
Abstract
BACKGROUND:
There is willingness in Europe to implement the use of a biopsychosocial model such as the International Classification of Functioning, Disability and Health (ICF) for assessing work incapacity.
OBJECTIVE:
A preliminary study was conducted to investigate the perceptions of medical advisers on the value of structuring clients’ biopsychosocial information in an ICF-based report.
METHOD:
A sample (n = 101) received a perception questionnaire after watching two comparative videos based on a clinical case. Questions relating to work incapacity were also asked. The data was analysed using quantitative methods. Comments were also collected.
RESULTS:
Before knowing the ICF-based report, 61.96% of the respondents believed a return to work seems possible by providing adapted work or a different job. There is an increase of 8.69 pp (p-value: 0.077) after reading the report. Opening up the initial sample to more insurance physicians (n = 119), the difference is more significant (p-value: 0.012). Also, 71.9% of respondents believe they have a better view of the client’s biopsychosocial situation after reading the report. Respondents recognise the clinical and diagnostic relevance of ICF but say it cannot be used at the moment for various reasons, such as the time required or the need for a multidisciplinary team and effective coordination. Older respondents are less enthusiastic about the appropriateness of using ICF.
CONCLUSION:
The respondents identify an added value in having a biopsychosocial based-report. After learning about the report, more physicians see opportunities for professional re-integration than before. The medical advisers and their team must be strengthened and receive a clear role in order to empower them.
Keywords
Introduction
In this article, the term “medical adviser(s) (MA(s))” is also used to refer to insurance physicians.
The Belgian context
The proportion of people claiming incapacity benefits has risen in several OECD (Organisation for Economic Co-operation and Development) countries. For many years now there has been an annual increase in the number of people in Belgium who have been incapacitated for work for more than one year, and the number has now passed 470.000 out of a total population of 11.5 million [1]. Moreover, expenditure on incapacity benefits has recently surpassed the total amount spent on unemployment benefits [2].
Work capacity evaluation for employees in the private sector is based on the article 100§1 1 of the Law on compulsory health insurance and benefits, which includes a provision that a person is unfit for work if he or she has lost at least two-thirds of his or her earning capacity [3].
In 2019 there were 220.25 full-time equivalent (FTE) medical advisers (MAs) in Belgium of which approximately 45% are French-speaking. They are responsible for workers working in the private sector and for self-employed. Each citizen in Belgium is member of one of the 7 non-profit mutual health insurance companies (MHICs). The 220.25 FTE MA are distributed among the 6 main MHIC. The 7th MHIC is dedicated for railways public agents. The primary task of MHICs and their MAs in relation to work incapacity is to check whether their insured persons actually meet the criteria set out in the law defining work incapacity, so that they can receive income-replacement benefits. MAs are also required to monitor occupational reintegration and initiate return-to-work programmes where applicable [3, 4]. Since 2016, MAs are also requested to give to the insured person one of the four categories 2 regarding socio-professional reintegration as defined in the legislation no later than two months after the beginning of the work incapacity[4]. If category 1 is not possible at that moment, category 4 is the one that opens up the possibility of returning to work.
The MA is always legally responsible for all decisions made even though some MHICs have other health care professionals (OHPs) such as occupational therapists, nurses or physiotherapists working in the same practice as the MA. Workers from the public sector are evaluated by dedicated institutions that have specific rules and MAs.
Looking beyond work capacity evaluation to include the wider issue of vocational rehabilitation, there is considerable fragmentation in Belgium between the various stakeholders involved, resulting in little scope for early intervention. Belgium has one of the most developed structures for rehabilitation and return to work in Europe, but the level of coordination is still limited [5, 6].
Basis of evaluations and their reliability
Few countries have made recommendations on good practice and, more importantly, require compliance with them in regard to work capacity evaluation [7]. In many cases, MAs have to find solutions quickly, basing their decisions on a combination of prior training and experience, intuition and opportunity. This creates a lack of transparency, standardization and quality in the evaluation process and a low level of reproducibility [7–12]. Their decisions are often made on the basis of the insured person’s medical condition rather than his or her functional capacity. Yet, a diagnostic process alone does not establish many links with the person’s functional status [9, 10]. There is not always a correlation between limitations with a medical cause and fitness for work. For some diseases, the fact that a particular medical condition results in a particular form of incapacity may lead to a low level of consensus. The same problem arises in regard to the severity of the incapacity or the type of support required as a result of a limitation with a medical cause [7, 14].
Variability between individuals carrying out medical evaluations can be explained both by variability in the interaction between the expert and the person being evaluated, and by variability between the experts themselves. A systematic review has shown a very clear correlation between the level of standardization in the evaluation and inter-rater reliability (p-value=0.006) [7]. The absence of a gold standard is a perennial problem in the assessment of limitations at work. Collecting the same data with a higher level of standardisation will enhance inter-rater reliability [15].
