
Abstract
BACKGROUND:
Important qualitative findings have accumulated on return to work after cancer from the perspective of various stakeholders.
OBJECTIVE:
The aim of this paper was to critically appraise the evidence produced between 2008–2017 on several key stages of the return to work process against the key stakeholders identified in the articles included.
METHODS:
A systematic search was done on four databases to identify relevant papers. Papers were selected based on pre-defined selection criteria. A qualitative evidence synthesis was performed on the articles included.
RESULTS:
A total of 57 articles were included in the analysis. Using the secondary thematic analysis, this study identified three categories of articles relative to the stakeholders included: articles focusing on patients’ experience (n = 41); articles dealing with multiple stakeholders, including patients (n = 12); and articles drawing on stakeholders other than patients (n = 4). The analysis also revealed five key stages of the return to work process which follow a sequential order and provide a comprehensive image of the process.
CONCLUSIONS:
More research is required on how employers view and are able to facilitate the return to work process after cancer. New forms of support must be planned and delivered by health professionals for patients who return on the labour market. The five stages model proposed in this study can help employers and policymakers to plan and deliver tailored legislation and guidance for RTW facilitation. All stakeholders must be further trained to embrace the idea that return to work is a complex process which continues long after the survivor returns to work.
Introduction
More than 19 million people were diagnosed with cancer worldwide in the last year and a considerable part of them are working-age patients [1, 2]. With improvements in screening, diagnosis and treatment, the number of survivors is increasing [3]. A growing number of the working-age survivors are able and wish to return to work (RTW) after treatment, as work provides financial security [4], a sense of normalcy and purpose [5] and an improved quality of life [6]. Although beneficial for both the survivor and the society, returning to work is a process marked with difficulties and barriers [7–11]. RTW is a process sensitive to contextual factors such as the specific of the national RTW policies, labour market features or the work environment [12]. Thus, RTW rates can vary significantly in different countries or regions [13] as well as the facilitator factors or the barriers influencing this process. This research reports findings from studies carried out worldwide thus bringing valuable support for comparing how RTW can vary depending on the context.
A bulk of quantitative and qualitative research has accumulated in the last decades on return to work after cancer emphasizing the complexity of the process [5]. This complexity pertains to multiple influencing variables, such as the socio-demographic characteristics of the patients [14], the type and stage of cancer, the physical and psycho-social effects of treatment [8], the duration of the sickness absence [15], the type of work [16], the work environment [17, 18], or the work accommodations provided [19]. A way to address the complexity of the RTW process is to understand it as a continuum of phases which can be approached step by step. Several existing papers describe this process as a dynamic and staged one [20, 21] or as a continuous communicative trajectory which is phased [22]. Such structuring of this complex process can be helpful for cancer survivors if they can understand and experience it as a sequence of stages, thus reducing the feeling of being overwhelmed when taking the decision to return to work [23], or when assessing their work readiness [24]. The structuring of the RTW process in successive stages can be helpful also for employers and health professionals which have a pivotal role in supporting workers with cancer to return to work, as they also perceive this process as being complex and intangible [25, 26]. Finally, this representation of the RTW process can help policymakers and employers to provide better legislation and guidance at company and individual level [21].
The multiple stakeholders involved in the RTW process is an additional factor underlining its complexity [27]: the survivor, the employer, the health professionals, the family, as well as other actors within community or at the government level. Reasonable enough, studies so far paid attention mostly to survivors. Considerably less articles reported findings on how the health providers (oncologists, occupational physicians, general practitioners, insurance physicians, psychologists and social workers [8, 28–30]) understand and involve in the RTW process. Much fewer papers explore the employers’ perspectives on the process, or other stakeholders like family or community actors [25, 31–33]. By showing the discrepancy in how the role of various stakeholders was analysed in the existing evidence, this review can orient future studies on return to work of cancer survivors. Equally important is to show within each category of stakeholders what topics are more intensely debated and what topics are missing from the current scientific discourse. RTW can be successful if all actors involved contribute to the process, thus it is important to highlight what contribution each stakeholder can bring.
