
Abstract
BACKGROUND:
Dental practitioners can be prone to stress because of the long working hours, high patient expectations, and work environment.
OBJECTIVE:
To investigate dimensions of occupational stress among dental practitioners leading to burnout and to model its causality with job satisfaction.
METHODS:
An analytical cross-sectional study was conducted for five months. A sample of 302 practicing dental practitioners was selected using the consecutive sample technique. This sample included dental practitioners working in clinical and non-clinical departments of public and private sector universities as well as those doing private general practice. A self-administered structured questionnaire based on the Work Stress Questionnaire was sent using Survey Monkey. Descriptive statistics were calculated. Spearman correlation was applied between stress scores and job satisfaction. A Chi-square test was applied to look into the association between stress levels and different categories. Univariate and multivariate analysis was performed.
RESULT:
The prevalence of overall occupational stress was high among dental practitioners (83.4%). Occupational stress was greatest in females (55.8%), dental practitioners in the private sector (55.7%), and general dental practitioners (GDPs) (47%). The overall prevalence of job satisfaction among dental professionals was 30%. Occupational stress was significantly associated with burnout and job dissatisfaction in dentistry. Stress levels and working hours were statistically and positively associated, whereas the association between stress levels and job satisfaction was inversely and significantly associated.
CONCLUSION:
The prevalence of occupational stress among dental practitioners was high and the level of job satisfaction was moderate. The model between these variables was well-fitted.
Introduction
In recent years emphasis has been laid on focusing on the mental wellbeing of individuals. Mental wellbeing helps in coping with daily stress and increases productivity at work in various organizations, and has numerous benefits both at individual and community levels [1, 2]. Psychological stability facilitates building resilience, improving relationships, and quality of life. In particular, cognitive welfare is of profound importance when it comes to health care professionals who are exposed to critical decision-making and varied stressful conditions frequently. Hence, health care professionals are inevitably susceptible to psychological stress and its consequences, risking its translation in compromised decision making and patients care [3].
Previously, numerous stressors have been identified among dental professionals in various studies [4, 5]. Dental practitioners can be prone to stress because of the long working hours, high patient expectations, and work environment [6, 7]. The literature has suggested that the dental working environment is subjected to diverse dimensions of occupational stress which provoke various stressors i.e., inappropriate dental ergonomics, extensive workload, prolong working hours, unsatisfactory wages, interpersonal relationships with patients and staff, and inability to cope with work and personal life [4, 8]. Also, the increased dental workload can result in a disorder termed as ‘burnout’ in which there is diminished interest in work. Burnout means feeling mentally exhausted, emotionally weak, and experiencing a lack of motivation in work [9, 10]. A study by Marklund et al. showed that the dentists who were dissatisfied with their jobs and had to work for long hours were prone to higher levels of stress and burnout [11]. Furthermore, lower back pain is a commonly reported physical disorder in dentists due to extensive work [12].
The British Dental Association reported that stress levels experienced by dentists are much higher than the general population [8]. A study showed 44% of dental practitioners had higher scores of stress. In relation, a significant association was seen between occupational stress and gender. Female dental practitioners reported higher stress scores as compared to males [13]. Another survey reported the presence of high-stress levels among general dental practitioners (GDPs) when compared to those teaching in dental hospitals or doing private clinical practice. Moreover, the field of practice was also found to be associated with psychological stress. In a recent study on occupational burnout, Toon et al. highlighted that patient-led stress was the most predominant type of stress observed among dental professionals leading to burnout [5]. In a similar study by Khan et al., the prevalence of stress and associated factors among dental professionals was assessed. In the study, it was revealed that 76% of dentists experienced no stress. Approximately 12 % unveiled mild levels of stress, whereas 10% exhibited moderate stress levels. A key reason for stress was workload and time management [14]. A study by Collins et al. on dental practitioners in the United Kingdom reported dentistry as one of the most stressful professions [8].
In the light of the above argument, it can be observed that the literature has illustrated conflicting and inconclusive findings in regards to levels of occupational stress and burnout among dental practitioners. Therefore, it is critical to identify strategies to manage psychological distress in dental practitioners. It was hypothesized that stress levels are high and there exists a causal relationship between occupational stress and dissatisfaction among dental practitioners. Therefore, the objective of the current study was to investigate dimensions of occupational stress among dental practitioners leading to burnout and to model its causality with job satisfaction.