Towards good practice
Currently, work capacity evaluation is usually based on a biomedical perspective, often taking a disease or injury as a reference point and not considering the possible influence of contextual factors [6, 17]. There is a willingness in Belgium and a need to move towards a more biopsychosocial model that also includes personal and environmental factors [6]. Although the ability to work is related to a state of health, it is not a direct consequence of the individual’s health, but more the result of the interaction between his or her state of health and contextual factors (environmental and personal) [18–20]. It is important to consider the person’s interaction with his or her working environment, as environmental factors can play an important part in improving participation in work [8, 22]. Building on this concept, incapacity for work is not a characteristic specific to the individual [23]. MAs are recommended to request detailed information during the insured person’s evaluation about the limitations that affect his or her participation and also about his or her activities, as well as gathering medical information [15]. There is growing evidence that psychosocial factors influence the actual experience of incapacity and the biopsychosocial model, which became prominent during the early 2000 s, is now commonly used in Europe [24–26]. Specifically with regard to low back pain, it is now widely recognized that it is a complex biopsychosocial phenomenon and not just a pathophysiological process, and that causation is not always easy to establish. It is recommended that a biopsychosocial model be used to guide the management and evaluation of this condition, taking into account the combination of behavioural, psychological and social factors and the likelihood of pain and disability persisting in future, particularly if the pain has become chronic [18, 27–30].
Key stakeholders, such as rehabilitation services and managers in the workplace, need to coordinate their efforts and should not only share medical information but also information on contextual variables such as aspects relating to occupational retraining, functional, psychosocial, environmental, educational aspects, etc. to ensure that the rehabilitation process is appropriate and that an individual reintegration plan (possibly with an adapted and/or gradual return to work) is in place. A multidisciplinary approach is an integral part of a vocational rehabilitation programme and has been identified as a key criterion in determining its success [24, 31–35].
The evaluation of functional capacity is part of vocational rehabilitation and is a central aspect of the assessment of work incapacity. This evaluation provides essential information on the relationship between impairments and functional limitations. The relationship between the individual’s medical condition and his or her functional capacity must be made explicit [11, 25]. Addressing functional limitations may be of first order importance in enabling employment for clients having musculoskeletal conditions [36]. Despite the fact that consensus on a definition is difficult to come by, the following definition of a functional capacity evaluation (FCE) is often cited nowadays: an FCE is “an evaluation of capacity of activities that is used to make recommendations on participation in work while considering the person’s body functions and structures, environmental factors, personal factors and health status” [37]. This approach is used in occupational insurance and rehabilitation medicine to assess fitness for work [38]. An evaluation in an environment that is as close as possible to the person’s own is preferred but this is not always easy to achieve. It is not always possible in an evaluation to simulate the real working environment or psychosocial factors. In this approach, an understanding of the environmental factors (e.g. client/patient relationships, employer attitude, etc.) is vital [8, 21]. A recent study showed that biopsychosocial factors were associated with every FCE results. Specifically, social factors showed a consistent association with FCE performances [39]. MAs and their team are not required to carry out an FCE in Belgium.
The International Classification of Functioning, Disability and Health (ICF)
The ICF is a model and a classification developed by the WHO (World Health Organisation) that provides a conceptual framework for health and disability. Its structure reflects a biopsychosocial approach to describe health and disability and includes environmental factors. The model also includes personal factors but these were not listed when creating the ICF [40]. The ICF model takes into account the dynamic interactions between multiple biopsychosocial factors and provides a generic framework with a common language for describing a person’s level of function in relation to a health condition, thereby promoting standardization (e.g. of reports on work disability) [10, 40–45]. However the ICF contains only a limited number of categories related to the workplace and therefore indicates that its implementation in the field of work and health might be hindered [46].
The ICF can be used to guide case management, since it provides concepts and definitions that can be useful in improving the quality of assessments for incapacity benefits, particularly in countries where medical examiners do not describe functional capacity in a structured way [11, 25].
Despite the fact that the ICF does not provide any list of items relating to personal factors, taking into account personal factors such as the individual’s career path or motivation is vital for the transparency of the evaluation, as is the insured person’s personal experience. These can be freely evaluated and described. Collection of this data is relevant when planning and personalising evaluations and interventions, especially since these factors play a part in causing the person’s disability [16, 47]. Heerkens et al. developed a list of contextual factors, consisting of a list of work-related environmental factors and a list of personal factors. Social support at work is an important work-related factor. Both personal and environmental factors can have a positive or a negative influence on health and employability [46].
Core sets are available that consist of a group of items intended for use in everyday practice for a specific disease or situation (e.g. vocational rehabilitation). The core sets facilitate the practical implementation of the ICF. They make it possible to determine what should be assessed but they do not indicate how it should be assessed [9, 32]. The core sets simplify the process of performing multidisciplinary evaluations by clarifying the skills and responsibilities of each professional, and they can also be useful for insurers planning case management processes [18, 44].
Talo mentions that every reduction of ICF categories runs the risk of ignoring the whole range of the individual situation [49]. But as the number of categories increases, the efficacy ratio of each item falls [10]. It seems important to identify the items that are relevant and need to be taken into account when evaluating work capacity and opportunities for returning to work with specific groups of conditions. As an example it is known that many clients are experiencing depression from the chronic pain due to the initial injury and resulting disability [50]. It is important that the selected items can also capture this kind of disorder.