The aim of the present paper is twofold: first, to critically appraise the qualitative evidence produced during 2008–2017 on RTW after cancer, in a comparative way, against the key stakeholders identified in the articles included, for the reasons presented above; second, based on previous papers mentioned above, to identify the key stages of the RTW process as they appear in the papers included in the review, and to present the results in a structured way, against these key stages. Thus, the goal of the paper is twofold: first, to emphasize which stakeholders are central in the current RTW literature and to show for which stakeholders more studies need to be produced and second, to highlight the RTW process as a continuum of stages and to show for which stage there is not enough evidence so far.
The focus of this review is on qualitative research as currently no studies have gathered data from qualitative studies that have examined the main categories of stakeholders or the stages of RTW process. Examining qualitative studies in addition to the reviews on quantitative studies that exist can bring more nuanced perspectives on this topic.
Methods
The present study is a qualitative evidence synthesis, which is a suitable method for exploring various perspectives [34] and a ‘more inclusive form of review’ [35].
Search protocol and data sources
Noyes and colleagues [36] emphasized the difficulties in systematically retrieving qualitative studies, either because of the various uses of the term ‘qualitative’ in the primary studies, or because of the limited value of the current strategies for indexing terms. There is also a current trend to consider a more holistic approach in searching the relevant articles, achieved through theoretical or purposive sampling [35, 37]. Therefore, a combined search strategy was used for this paper, for ensuring comprehensiveness.
First, PubMed, Web of Science, Google Scholar and Scopus databases were systematically searched to identify English qualitative studies, in peer-reviewed journals, published between 2008-2017. The search terms used were: ‘cancer’ OR ‘neoplasm’; ‘work’ OR ‘employment’; ‘return to work’, ‘qualitative’. The studies were included based on the following inclusion criteria: a. at least one goal of the study or research question or emerging theme focused explicitly on at least one component of the process of RTW; b. the study employed a qualitative research method (interview, focus-group, written narratives, ethnographic observations or a mixed approach); c. the study referred to at least one relevant stakeholder of the RTW process. Second, hand searches were performed in key journals in the field, as well as screening of the reference list of all the articles already included.
Articles found in the initial search were screened based on the title and abstract, then based on the full text. Studies were not excluded based on methodological quality in order not to discount important findings. Articles with mixed methods were included only if the qualitative data was discussed separately.
Data analysis
As a first step, data on authors, year, country, aim, type of stakeholders, type of cancer, emergent themes (based on the Results section of the articles) and methods were extracted from all the articles included in the review (Supplementary Table 1). Second, all the findings presented in the Results and Discussion sections of the articles were abstracted in detail, but only the results related to the aims of the paper were retained for the analysis. Thus, the focus was on critically and comparatively appraising only the results reported on (1) the stakeholders identified and (2) on key stages of the RTW process. A decision was taken to not include in the present review the findings on impact of cancer on work, meaning and benefits of work, drivers and barriers for RTW, and to focus on the actual RTW process. After summarising the data from Results and Discussion sections of the articles, we used the Discussion sections to finally decide what findings to keep and report further, as usually the Discussion section synthetizes the most important findings of a paper. The outcome of this step was a summarization of the findings based on two criteria, i.e., the stakeholder category and the RTW stage.
Third, thematic analysis was used for analysing the findings in the articles included in the review [35]. Being informed by an interpretive approach, the analysis was not limited to summarising the themes and findings reported in the included studies but determined overarching findings for every category of stakeholders and for every stage of the RTW process. The analysis was done using Nvivo 11.
As indicated by Sandelowski and Barroso [38], several steps were followed in this thematic analysis. The findings already summarized in the previous step were grouped according to their topical similarity. For example, all the findings related to ‘patients’ (as stakeholder category) and ‘disclosure’ (as stage of the RTW process) were put together, even if they refute each other. Finally, the findings in each category resulted were examined in order to eliminate redundancies and to formulate statements which comprehensively kept the significance while preserving the context in which they were formulated. The result of this process was a taxonomy of overarching findings in relation to the stakeholder category and the stage of the RTW process.
Results
The systematic search identified 2,533 articles, out of which 72 articles were retained for full text screening (Fig. 1), which resulted in 57 qualitative studies included in the review.