Materials and methods
Study design and ethical approval
An analytical cross-sectional study was conducted in November 2019 for five months. Ethical approval was obtained from the College of Dentistry. This study followed the STROBE statement of reporting cross-sectional surveys.
Study participants
The sample size was calculated as more than 300 participants. Considering the number of dental practitioners as 1500 at 95% confidence interval, 5% margin of error, and 80% power. Raosoft calculator was used in determining the sample size [15]. All dental practitioners working in clinical and non-clinical departments of public and private sector universities as well as those doing private general practice were included in the study. Licensed but not practicing dental professionals were excluded from the study. Participants were selected using the consecutive sampling technique.
Study questionnaire
An interview-type questionnaire was formulated consisting of a total of 18 questions in 4 domains. The research team of statisticians along with authors reviewed the content of each question to make sure that the survey reflected appropriate phrasing and understanding (Cronbach’s alpha 0.80). A link containing details of the questionnaire was sent using Survey Monkey. Reminder emails were sent periodically to improve the response rate. Participant responses and information were only available to study investigators and were kept confidential.
The questionnaire comprised of validated Work Stress Questionnaire (WSQ) with certain modifications, it was divided into four parts: i) Socio-demographics of participants which comprised of the age, gender, working sector, qualification ii) Work Stress Scale based on working department, stress levels at workplace, reasons for stress at work and job satisfaction iii) Stress Coping Strategy Checklist, was based on questions regarding strategies to cope with stress like frequency of taking breaks from work, strategies to cope up with stress, access to stress management programs, getting help and support from colleagues and seeking professional help to reduce stress, iv) Burnout Inventory (BI) was constructed on working hours per day, years of experience, the number of patients treated each day, stress while performing different procedures, repetitive work without breaks. (Appendix)
Work Stress Scale and Burnout Inventory (BI) was based on Likert scale ranging from 1–5 scores where ‘1’ means ‘no stress’, 2 ‘little stress’, 3 ‘moderate stress’, 4 ‘considerable stress’ and ‘5’ meant ‘a great deal of stress’. Data were merged into two categories stressed and non-stressed. Job satisfaction was measured using the Warr-Cook-Wall Job Satisfaction Scale based on the Likert scale (extremely dissatisfied to extremely satisfied) [16–18].
Data analysis
Data were entered and analyzed using SPSS v.21. Descriptive statistics like frequencies and percentages were calculated for categorical variables whereas means and SD were calculated for continuous variables. Spearman correlation was applied between stress scores and job satisfaction. Chi-square test was applied to look into the association between stress levels and different categories p < 0.05 The generalized linear model was also applied, p < 0.25 was considered statistically significant in univariate analysis, whereas in multivariate analysis p-value < 0.05 was considered significant.
Result
A total of 302 dental practitioners were included in the present study. Out of the total 550 emails sent. 410 participants consented to take part. 306 were eligible and 302 filled the questionnaire and returned it attaining a response rate of (54%) (Fig. 1, Table 1). Among the 302 participants, 111 (36.7%) were males and 191 (63.2%) were females. The ages of all the participants were between 20 to 50 years with a mean age of 27±4.90.