Purpose of the study
The study focused mainly on the perceptions of MAs and other healthcare professionals (OHPs) in Belgium regarding the use of ICF core sets when assessing primary work incapacity (<1 year on sick leave) related to back pain. The first purpose of the study was to investigate the perceptions of MAs and OHPs on the value of having access to an ICF-based assessment that contains biopsychosocial information, as an additional tool to support decision-making. The focus was only on the French-speaking MAs and OHPs responsible for workers working in the private sector and as self-employed. In this article, the term “other healthcare professionals (OHPs)” is used to refer to occupational therapists, nurses or physiotherapists who work alongside MAs. The following research question guided the study “What are the perceptions of medical advisers on the use of ICF core-sets for evaluating work incapacity related to back pain in French-speaking Belgium?”. Ancillary research questions have also been asked and guided the study: Does an ICF-based biopsychosocial report change the decision of the MAs on work incapacity? Does an ICF-based biopsychosocial report change the perspective on returning to work? Do the age and years of experience of the respondents have an impact on the responses to the perception questionnaire? In what form does multidisciplinary take place if it exists within the MA practice?
The main hypothesis is that such a biopsychosocial report will be an added value for the MAs and OHPs especially in this period of time when they are relatively few for a very large number of clients.
It was also hypothesised that an ICF-based report will have an impact on the recognition of work incapacity and that the report will have a positive impact on the perspectives to return to work. There were no strong hypotheses about the impact of years of age and years of experience.
Materials and methods
The methodology consisted of two phases: 1) creating a clinical vignette based on a video-recorded consultation (the vignette was made up of two videos with subtitles), and 2) presenting the clinical vignette to a sample (N = 101) of French-speaking MAs and OHPs so that they could complete a questionnaire on their perceptions of the added value of having more biopsychosocial-type information when making decisions.
Phase 1: Creation of a clinical vignette consisting of a medical examination and a biopsychosocial assessment based on the ICF
First, four pre-selected people insured within two Belgian mutual health insurance companies (MHICs) were met. Informed consent was obtained from all of them. The inclusion criteria were: 1) being a member of one of the 6 MHICs, 2) being recognised on work incapacity by a physician, 3) being between 18 and 64 years of age, 4) being identified by one of the following ICD-10 codes or similar pathologies if no ICD-10 codes were provided on the medical certificate: M40 to M48, M50, M51, M53, M54. The exclusion criteria were: 1) suffering from a pathology other than back pain (or its possible co-morbidities) which is the main reason for the work incapacity, 2) receiving immediately prior to their incapacity for work unemployment insurance benefits, 3) not being able to speak French, Dutch or English to a sufficient level.
First of all, an occupational therapist (the first author of this article) passively attended the standard medical examination performed by the MA (duration: 15 minutes). The occupational therapist then interviewed the insured for one hour and fifteen minutes to discuss the various items in the selected core sets. Two core sets provided and validated by the ICF Research Branch were used with their comprehensive version: “Vocational Rehabilitation Comprehensive” and “Low Back Pain Comprehensive”. The comprehensive versions reflect all the commonest problems that a person may encounter in relation to a specific disease or context [18]. The “Generic Set” and the “Rehabilitation Set” were also used as well as the core set created and validated by the European Union of Medicine in Assurance and Social Security (EUMASS). Many items were included in more than one of the selected core sets. Combining these core sets and items should give an overall view of the insured person’s level of occupational functioning [16].
After the occupational therapist had attended the medical examination and then conducted the interview with the insured, a brief summary based on the ICF assessment describing the person’s level of functioning was written. On a practical note, the ICF was used as a checklist to provide an easily understandable written assessment for Phase 2. A number of personal factors were also addressed.
One clinical case out of the four that were included was selected and its corresponding ICF-based functional assessment for presentation to MAs and OHPs in the form of two videos. The selected clinical case was the only one that met all the criteria to be included for the study. The three other cases had one or more exclusion criteria. For ethical reason, the two videos of the selected clinical case cannot be shared. However, the case was validated by a panel of experts composed of insurance physicians, who met for a face validity session lasting approximately one hour. The case concerned a French-speaking female 31-year-old industrial cleaner in a hospital who was employed on a permanent contract. She had been unfit for work for less than six months. Her main diagnosis was “radicular pain”, “neck pain” or “neck and arm pain” according to the medical certificates received. This was the first time she had been called to see the MA. The following key factors can be added among others: has pain in her arms and elbows for years and now has pain in her shoulders, neck and back; no lesions detected in a recent scanner and MRI; consults a psychologist twice a month and takes antidepressants; stopped the physiotherapist’s sessions before having completed them all; hasn’t taken appointments to the rheumatologist nor the acupuncturist despite the recommendations from her physician; is in conflict with her hierarchy and some colleagues; lives in a couple with her teenage son; tries for one year and a half to get pregnant from her new partner and is waiting for a gynaecologic surgery; reports no financial difficulties. Full ICF-based report is available on request.
Phase 2: Case presentation and questionnaire distribution
The two videos presenting the clinical case were introduced on 19 February 2019 at a conference of the Association Scientifique de Médecine d’Assurance (ASMA – Scientific Association of Insurance Medicine) attended by the majority of French-speaking Belgian MAs as well as other insurance practitioners.