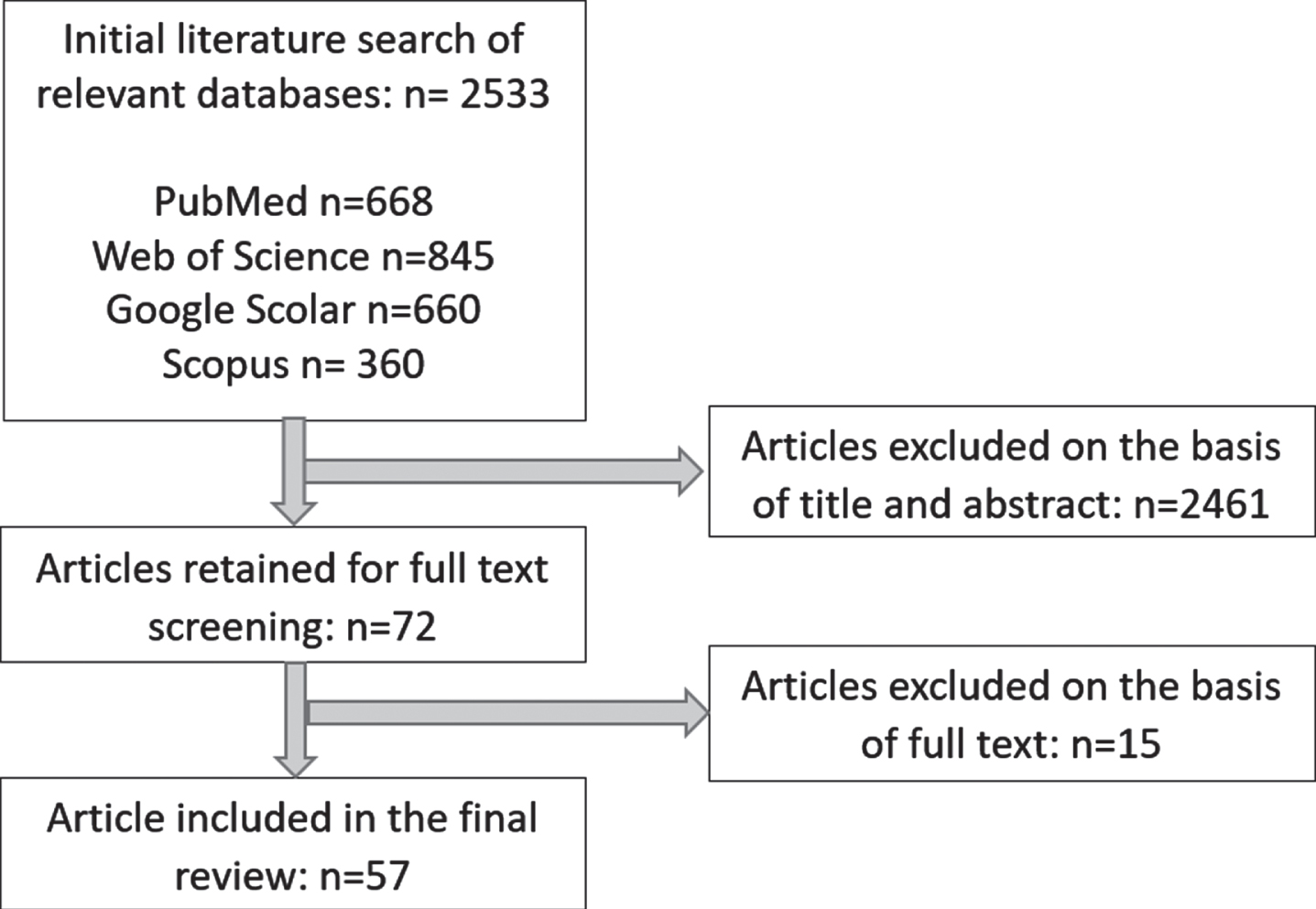
Flowchart of study selection.
Three main categories of stakeholders appear in these articles (Table 1). The predominant category (A) is represented by patients, as 41 articles were focused exclusively on patients as participants in the study. The second category (B) comprised 12 papers dealing with multiple stakeholders including patients. The third category (C) included four articles on stakeholders other than patients.