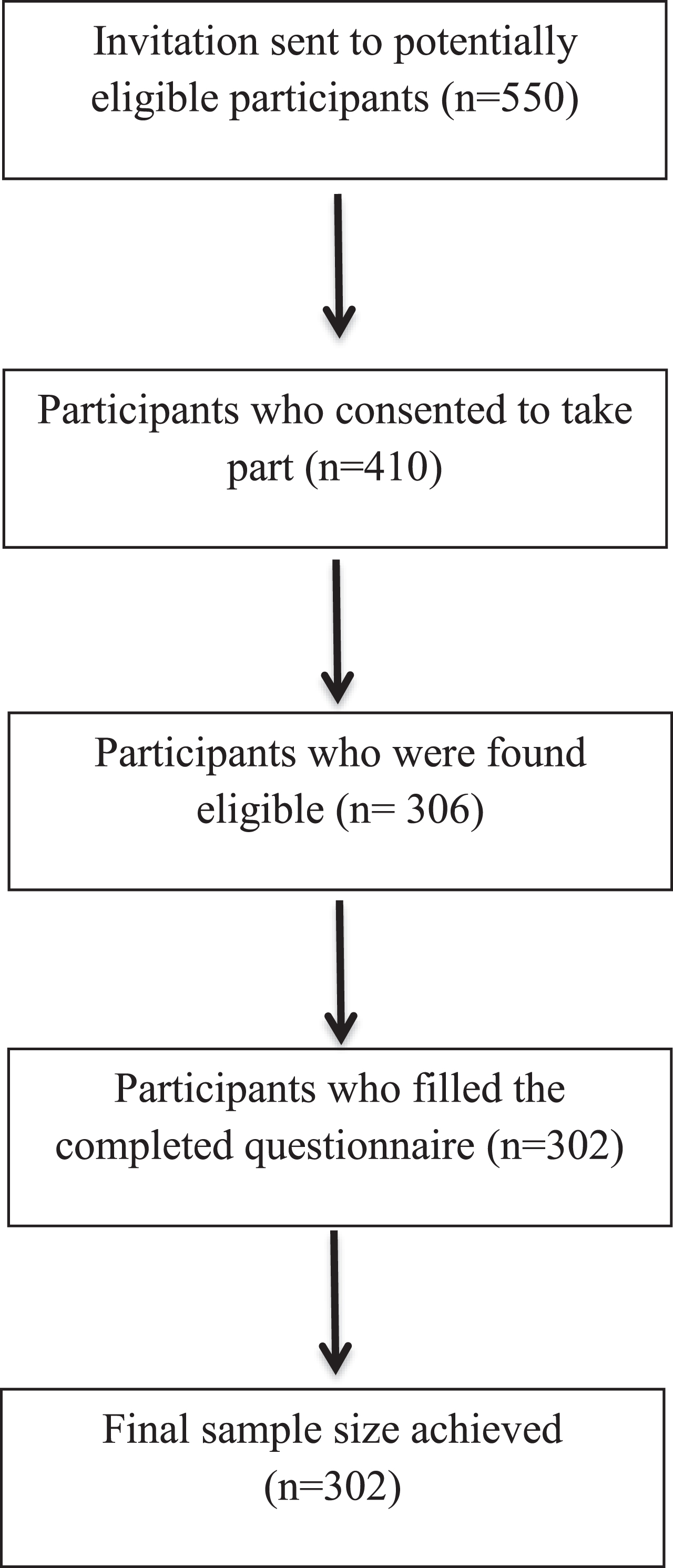
Details of participants’ recruitment.
Sociodemographic of study participants
The prevalence of overall occupational stress was high among dental practitioners (83.4%). Occupational stress according to gender was 49 (44.1%) and 62 (55.8%) in males and females respectively. When stress was assessed according to the sector it was found that prevalence of occupational stress was highest in those working in the private sector 59 (55.7%), it was followed by those who belonged to the government sector 90 (48.7%) and least was observed in those who were self-employed 11 (3.6%).
GDPs exhibited elevated stress levels (47%) when compared to postgraduate trainees (39.4%) and specialists (13.6%). When stress was assessed according to the working department it was highlighted that stress among dental practitioners belonging to different dental specialties varied according to the department they work in. Highest to lowest prevalence of stress was recorded in following departments: oral maxillofacial surgery 37 (66.7%), operative dentistry 32 (59.2%), periodontology 13(56.5%), prosthodontics 24 (50%), orthodontics 12 (42.9%), community dentistry 12 (36.7%), dental materials 6 (33.3%), oral pathology 3(33.3%) and least was found in oral biology department 15 (30%). Moreover, stress levels were high in those working in clinical departments when compared to those working in non-clinical departments.
The majority of dental practitioners 207 (68.5%) worked for 6–10 hours per day, and nearly 97.4% of dentists treated up to 20 patients per day. When participants were inquired about the history of musculoskeletal disorders it was found that 57.9% reported pain in the wrists, arms, and shoulders in the past 12 months. When job satisfaction was assessed among GDPs, it was observed that 66.2% were not satisfied with the money they were earning as dentists. In addition, the majority of participants (33%) reported that they find dentistry very effort-taking. Several stressors have also been identified among dental professionals (Fig. 2). It was seen that the commonest reason for occupational stress among dentists was being underpaid, due to which 91 (31.1%) were forced to do part-time jobs to overcome their expenses. The overall prevalence of job satisfaction among dental professionals was 30%. When scores for job satisfaction were calculated it was found that the level of satisfaction of participants was moderate with the mean score of 2.77±0.59.