The first video showing the medical examination carried out by the MA was 15 minutes long. Recording blanks and the decision were edited out. The second video presented the ICF-based functional assessment (continuous text, not detailing every item), in the form of a 15-minute clip. Both of the videos shown were subtitled in French to facilitate assimilation of the information. Figure 1 illustrates the data collection process during Phase 2.

Timeline for data collection in Phase 2 of the practical part at the ASMA conference on 19 February 2019.
The resources needed to carry out the ICF assessment were explained at the beginning of the session. A brief presentation of the study and the ICF was given so that the respondents understood the context of the study.
Questions concerning recognition of work incapacity were asked after the first video (the medical examination) and then repeated after the second video (the ICF assessment). Following these presentations, a perception questionnaire was distributed to MAs and OHPs working alongside them, making use of the Turning Point® direct voting system to measure their perceptions of the value of having an ICF-based assessment as an additional decision-making tool for MAs. The questionnaire included 22 questions with four Likert scale-type response options. A few questions concerning demographics were asked at the end as well as questions related to the implementation of multidisciplinarity. After the session, free-form comments were also collected.
The data from the questionnaires was analysed using a quantitative method. A number of different statistical methods were used: descriptive (frequency), Cronbach’s alpha, Chi2, McNemar and regressions run with IBM SPSS® software: version 25 (Armonk, NY). Free-form comments were also analysed with a semi-qualitative method.
Sample
Of the 141 people present, a sample of 101 individuals (92 MAs and nine OHPs) was obtained. This sample is considered representative as it is known there are currently approximately 100 FTE French-speaking MAs in Belgium in charge of the private sector’s workers and of the self-employed. They were 7,9% under 35 years of age, 19,8% between 35 and 45 years of age, 25,7% between 46 and 55 years of age and 46,5% above 55 years of age. The over-55 age group was composed only of MAs. In terms of years of experience, half the respondents (50,5%) had more than eight years’ experience, 11,9% had between 5 and 8 years, 17,8 % between 2 and 4 years and another 17.8% had less than two years’ experience.
Results regarding recognition of work incapacity before and after presentation of the ICF assessment
Recognition of work incapacity
Before submitting the questionnaire, it was needed to know whether having access to an ICF assessment would change the respondents’ position with regard to whether or not the official recognition criteria apply to the patient (art. 100§1 of the law of 1994 [3]). It was therefore asked for their opinion on article 100§1 before presenting the ICF assessment (immediately after the presentation of the medical examination) and 79.6% of the respondents would not recognize the insured person for work incapacity. It was then asked the same question after presenting the ICF-based assessment and 82.8% would not recognise the insured person. The results were analysed using a McNemar test, and the difference was not significant.
Assignment of one of the four categories related to socio-professional reintegration
The participants were also asked to place the insured person from the clinical case in one of the four categories (cf. footnote in section 1.1 for definitions) as required under the legislation [4]. This question was asked before and after the presentation of the ICF-based assessment. A Pearson’s chi-squared analysis indicates that there is a significant difference (p-value<0.001) between the responses for the different categories.
The sample was then split in two groups for further analysis. The first group included all those who placed the insured in categories 1, 2 or 3, while the second represented those who placed the insured in category 4. It was assumed that those individuals who had changed their mind and placed the insured in category 4 after the presentation of the ICF assessment, having placed her in one of the other three categories before the presentation of the ICF assessment, were also those who were convinced that the ICF assessment had an added value. Cross-tabulation McNemar analysis were used. The results of this analysis are shown in Table 1. Among the MAs and OHPs, 61.96% placed the insured in category 4 before the presentation of the ICF assessment. This figure was 8.69 percentage points (pp) higher after the presentation, i.e. 70.65% (p-value: 0.077). After this, an analysis of the results was conducted based on two groups: those over or under 55 years of age. For the under-55 age group, 14 pp more respondents placed the insured in category 4 after presentation of the ICF assessment, thus rising from 60% to 74% (p-value: 0.039).
Proportion in “category 4” before and after presentation of the ICF assessment (per group)
Proportion in “category 4” before and after presentation of the ICF assessment (per group)
Next, although this was beyond the scope of the initial research question, an analysis was conducted on what proportion of all those who attended on that day changed to category 4 after presentation of the ICF assessment. In other words, as well as taking into account the opinion of the initial study sample as strictly defined (MAs and OHPs working with them), the opinion of the other conference participants was also taken into account, most of whom were insurance physicians who were also very familiar with the legislation. Of the 119 respondents, an additional 10.09 pp placed the insured in category 4 after presentation of the ICF assessment, a rise from 61.345% to 71.43% (p-value: 0.012).
The perception questionnaire consisting of 22 questions was structured around four dimensions that were determined by the authors: clinical and diagnostic relevance (CDR), management (M), communication (C) and role enhancement of the MA or other OHP (RE). The questions were asked in a random order. Two mirror questions were introduced to identify respondents with a boycott attitude. This resulted in the exclusion of three participants. Ultimately a sample of 98 individuals was retained (89 MAs and nine OHPs).