Categories of stakeholders in qualitative articles on return to work (2008–2017)
The analysis revealed five components of the RTW process which are most frequently presented as findings and examined in the articles included in the review: (1) disclosure, (2a) sickness absence and keeping in contact, (2b) continuation of work during treatment, (3) decision to go back to work and preparing the resuming of work, (4) support and advice received for RTW and (5) resuming work. These components can be understood as following a sequential order (Fig. 2). Hence, they can be considered as stages, although RTW can be different from one cancer survivor to another and in some cases the process is non-linear. The five stages depict a comprehensive image of the RTW process, from the initial phase of disclosure to the final steps of resuming work. The following section will be structured against the main categories of stakeholders and also on these five stages.
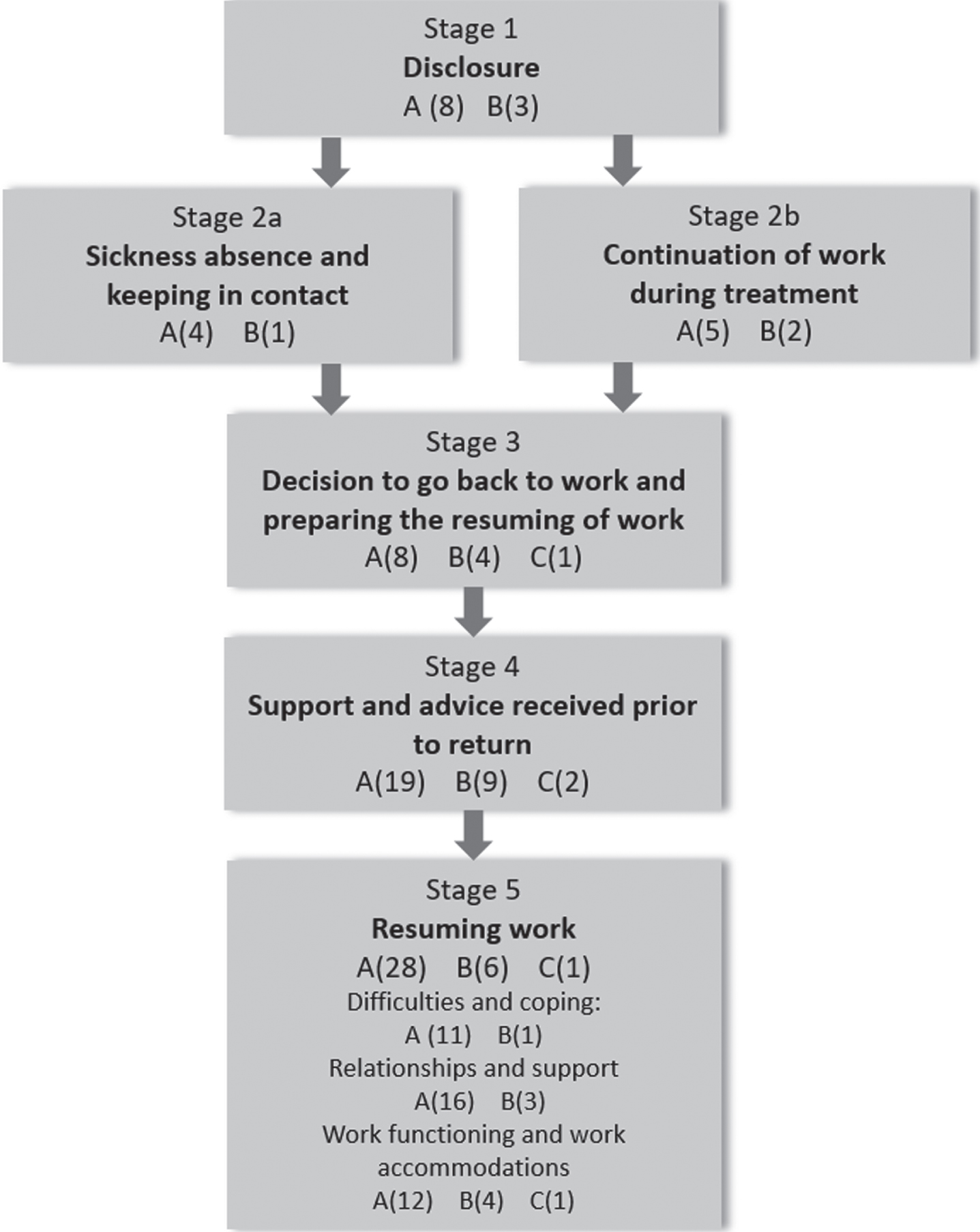
An integrative model on the key stages of the return to work process. Stage 1, 2,.., 5: The five sequential stages of the return to work process as they appear in the articles included in the review. A, B and C: the three categories in which articles included in the review can be classified depending on the type of stakeholder (A = articles dealing exclusively with patients; B = articles dealing with multiple stakeholders including patients; C = articles dealing other categories of stakeholders except patients). A/B/C (n): n is the number of articles in the category which focus on the respective stage.