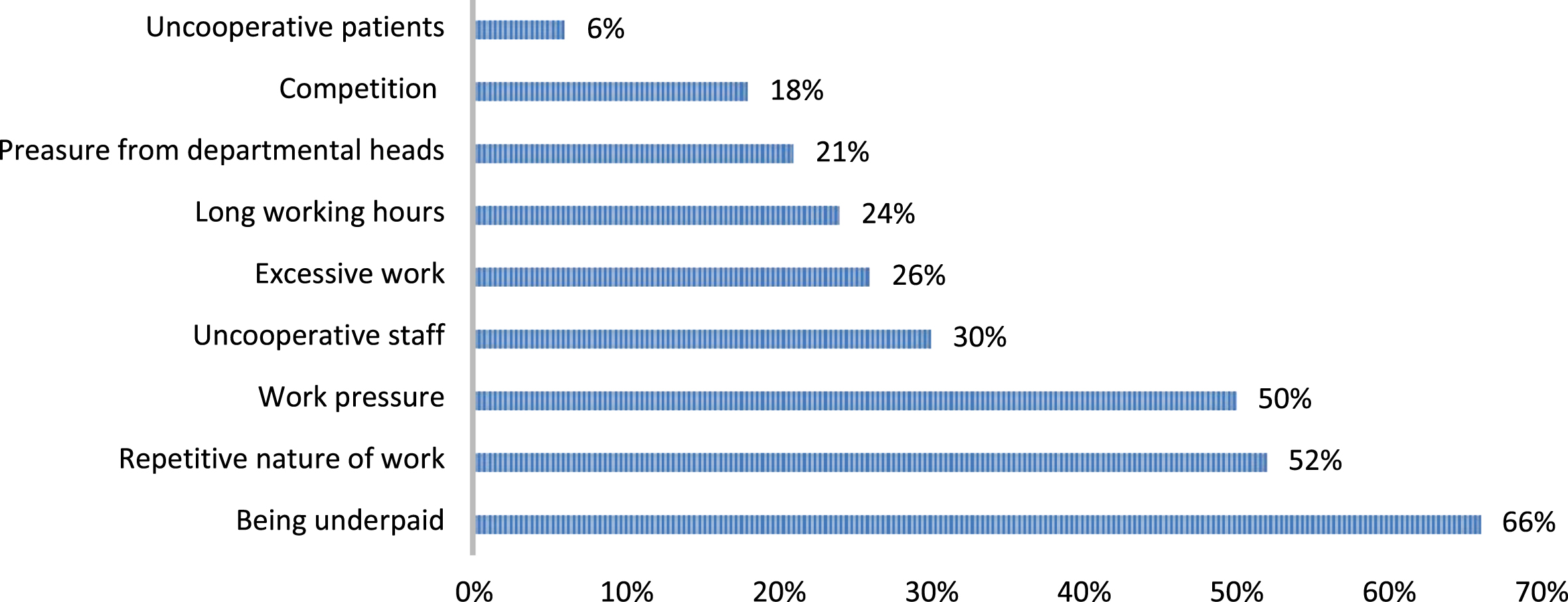
Common stressors among dentists.
Stress management strategies were also inquired from dental practitioners based on Coping Strategy Checklist (Fig. 3). 84% of participants took a break from work to cope up with stress. In our study, the commonest identified dimensions of occupational stress included work content stress, patient-led stress, productivity stress, and regulatory stress. When dentists were inquired about how often they seek professional help to lower stress levels majority of them reported they rarely seek professional help to lower stress levels and only 16.9% had access to stress reduction programs.