Table 2 shows the results for the 22 questions. Subsequently the mean of the scores for the four dimensions was calculated. The scores for the two mirror questions were converted prior to the calculation. A score of 2.5 indicates a neutral stance in terms of agreement/disagreement for the questions relating to each dimension because the response options ranged from 1 to 4. Less than 2.5 means a favourable opinion, while a mean score higher than 2.5 indicates an unfavourable opinion. Abstentions were not taken into account (weighting was based on votes cast).
Results of the perception questions (N min/max=90/98)
Results of the perception questions (N min/max=90/98)

*Adding together “Strongly agree” and “Agree” scores. **Range from 1 to 4; 1=“Strongly agree”, 2=“Agree”, 3=“Disagree”, 4=“Strongly disagree”; 2.5 = neutral score (neither agree nor disagree) ***Definition provided when the questionnaire was distributed: “Multidisciplinary working can be defined as the involvement of several disciplines on a single topic, to approach a subject from the perspectives of different specialists, bringing together a number of specialist areas in a complementary way to solve a problem, whereby each specialist continues to use his or her own specific concepts and methods”. ****The mean after converting the scores (can be compared with the mean of the corresponding mirror question).
There was a good to very good internal consistency across all four dimensions, with Cronbach’s alphas ranging from 0.69 to 0.83. A Cronbach’s alpha of 0.69 for the “management” dimension is relatively low, as 85.7% of the respondents disagreed with the statement in question M2 about time and resources received (cf. Table 2). After removing this question from the internal consistency calculation for dimension 2, Cronbach’s alpha was 0.78.
Figure 2 shows box plots representing the values observed for each of the four dimensions. The values for each question within a single dimension were aggregated to give a single score per respondent for each dimension. Missing values were replaced by the mean of the available values for the respondent within the same dimension. Significant variations were found in the responses, with most between 2 and 3. Extremes were seen in relation to disagreements for the “management”, “communication” and “role enhancement” dimensions.
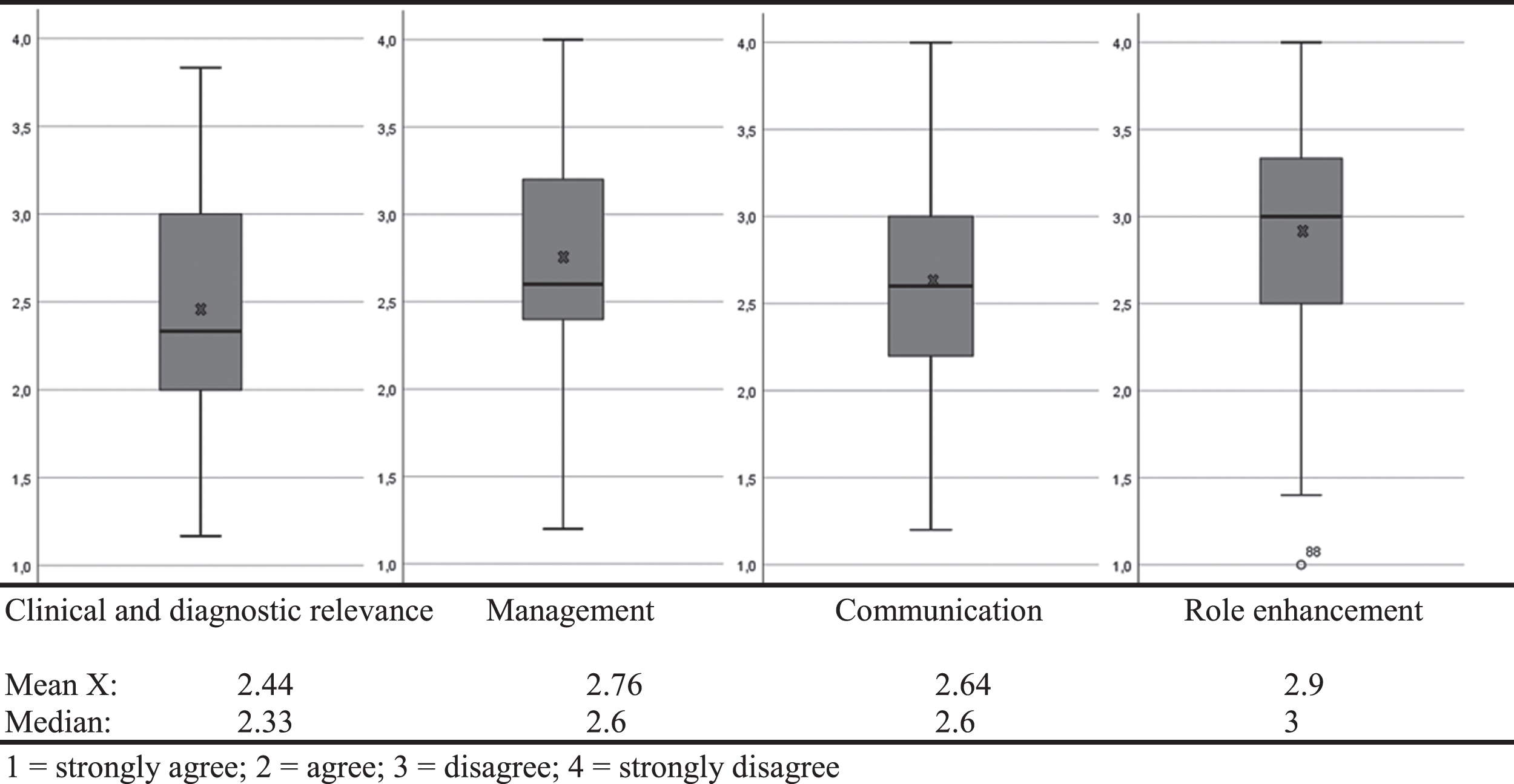
Box plots representing the values observed for the four dimensions (N = 98).