Within category (A), 8 articles present findings on disclosure, underlining mainly three aspects. First, some articles emphasized the conditions and the limits of telling the diagnosis in the workplace, e.g. the influence of relationships at work [15] or being in a professional or managerial position at work [39]. Non-disclosure may also have benefits, by providing a ‘buffer’ allowing to avoid questions and concerns from colleagues and did not seem to negatively impact the success of RTW [39]. Second, special attention was given to the difficulty to disclose the diagnosis in the case of sensitive cancers, such as anal, prostate cancer or gynaecological cancers [40–42]. In this case, disclosure was either reduced or perceived as an ‘extra burden’. Third, 3 articles elaborated on the concerns and worries over the possible negative consequences of disclosure [43, 44].
Few articles in category (B) analyse disclosure. Two of them highlight the positive effects of disclosure and the negative consequences of non-disclosure [20, 45], while the third acknowledge that in order to be beneficial, disclosure should result from a collaborative effort of the survivor and the supervisor [24].
No articles in the category (C) deal with disclosure. Thus, compared to the considerable in-depth discussion on disclosure in the articles with patients as stakeholders, the much simpler analysis of this topic in the articles with multiple stakeholders indicates that disclosure is not an important topic for health professionals and employers.
Stage 2a. Sickness absence and keeping in contact
Here also there is more discussion on sickness absence and keeping in contact in the articles in category (A) than in the ones in (B), showing that this topic is probably significant for the patients. The variety of accounts in category (A) highlight how concerned are the patients regarding sick leave and keeping contact. The papers emphasize the patients’ attitudes towards sickness absence [43] or the impact of not having sick leave [46], as well as the importance of communicating with the workplace during sick leave [10].
In comparison, the single article in (B) discussing this topic reports the employers’ fear of generating negative reactions if they contact the employee during sick leave, which results in low frequency of keeping in contact [27]. The framing difference is obvious for patients versus health professionals and employers, as the first category speaks about communication and support, while the second about reasons to not be in contact with the employee.
Stage 2b. Continuation of work during treatment
In category (A) this topic was discussed in 5 articles, out of which 2 dealt with the continuation of work as the single option available for the patient, due to lack of access to paid leave [47], or financial and insurance reasons [44]. Another 2 articles reported that workplace support, work accommodations and fatigue were the factors facilitating in a great extent the continuation of work [48, 49]. One last article showed that the reduced schedule represented an administrative difficulty of continuing work [23].
While these articles highlight more the challenges of work continuation during treatment, the articles in category (B) emphasize the beneficial effects of continuing working during treatment with proper support from employers and family [45] and the factors enabling patients to work during treatment [50].
Stage 3. Decision to go back to work and preparing the resuming of work
Almost all articles in category (A) stress the complexity of the decision to RTW, either by presenting the main factors influencing this decision [23], or by focusing on specific factors, such as the treatment side-effects [46]. Generally, more weight is put on how the decision is taken and less on the actual preparation for RTW. Preparing for RTW seems to be a non-linear process, marked by mixed feelings and thoughts, and insufficient advice from health providers [51, 52]. Only 2 articles discuss the actual management of the RTW, i.e., planning and phasing the steps [53, 54].