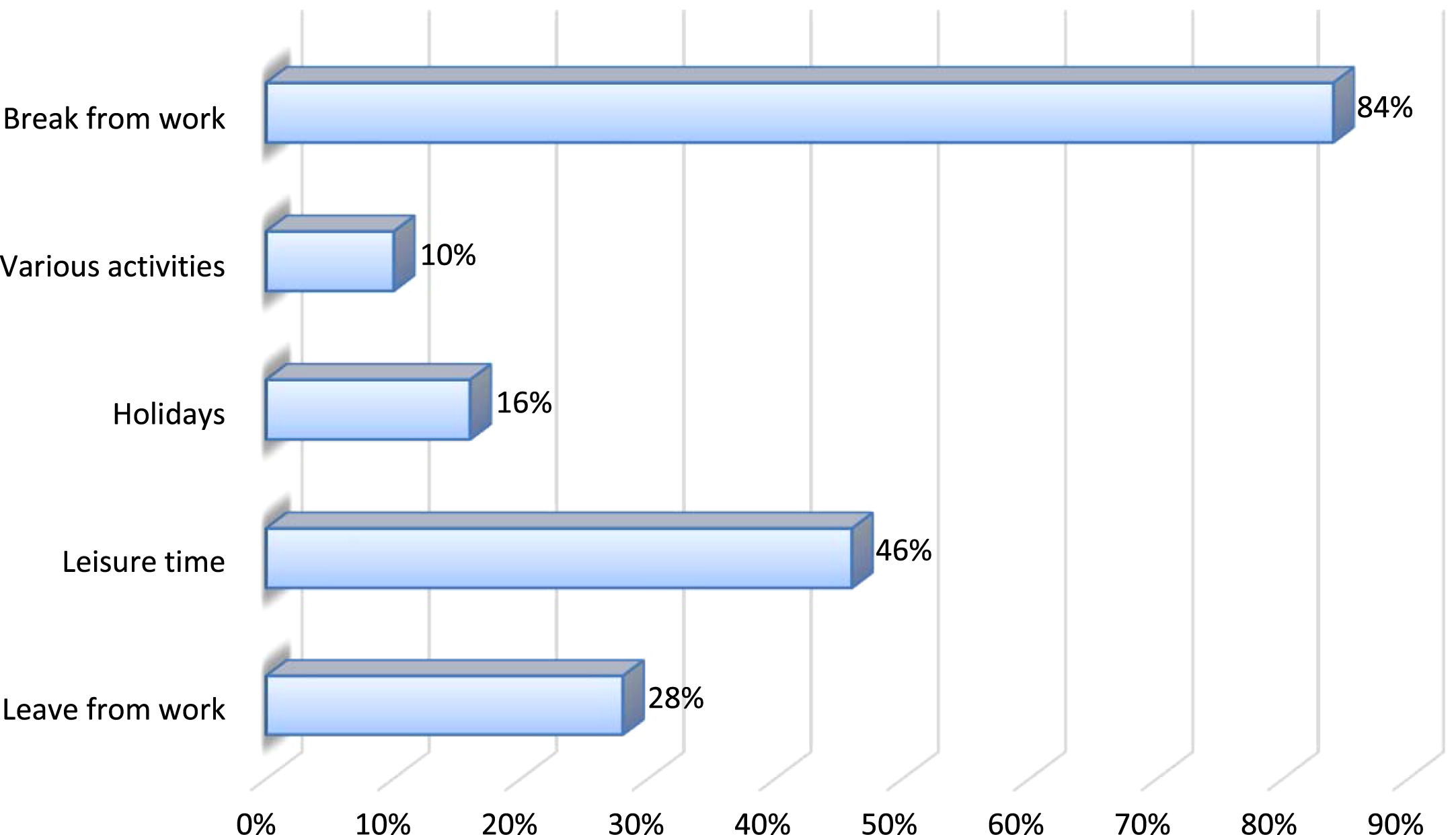
Stress management strategies adopted by dentists.
A correlation was checked between stress levels and job satisfaction. This indicated that the model between stress and job satisfaction was well fitted (R2 = 0.8). Statistically, significant association was found between stress levels, gender, working sector, qualification, department, working hours, years of experience, number of patients treated each day, and job satisfaction (p < 0.05).
In univariate analysis stress in dentistry was associated with job satisfaction, the gender of participants, working sector, qualification, department, working hours, years of experience, number of patients treated each day (p = 0.022, 0.234, 0.108, 0.024, 0.098, 0.001, 0.002) Statistically significant and positive association was found been stress levels working hours, years of experience, number of patients treated each day (β= 0.040, 0.025, 0.013) (p < 0.25). Inverse relationship was found between stress levels and job satisfaction (β= –0.250, p = 0.002) (Table 2).