Only the
In the
In the
For the
Linear regressions were performed to analyse the impact of the respondents’ age and experience on their perceptions of the four dimensions that were analysed using the perception questionnaire (cf. Table 3). The normality of the distributions was tested beforehand and considered adequate.
Univariate regressions for age and years of experience for each of the four dimensions
Univariate regressions for age and years of experience for each of the four dimensions
The age of the respondents was classified into three categories: under 46 years of age (N = 28), 46–55 years of age (N = 26) and over 55 years of age (N = 47). In terms of experience, the respondents were divided into two groups: less than five years’ experience (N = 36) and more than five years’ experience (N = 63). For the “clinical and diagnostic relevance” dimension, the younger the respondent, the more he or she agrees, i.e. agrees that using the ICF is clinically and diagnostically relevant (p-value<0.05). Also for this dimension, respondents with less than five years’ experience agreed more than respondents with more than five years’ experience (p-value<0.05). For the other three dimensions, respondents over 55 years of age were clearly less favourable than younger respondents, although the difference was not significant. In other words, they are more likely to think that using the ICF will not have a favourable impact on their communication, on the enhancement of their role or on case management. Multivariate regressions were performed including both age groups and years of experience. Though the results were broadly similar to those presented above, the aforementioned differences ceased to be significant.
A total of 76.4% of the respondents reported having one or more OHP working in their practice within the MHIC. Of these, 55.88% stated that each discipline evaluates the insured person within its own field, and the MA then makes a decision based on the information from each discipline, 27.47% said that OHPs carry out evaluations in place of the MA, who does not necessarily see the insured. Only 55.88% indicated that meetings take place to discuss specific cases.
Results relating to the need for more information
The last question asked was “Would you have liked to have had more information about the insured persons’ situation at the end of the presentation of the medical examination?” (the first video). Half of the respondents (49.5%) would have liked to have had more information and 80% of them felt that the ICF assessment remedied all or part of this lack of information.
Free-form comments
The participants had the opportunity to make free-form comments anonymously at the end of the session, and 48 of them did so. Twenty individuals (41.67%) mentioned in their comments that there was insufficient time and/or resources in their organisation to carry out an evaluation as proposed in the study. Eighteen individuals (37.5%) stated that the ICF assessment is useful to some extent, while six people (12.5%) said that the ICF was not useful or its input was not significant. Several of the latter group mentioned that the evaluation was too subjective, since it is based mainly on statements made by the insured, or that it was more the time available to the occupational therapist that made the difference compared with the medical examination by the MA, rather than the ICF itself. Three individuals said that an abridged version would perhaps be more appropriate. Seven comments addressed the cost/benefit issue. Some of these mentioned that the ICF assessment as presented took up a lot of time but ultimately provided only a small amount of extra information and that the additional information obtained would not have altered their decision. Finally, six respondents indicated in their comments that they were rather in favour of multidisciplinary working for the work capacity evaluation and suggested that the ICF assessment could be useful in this respect.
Discussion
Recognition of work incapacity
Both before and after the presentation of the ICF assessment, one in five respondents would not recognise the insured as being unfit for work while it was actually the case. So there was a difference of opinion among the respondents. This finding is in line with the literature review in the introduction section, which highlights a low level of inter-rater reliability for chronic low back pain. The results, which related to chronic back pain and not specifically to low back pain were extrapolated here. Also a recent study concluded that from the client’s perspective, the official decision about sickness benefits was considered unrelated to the results from the previous work ability evaluation, lacking solid arguments and sometimes contradictory to the recommendations of other stakeholders [51].
That there was no significant difference before and after distribution of the ICF assessment is contrary to the literature, which states that when patients provide additional information about participation restrictions and the activity limitations on their activities, they are given a higher incapacity score. This finding doesn’t support the hypothesis that an ICF-based report would have an impact on the recognition of work incapacity. These results should, however, be interpreted with caution, since a number of possible forms of bias were identified. Firstly, the respondents saw the results displayed immediately after the vote (unlike in the case of the 22 perception questions), so there was probably a non-confrontation bias and a “group effect” following the disclosure of the results immediately after the vote. Finally, it is possible that the law [3] (cf. footnote in section 1.1) is not sufficiently flexible to allow biopsychosocial aspects specific to the clinical case presented to be taken into account while complying with the legislation.