Three articles elaborated on the decision to resume work in category (B). Participants (either patients, employers or health providers) agree that this decision belongs to the patient and should be coupled with the assessment of work capacity done by independent professionals [8, 55]. As in category (A), the studies in this category analysed the factors influencing this decision, with two factors being stressed as the most important: the timing of the decision [8] and the need to ground it both on the employee’s motivation to return and on the objective evaluation of the emotional, cognitive and physical readiness to return [55]. Again, similar with articles in category (A), in one study managers complained about the lack of guidance and inconsistent procedures for preparing RTW. All stakeholders in this study agree the survivor should have a contribution in preparing RTW, but the level of this contribution varied in their opinion [20].
In one article in category (C) employers explored their potential involvement in the RTW process [25]. Respondents acknowledged having concerns and dilemmas regarding the RTW process while trying to prioritise help and empathy towards the employee over performance and efficiency.
Stage 4. Support and advice received prior to return to work
This topic was the second most explored in the articles on patients (category A). A total of 19 articles deals with support from health providers, employer/colleagues and other types of support. Regarding the support received from health professionals, 7 articles highlight either the lack or the rudimentary support received by the patients from the oncologists. Other articles analyse the support from health professionals in general [57], the role of occupational physicians [49, 58], and the role of the disability insurer [39]. Many articles strongly advocated for the idea that the current guidance from health professionals is insufficient and should be improved.
The topic of support from employers and colleagues was even more present, as many articles discussed the pivotal role the employer and colleagues should have in supporting employees for RTW, and the support actually received [10, 59–61]. Two articles provided findings on the lack of support, or the random support received from the employer [53, 54], while others analysed the characteristics of the support, such as to be grounded on the employee preferences and to be honest and respectful [62, 63]. Overall, more articles report positively rather than negatively about the support and advice received by the patients. The third category, other type of support, comprised mainly the informational support needed and pointed towards the lack of information on statutory rights, working arrangements and employment contracts [27, 53]. Another article stressed the required support from close relatives [49].
As opposed to how this topic is represented by the patients in category (A), the articles in category (B) focus intensely on the support offered by health professionals (8 articles) and much less on the support from employers (1 article). This is explainable considering that category (B) includes articles in which participated mostly health professionals. Participants were satisfied with the support received from the employer in the initial stage of the sick leave but not so much after the recovery [27]. Patients and health professionals were unsatisfied with the lack of information on cognitive functioning of workers with cancer [28, 64]. Regarding the support from health professionals there is agreement that such interventions should involve all the key stakeholders (patient, physician and employer) and should agree on roles, responsibilities and timing of these interventions [65]. Health professionals expressed several requirements regarding support: to be multidisciplinary, to be part of the psychosocial care, to be customized to the patients’ needs [8], to be patient-led [24, 45] and to be based on the cooperation of the stakeholders [27]. A new category of specialists, the oncological occupational physicians, could be involved in addressing at least part of these needs [66].
This stage of the RTW process is approached also in 2 articles in category (C). Health professionals were convinced of the importance of RTW, but had little experience with the process [67]. Health professionals consider the RTW support as being not systematic, based on common sense rather than guidelines, and led by the patient. Moreover, they are not satisfied with the communication among professionals and how responsibilities are taken [26].
Stage 5. Resuming work
Resuming work is the most explored topic, as most of the articles in category (A) and (B) are providing an in-depth analysis of the patients’ experiences once they come back to work. The complexity and richness of the findings on this topic required organising the material in several sub-categories.
Difficulties and coping
The articles in category (A) summarise the difficulties encountered by the patients who resume work as physical and emotional vulnerability [44, 68–70], the gradual ‘wearing-off’ of understanding received from colleagues [9] and loss of cognitive function [56].
Two difficulties at work mentioned in the articles in the category (A) are also present in category (B): the wear-off effect of empathy and support and the cognitive limitations. In addition to how this topic is presented in articles in category (A), one difficulty reported here is the lack of follow-up of the patient after returning to work [11].
The patients’ experiences of coping at work relate either to individual strategies devised for active coping [47, 71] or for passive coping by silence [73], or by having no expectations at work [68]. Coping at work can also be gendered in the case of men who hide physical impairments from colleagues [40].