Univariate and multivariate analysis (Generalized Linear model, n = 302)
However, in multivariate analysis after adjustment of confounding variables stress levels and working hours were still found statistically and positively associated (β= 0.008, p = 0.008) whereas, the association between stress levels and job satisfaction remained inversely and significantly associated (β= –0.150, p = 0.001).
The concept of ‘burnout’ was first coined by Freudenberger to identify exhaustion among health care providers who are exposed to problems and emotional distress [11]. Dental practitioners have been identified as medical professionals that are exposed to severe stress and burnout due to the nature of work as well as other factors like long working hours, the urgency of some cases, patient compliance, and work overload. It is suggested that productivity stress, work content stress, and patient-led stress, are the key dimensions identified that lead to burnout among dental practitioners [6, 19]. The relationship between occupational stress and burnout among dental practitioners has been inconsistent despite various researches on this topic which has led to the basis of this study. The objective of the present study was to investigate dimensions of occupational stress among dental practitioners leading to burnout and to model its causality with job satisfaction. In the present study, it was hypothesized that stress levels are high and there exists a causal relationship between occupational stress and dissatisfaction among dental practitioners.
The existing study has found a high prevalence of occupational stress and moderate levels of job dissatisfaction among dental practitioners which accepts the hypothesis. Also, a statistically significant association was found between stress levels and variables like gender, qualification, working hours, and job satisfaction. Stress levels and working hours were found statistically and positively associated whereas, their association between stress levels and job satisfaction was inversely and significantly associated. Being underpaid was commonly reported as the cause for low levels of job satisfaction among dental practitioners.
In the current study a low response rate was noted among dental practitioners. A possible explanation for this low response rate was the duration of the study, busy clinical settings, and personal commitment [20]. In the present study high prevalence of occupational stress among dental practitioners was found (83.4%) which is in agreement with other studies [21, 22].
When gender was taken into consideration it was identified that occupational stress and gender were significantly associated. It can be said that gender plays a key role in occupational stress. In the current study, female dental practitioners exhibited higher stress levels compared to males. These findings were persistent with work by Pallavi et al. who reported greater stress in women dentists is due to their innate characteristics to constantly juggle between work, financial pressures, and family life [23, 24]. Another key finding was that stress levels were greatest in GDPs compared to specialists. This outcome was consistent with a study by Najafi et al. A possible explanation to this finding might be attributed to lack of experience in specialized work and patient management [25].
A key finding of the present study was that with the increase in years of experience, occupational stress became less prevalent. This trend follows work by Porto et al., [26]. A probable reason for this outcome might be due to increased exposure to patients over the period. When stress was assessed according to dental specialty it was observed that those who worked in the oral and maxillofacial surgery department revealed the highest stress scores. This might be attributed to the possibility that due to exposure to dental emergencies and work in changing shifts dental surgeons are more subjected to stress. These findings are in agreement with Alkindi et al. and Dehand et al. who reported a high prevalence of stress among those who were specialized in oral maxillofacial surgery [27, 28].
The majority of dental practitioners (66.2%) were not satisfied with their job which could be one of the reasons for their increased stress levels. Previously, one of the studies has shown that job-related stress which GDPs face directly affects their family especially their spouse. Therefore, they cope up with stress by maintaining a balance between their job and family [18]. The present study showed that the most common strategy adopted by the participants to reduce their work stress was to take a break from work (84%) and spending leisure time (46%). The greatest hindrance in coping with stress was reported due to lack of access to stress reduction programs. Only a minority of the participants reported that they have access to stress management or stress reduction programs (16.9%). These strategies are in agreement with other studies [4, 11]. A study by Sakzewski on Australian dentists reported that the conditions in which dental practitioners work make them more prone to musculoskeletal disorders which increases with extensive working hours [29]. Similar findings have been observed in our study which has revealed that many dental professionals (57.9%) experience musculoskeletal disorders due to similar reasons.
A systematic review by Leggat et al. perceived dentistry as a very stressful profession [30]. This finding contradicts the results of our study which shows that most dental practitioners find their job only a little stressful (32.8%) or moderately stressful (31.5%). Choy et al. reported that the medical doctors and dental practitioners who teach in addition to their clinical work experience high levels of stress [31]. But some evidence has also shown that teaching may even reduce their job-related stress [32]. In the current study GDPs who were related to non-clinical subjects yield lower levels of stress and greater job satisfaction.
