance and servicing for ideal functioning of such devices.
Another aspect explored in this study was the possible adverse effect of using magnification devices on eyesight. It was found that a high number of responders were of the opinion that magnification adversely affects eyesight and may lead to dependence on prolonged use. This is similar to another study where the greatest fear of dentists was reported to be the weakening of the eyesight with the use of magnification devices [20]. This fear is unfounded, as there is no evidence which supports this apprehension. There is also the fear of growing dependence on magnification devices with continued use. In another study, dentists reported not wanting to become dependent on magnification devices with prolonged use [21]. It has been found that magnification devices that are not corresponding to the visual acuity of the user can cause problems like eyestrain or headache. It is therefore advised that when magnification devices are initially used, professional assistance regarding the most appropriate fit and specifications be sought. Another recommendation is to not wear magnification devices for all procedures, rather use them for selected procedures in order to prevent the psychological feeling of missing details in case magnification devices are not available. This will also help keep the eyes accustomed to working with normal vision [22].
A large number of specialists were of the opinion that the use of any magnification device actually helps to improve the posture of the practitioner, as well as reduces the risk of fatigue. Similarly, other studies reported that use of dental loupes reduced pain in arm, hands and neck [23]. Ergonomics is an important consideration in dental clinical practice, since it has been observed that dentists face significant musculoskeletal fatigue due to the nature of the procedures they perform [24–26]. In light of this, appropriate selection and use of magnification devices which facilitate the dentist in minimizing repeated fatigue by improving his/her vision could greatly curtail the incidence of musculoskeletal disorders in dental practitioners. Important considerations are the correct focal length, declination angles and alignment of the magnification devices pertaining to each individual operator in order to ensure prevention of problems like back and neck pain and poor posture.
A concern with the use of magnification devices for most specialists was the expense of such devices [19]. Even though in our study most of the participants were unsure about the expense of using magnification devices, nonetheless in a developing country like Pakistan, the profession of dentistry suffers due to low per capita income of the population resulting in diminished affordability of the majority of people to pay for even routine dental procedures. In addition, there is currently no national or provisional health care policy or program which covers dental procedures [27]. In the face of this fact, practitioners may be reluctant to invest in relatively expensive visual magnification devices such as a DOM, as they might risk lack of returns on any considerable financial investments towards their practice. Expense has been expressed as a concern to magnification use in other studies as well [11, 13]. However, with the exponentially increasing use of magnification devices globally, simpler devices like loupes are no longer as expensive as when they were considered a novelty. There is a wide range of magnification products and devices with various specifications and cost available today. Therefore, the dental specialists should explore these options and choose the device most suitable and affordable to their dental practices, instead of completely forgoing the idea of magnification use because of the perceived expense. Perhaps recommendations based on current evidence regarding the benefits of magnification devices in terms of visual advantages and decrease in postural fatigue could be made to the relevant authorities, in order to help in subsidizing the cost of such devices. This measure, along with provision for payments in installments or funding for purchase of magnification devices could help encourage their use in dental students and specialists alike.
Limitations
One limitation of this study was that only practitioners who had fellowship or post graduate diplomas from CPSP in the specialty of Operative dentistry and Endodontics were included, even though many general practitioners may be using some form of magnification in their clinical practice. Hence, there were a limited number of participants that could be included in our study. Also, specialists involved in other clinical dental fields including periodontology, implantology or oral surgery may also be employing various magnification devices for specialty specific procedures, but they were not included in this study. For a lot of practitioners, the use of magnification devices particularly those which are relatively expensive like the DOM is commensurate with the ease of access, availability and affordability. Therefore to explore this particular aspect, only specialists from Pakistan currently practicing within the country were included. Usually, specialists trained from Pakistan but practicing elsewhere globally have a better opportunity to work with magnification because of well-equipped public and private practices, hence they were not included in our study. We also did not explore the formal teaching practices related to the actual usage of magnification devices in post-graduate training, which would give an idea regarding any lacking in the propagation of the use of magnification devices at that particular stage of learning and practice of post-graduate trainees.
Recommendations
In light of the results of this study, it is recommended that any misconceptions about the use of magnification devices like adverse effects on eyesight and perceived difficulty in learning its use and positioning should be dispelled by formal training of Operative and Endodontic trainees at the post-graduation level. This would ensure that they are comfortable in routinely using an appropriate magnification device in their clinical practice. Further research into the training and use of magnification devices during postgraduate training could be conducted in order to identify teaching and training practices which could influence subsequent trends of using magnification devices in actual practice.
Conclusion
Most of the Operative and Endodontic specialists in Pakistan were found using Magnification devices in one form or another and the majority was abreast with the advantages of using magnification devices in their clinical practice. However, there were also some misconceptions present, particularly related to the possible adverse effect of using magnification devices during practice. Also, there were divided opinions regarding some aspects of magnification use including the routine use of such devices for regular clinical practices. With the propagation of training and continued dental education courses based on current evidence, such and any other misapprehensions can be dispelled, so that Operative and Endodontic specialists in Pakistan would be motivated, encouraged and educated to initiate and continue performing clinical procedures in the most efficient way utilizing magnification devices.
Conflict of interest
The authors do not have any conflict of interest to report.