Relationships and support after returning
Articles in category (A) reveal that employees want to be accepted by colleagues and treated normally [68], yet relationships at work may be affected by the side effects of treatment and the type of cancer [46]. Except for the situation of not extending the employment contract after cancer [70], discrimination seems not to be an issue [23, 71].
In comparison, articles in category (B) reveal a contradictory view on discrimination and stigmatisation. Thus, workers consider cancer as a highly stigmatising condition, in opposition with the vocational service providers and employers who consider that employees with cancer are not likely to be stigmatised at work. Fear of discrimination is pervasive for survivors, leading to the decision of not disclosing the diagnosis [24].
Relationships at work can be objectified as support received from employers, colleagues and health professionals. Articles in category (A) show a balanced situation regarding receiving or not receiving support after returning to work, judging by the number of articles reporting the two alternatives. Thus, a form of support may be a greater flexibility of the employer or engaging the employee in new ways [41, 72]; support may be also informal or may be grounded on the a previous good relationships with the supervisor [42, 63]. The lack of support is usually experienced as lack of understanding or assessing the work performance without considering the impact of cancer [44, 73]. Having negative beliefs about the work capacity and the recovery time after cancer, providing support only when the disease is visible, as well as treating all employees with a “one-size-fits-all” approach are other forms of inadequate support [9, 74]. Still, the support from employer and colleagues is crucial in helping employees adjusting back at work and support from health professionals is deemed insufficient or considered to be of no great influence [10, 74].
The support offered at work after returning, as presented in articles in category (B), is not specifically targeted to decrease stigma and discrimination, but rather general psycho-social support which wore-off after some time [30, 45].
Work functioning and work accommodations
Participants reported limited work capacity which was impaired by cognitive deficits and emotional problems [44, 75]. The limited work capacity was perceived as particularly devastating for some type of professions, such as musicians [57]. Still, participants felt the expectation from the manager to function at the same level as before the diagnosis [53] or even to work harder in order to compensate for the deficit in work capacity [77].
The topic of work functioning is differently approached in the articles with multiple stakeholders (B), as opposed to the articles on patients (A). While in category (A) the focus was more on how the work functioning was changed by cancer, in category (B) the discussion is on barriers and facilitators of work functioning and how the co-workers’ and employers’ perceptions of the work ability and productivity of cancer survivors can be stigmatising [24, 45].
The article in category (C) relevant for this topic presents an informative discourse on work functioning, by giving voice to insurance physicians who report on the medical and non-medical factors most often used in the work disability assessment [78].
Despite the consensus that work accommodations are essential in RTW, several articles report negative situations: employees not asking for accommodations because they fear losing the job [68]; conditioning accommodations on the self-identification as ‘disabled’ which some patients refuse to do; not offering accommodations consistently in practice although they are advocated in policy [79]; an extra burden put on women who were also mothers and did not receive accommodation after returning to work after cancer [48]; Only 2 articles actually describe types of accommodations employed in specific cases, in two distinct categories: task-related and work environment related [71, 80].
The different perspectives of patients as opposed to employers and health professionals on work accommodations is obvious as many articles in category (A) described negative experiences of patients on this regard, while in category (B) there is a general agreement of employers and physicians on the necessity to provide work accommodations and five steps for an ‘ideal’ accommodation process are described [30].
Discussion
The analysis in this review derives interesting overarching findings relative to (1) the categories of stakeholders and (2) the stages in the RTW process, which can bring valuable information for the future research and practice in the field.
First, concerning the categories of stakeholders, most of the evidence produced so far is on patients (41 papers in category (A) out of 57 articles). Within the 12 papers with multiple stakeholders (category B), the situation is rather balanced, with slightly more interest on the views of health professionals than employers, as 7 articles deal with patients and health professionals and 5 articles draw on patients and employers. Similar, in the category of other stakeholders (C), 3 articles and 1 article present the views of health professionals and employers, respectively. Concluding, for researchers in the field understanding the perspectives of patients is most important, followed by the endeavour to obtain health professionals’ opinions. This probably illustrates the belief that patients and health providers have the most important role in RTW and the practice of involving and making accountant for the success of RTW mostly the patients and the health providers. Still, the limited existing literature on the role of employers [20, 27] stresses the crucial influence employers have on RTW. The ensuing implication for research is that more studies are required on the employers’ role in RTW facilitation.