This study has highlighted that work-related stress and occupational burnout are quite prevalent among dental practitioners (83.4%). These findings must be considered alarming as increased stress levels might compromise the quality of treatment and patient management hence must not be neglected. This issue needs to be addressed at the individual level by identifying the root cause of the problem and providing opportunities to GDPs to have easy access to stress management programs. Also, the incorporation of stress management is essential in the dental curriculum so that they can be trained at undergraduate levels regarding the handling of medical disputes, administrative problems, and time management [4, 33]. Furthermore, cultural change is required in this sector to overcome this issue by building a healthy working environment, workload distribution, and providing better wages [10].
This study has few limitations, due to consecutive sampling technique equal numbers of participants from each department were not catered indicating poor generalizability. Further work is required on the same topic using different study designs to ensure the cause-and-effect relationship between stress and other confounding variables. More work is needed comparing the stress levels in medical doctors and dental practitioners to extrapolate findings of the current study. A qualitative study design is recommended among dentists as well to reciprocate the findings of the present study.
Conclusion
The prevalence of occupational stress among GDPs is high and the level of job satisfaction was moderate. Occupational stress was significantly associated with burnout and job dissatisfaction in dentistry. It was concluded that stress levels and working hours were statistically and positively associated whereas, the association between stress levels and job satisfaction was inversely and significantly associated. Those working in clinical departments and running their private practice exhibit the greatest stress levels. These findings have led us to the conclusion that all dental specialties have somewhat equal or high work-related stress.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors are grateful to the Researchers supporting project at King Saud University for funding through Researchers supporting project No. (RSP-2021-44).
Appendix
Appendix: Work Stress Questionnaire
| Socio demographics |
| 1. Age: |
| 2. Gender: |
| a. Male |
| b. Female |
| 3. Which sector do you work in? |
| a. Private |
| b. Government |
| c. Self employed |
| 4. Please select your qualification |
| a. Post graduate trainee |
| b. General dentist |
| c. Specialist |
| Work Stress Scale |
| 5. Working department: |
| a. Oral diagnosis |
| b. Oral surgery |
| c. Prosthodontics |
| d. Orthodontics |
| e. Periodontology |
| f. Operative |
| g. Oral pathology |
| h. Dental materials |
| i. Community dentistry |
| j. Oral biology |
| 6. How would you describe your stress levels at workplace? |
| a. No stress |
| b. Little stress |
| c. Moderate stress |
| d. Considerable stress |
| e. A great deal of stress |
| 7. If yes, then which of the following would you select as the |
| reasons for stress at work? |
| a. Being underpaid |
| b. Repetitive nature of work |
| c. Work pressure |
| d. Uncooperative staff |
| e. Excessive workload |
| f. Long working hours |
| g. Pressure from departmental heads |
| h. Competition at work |
| i. Uncooperative patients |
| 8. Are you satisfied with the money you are earning through this |
| profession? |
| a. Yes |
| b. No |
| Stress Coping Strategy Checklist |
| 9. How often you decide to take a break from work? |
| a. Never |
| b. Seldom |
| c. Sometimes |
| d. Often |
| e. Always |
| 10. What are the methods through which you reduce your stress |
| levels at work? |
| a. Leave from work |
| b. Involvement in leisure activities |
| c. Going on holidays |
| d. Through various activities |
| e. Taking break from work |
| 11. Do you have access to stress management or stress reduction |
| programs? |
| a. Yes |
| b. No |
| 12. How often do you seek help from colleagues to reduce the |
| levels of stress? |
| a. Often |
| b. Rare |
| c. Uncertain |
| 13. Do you seek professional help to reduce stress at the |
| workplace? |
| a. Yes |
| b. No |
| Burnout Inventory |
| 14. Working hours/day: __________________ |
| 15. Years of experience: __________________ |
| 16. Number of patients treated/day: ________ |
| 17. How stressful is it to manage a patient having different |
| dental procedures? |
| a. No stress |
| b. Little stress |
| c. Moderate stress |
| d. Considerable stress |
| e. A great deal of stress |
| 18. Do you feel tired due to repetitive work without taking |
| breaks? |
| a. Yes |
| b. No |