Assignment of one of the four categories related to socio-professional reintegration
The respondents were asked to place the insured in one of the four categories (cf. footnote in section 1.1 for definitions) set out in the legislation [4], taking the position that respondents who changed from category 1, 2 or 3 to category 4 after presentation of the ICF assessment had seen an added value of the ICF assessment. Category 4 establishes the possibility of returning to work. The before/after difference was significantly in favour of the ICF, except for the group of MAs over 55 years of age. The significance is even greater when the sample is extended to include all the respondents who attended that day, i.e. most of the insurance physicians who are not MAs for Belgian MHICs. This reinforces the view that an ICF assessment is useful in facilitating a return-to-work process and supports the hypothesis that such a biopsychosocial report would have a positive impact on the perspectives to return to work.
A recent study showed evidence that psychosocial factors contribute to work-related musculoskeletal disorders symptom intensification, including an increase in pain intensity and severity [52]. Another recent study about chronic pain and contextual factors showed that according to the clients’ view both environmental and personal factors play a role in achieving a rehabilitation programme [53]. These factors are part of contextual factors in the ICF model. This is all the more interesting since it is known that a return to work can sometimes take place before symptoms have disappeared and that functional capacity may improve despite the persistence of symptoms such as pain.
It seems quite clear that the ICF is useful, but that measures are needed to facilitate appropriate case management and communication. One explanation for the fact that the MAs over the age of 55 were not convinced may be that the obligation to initiate a return-to-work process, which came into force in late 2016, has brought about more of a change in practices for older MAs, because they were used to working according to a “fit for work/unfit for work” approach, whereas the current legislation encourages more nuanced approaches.
The perception questionnaire
A number of comments left by the respondents indicate that the information provided by the ICF is in fact useful and represents the basis of what an evaluation should or ought to include. One respondent stated that, in the past, evaluations took more into account the aspects included in the ICF assessment. For some respondents, it is therefore not so much the ICF assessment that provides comprehensive information, but rather the time that the occupational therapist had available to carry out an assessment of this kind.
In regard to the
As regards the
On the
Philosophy of multidisciplinary working
Among the respondents who work in a MA’s practice that includes OHPs, it is surprising to find that only just over half of them are working in a truly multidisciplinary setting. In other words, a situation where the MA makes decisions based on information from each discipline, possibly with meetings between the various disciplines. This is despite the fact that the literature advocates a truly multidisciplinary approach. This is even more striking given that more than one in four respondents stated that OHPs working in their MHIC carry out evaluations in the place of the MA, so that the latter does not necessarily see the insured person although he or she is responsible by law for the final decision.
Several of the comments that were collected reflect a certain fear of the idea that MAs could be required to carry out the ICF assessment, even though they already have insufficient time, or that their role as a MA will be replaced by an OHP. However, the process of carrying out this assessment in a true multidisciplinary working context was explained in the first part of the presentation, specifying that the study was part of a process to improve complementarity between the roles of the MA and the occupational therapist or any OHP.
The results of the perception questionnaire as well as the additional questions asked tend to support the main hypothesis which was assumed that a biopsychosocial report would be an added value for the MAs and OHPs. It is noted that this added value is to be relativized according to the dimensions evaluated and according to the age and experience of the respondents. The free comments collected provide a better understanding of the results. The time available for MAs and OHPs seems to be a very important element of understanding.
Limitations and further research
Although this study is original and has brought new elements, there were limitations that need to be addressed in future research. The first limitation is that the opinion of the MAs took place on the basis of a single clinical vignette. The sample of MAs was large and representative, but it was not possible to collect their opinion for several clinical cases. It would be interesting to carry out other studies considering more clinical cases. Another limitation is that it was not possible to assess the client in a truly multidisciplinary setting. In this study only a MA and an occupational therapist were involved in the evaluation and there was no discussion between the occupational therapist and the MA at the end of the assessment. Studies involving other OHPs around the MA could be of interest for the Belgian context.
The collection of data for each selected ICF item was based on an interview with the client. There is a need to use proven and validated methods for collecting and assessing data for the evaluation of each ICF item. Evaluation instruments designed to allow direct association with the ICF categories are essential to operationalize it [54].
Finally and in relation with what has just been said, it appears that carrying out an FCE assessment for this client would probably have been very interesting. For practical and ethical reasons the occupational therapist did not examine the insured either in the context of a consultation or in her own environment (work, home, etc.). Research should be carried out to assess the impact of offering such an evaluation in the Belgian context of work disability insurance. FCE does seem to be necessary in some cases and could provide a tool to support MAs in decision-making. It will also allow MAs or OHPs to rely on extra elements than on the insured person’s statements. Carrying out such an FCE is also in line of collecting biopsychosocial factors as the latter are associated with performance on FCE [39]. Carrying an FCE based only on ICF items is not possible at the moment. It is needed to link further instruments measuring work functioning to the ICF. In order to do so, it is essential to know what aspect of work functioning needs to be measured in a certain setting [49]. To ensure correct decisions and efforts in clients’ case it is essential that these are based on valid results representative of the client functions at work [51]. Further research should focus on identifying the extent to which ICF and the development of it done so far can be helpful in performing FCEs.