Within articles focusing on patients two topics are central: support offered for RTW and the experience of resuming work. This reveals the patients’ need for support and the concerns they have in this area, as well as the richness of experience gained after getting back to work and the positive effects on identity and the welfare system. The employers’ support for RTW is described and discussed the most, followed by the health providers’ support. Another striking aspect is that almost all accounts related to health providers’ support for RTW are negative. As described by the patients, the support from health professionals is insufficient, almost always offered only if the patient asks for it and does not provide enough data to inform the decision to return or the choice of work accommodations. The implication for practice is that support must be continuously provided for cancer survivors by employers, physicians and nurses, considering that RTW is not a linear process, but rather a process marked by vulnerability [81]. Our study shows that despite all efforts and interventions done so far in different countries, the support from the health professionals for RTW is still an unmet need. New forms of support must be planned and delivered, considering the type of cancer, the patient’s characteristics, the type of work, but also the social and policy context. The alternative of not returning to work is leading in some cases to claiming welfare benefits which is stigmatising and is also increasing hardship on the welfare system [82].
Within articles with multiple stakeholders, more attention is given to the topic of support offered for RTW, which is similar with articles on patients, but less to what happens after resuming work. This probably indicates the implicit perception of health providers and employers that RTW process ends after the survivor has resumed work. Their efforts appear to be oriented towards the initial steps of RTW (disclosure, preparation) and less on the challenges encountered after returning to work. In addition, the ‘work accommodations’ topic is differently approached in the articles in category (A) versus (B). In the first case, more articles discussed the topic in more depth, while in the second case considerably less attention was given to this subject. The resulting practical implication is that health providers and employers must be trained to embrace the idea that the RTW process does not end when the survivor resumed work. Patients may face major challenges after returning to work which must be addressed using multidisciplinary interventions, by all stakeholders, instead of expecting that the survivor will simply adjust [83, 84]. Increasing the efforts to understand the survivor’s challenges after resuming work will improve long-term work reintegration which is a pressing need [3].
One critical finding of this review is the lack of discussion in category (C) on disclosure, preparing the RTW and resuming work, which indicates that these components of the RTW process are not as important for employers and health professionals as they are for patients. Thus, more research is needed on stakeholders other than patients to understand their views and potential involvement in the RTW process. More specific, there is critical need of studies on samples with no survivors, for collecting genuine opinions from doctors and employers.
Second, concerning the stages of the RTW process, the present study revealed five components of this process which can be envisaged as a chronological continuum, thus depicting a comprehensive and sequential development of the process. The results of this review show an unequal representation of these stages in the studies included. Some stages are more intensely discussed than others and there is also a significant difference when considering the stages against the categories of stakeholders. Articles focusing on patients present more in depth findings on all the stages as opposed to articles on other categories of stakeholders which cover briefly only three stages. There are also articles analysing narrow topics belonging to one of the stages.
The representation of the RTW process as a succession of consecutive stages was previously proposed in other studies [21, 22] with remarkable findings. One study finds that the intensity of addressing the phases is increased in the case of employers from countries with developed RTW guidance and legislation [21]. In another study the phases are understood as a continuous communicative trajectory involving different communication style [22]. Structuring the RTW process as a framework of five stages which is a finding of the present study has value because it helps stakeholders to deconstruct the process and to approach it stepwise. Employers can use this framework as a tool for planning and providing tailored company-level guidance. The five stages structure can also help policymakers to inform future guidance, interventions and policies for RTW facilitation.
Conclusions
The present study assessed the qualitative evidence on cancer and work produced during 2008-2017, against the main categories of stakeholders involved in the process and the key stages of the RTW process. The results show that patients and health providers are considered to have the most important role in RTW, while the role of employers is marginally represented in the current research. More research is required on how employers view and are able to facilitate the RTW process after cancer. The study also indicates that new forms and strategies of support must be planned and delivered by health professionals for patients who return on the labour market.
The five stages model proposed in this study can help employers and policymakers to plan and deliver tailored legislation and guidance for RTW facilitation. Finally, all stakeholders must be further trained to embrace the idea that RTW is a complex process which continues long after the survivor returns to work.