Recommendations for the Belgian context
The use of a biopsychosocial based evaluation would be appropriate to guide the first appointment done by the MA and/or the OHP. The ICF can provide a biopsychosocial framework, with core sets that allow only the items relevant to a specific disease or situation to be considered such as the vocational rehabilitation core set. It may be useful to reduce the number of items that must be considered. This will make it possible to strike a balance between the number of items that need to be assessed in order to have a sufficiently comprehensive evaluation, and the resources that are available for evaluations carried out by MHICs. However this selection should be done carefully as participation in the life area of work and employment has to be understood as interdependent with the ability to participate in other areas of life.
In view of the results discussed above and according to the literature review, it would seem to be appropriate to introduce true multidisciplinary working within Belgian MHICs by identifying which professionals are actually needed and by defining their roles and the occasions when they should intervene. This should be done on a scientific basis and in accordance with the law. In the Swedish sickness insurance system, the professionals that can be involved in the clients’ evaluation are physicians, occupational therapists, physiotherapists and psychologists [51]. It will make it possible to reduce the workload of MAs and enable insured persons to have a more comprehensive evaluation.
For specific clients yet to be determined, carrying out FCEs would be of interest to go deeper in the evaluation.
Bridges between the health care sector, the MHIC services and other actors currently involved in the return to work should be further developed. The health care sector in Belgium should have a greater role in the return to work. The use of disability managers 3 could be useful for coordinating the various stakeholders mentioned above and making optimum use of their contribution.
All of these recommendations cannot be implemented without the necessary reforms and means.
Conclusions
This study provides information on the perceptions of Belgian French-speaking medical advisers (MA) and other health care professionals (OHP) working alongside them regarding the use of ICF core sets when evaluating work incapacity due to back pain in Belgium. Although the methodology for the practical part does have a number of limitations, a framework that is more innovative than the one currently being used by mutual health insurance companies (MHIC) was nonetheless provided. It has been shown that MAs and OHPs working with them who are under 55 years of age consider it appropriate to take biopsychosocial information into account during the evaluation, that this plays a positive role in occupational reintegration and has highlighted perspectives that had not been identified before the presentation of the ICF assessment to the sample of MAs and OHPs. By using a larger sample of insurance physicians (n = 119), there is an even more significant increase of physicians who have seen opportunities for occupational reintegration after learning of the report than before. The use of a biopsychosocial model like the one presented here to drive the assessment provided a more comprehensive understanding of the biopsychosocial situation for a specific clinical case. A biopsychosocial tool to support decision-making in Belgian MHICs will provide benefits both clinically and diagnostically, and should therefore improve the quality of evaluations of insured persons and thus promote their return to work. The context in which the ICF was used in the study, however, does not allow a practical response to the concerns of the participants, nor to the challenges associated with evaluating work incapacity and providing support in Belgium. Those identified challenges include the time required for the evaluation, the various individuals involved in using it – which means having a multidisciplinary team in which each person has a clear role – and effective coordination. Addressing these challenges will improve communication between the various individuals involved and thereby improve case management. The MAs and their team must be strengthened and receive a clear role in order to empower them.
A revision of the Belgian legislation, which is currently biomedical oriented, and addressing the above challenges seem to be essential.
It could be of interest for further research to investigate the current findings with multiple and various types of clinical cases as well as in different multidisciplinary settings for the evaluation.
Ethics statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the Ethics Committee “Comité d’Éthique Hospitalo-Facultaire Saint-Luc” of UCLouvain University on 22 January 2019 under reference number 2018-14NOV-432.
Informed consent
Informed consent was obtained from all patients to be included in the study.
Conflict of interest
To conduct this study partly during working hours as a civil servant in the employ of the Belgian National Institute for Health and Disability Benefits (NIHDI). He had a dual role in conducting the study: as a Public Health Sciences student at UCLouvain University and as an employee of NIHDI. SD and WG worked on the study during working hours paid by the NIHDI. CD declares that he has no conflict of interest.
Funding
None to report.
Availability of data
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgment
The authors have no acknowledgments.
Is recognized unable to work, the worker who has ceased all activity as a direct result of the onset or worsening of injuries or functional disorders which are known to lead to a reduction in earning capacity, at a rate equal to or less than a third of what a person of the same condition and the same training can earn through their work in the group of occupations in which the professional activity carried out by the person concerned when he/she became unable to work or in the various professions he/she could have exercised as a result of his professional training. [free translation]
Categories described in the Royal Decree of December 2016: Category 1: it can be reasonably assumed that the individual will be able to return to work spontaneously as per their contract, no later than the end of the sixth month of work incapacity; Category 2: a return to work does not seem possible for medical reasons; Category 3: a return to work is currently not appropriate because priority must be given to medical diagnosis or medical treatment;
“The disability manager characteristically focuses on coordination: a central person (job coach, medical adviser, company doctor, etc.) brings together the other parties involved and supports them in their various tasks related to maintaining the employment of individuals at risk of losing their jobs and getting people who are currently unfit for work back into the workplace. This methodology is based on the premise that the workplace is the most effective place for occupational reintegration” [free translation] [55]. INAMI-RIZIV. De Cock J. Disability Management - De la formation à la certification (brochure). 2017 p. 20. [consulté le 06/05/2019]. Disponible à l’adresse: ![]() .
.