
Abstract
BACKGROUND:
Low back pain (LBP) is the most common musculoskeletal disorder work-related health problem in Europe, affecting millions of workers. It is estimated that 60–80% of the population will suffer at least one episode of mechanical LBP during their life.
OBJECTIVE:
To evaluate the kinesiotape (KT) effectiveness in mechanical LBP.
METHODS:
This was a double blinded, randomized-controlled clinical trial. Twenty-eight nursing and cleaning auxiliaries from Salamanca received a manual therapy program and a bandage of KT or false kinesiotape (FKT). They received two sessions a week for three weeks and a follow-up one month after the last session. Pain, range of motion and function were measured at baseline, at the end of each session and a month after the last session.
RESULTS:
Work-related musculoskeletal disorders and LBP are responsible for a high prevalence of sick-leave and absenteeism. Manual therapy and KT has demonstrated to reduce pain and to increase range of motion and function being effective in this population. There are statistically significant results in both groups in all measurements for all variables. KT seems to be superior, however, both have a positive effect on LBP. Although benefits decrease, long-term treatments focusing on pain alleviation and functional recovery is needed to maintain the benefits achieved.
CONCLUSION:
KT was an effective complement for this treatment. Although both show improvements, KT is recommended. Future studies are needed to demonstrate KT properties, to establish a treatment protocol to prevent chronic LBP and to avoid sick leave and absenteeism.
Introduction
Work-related musculoskeletal disorders (MSDs) are defined as symptoms caused or aggravated by occupational risk factors, including persistent discomfort, damage, or pain in body structures [1]. MSDs are the most common work-related health problem in Europe, affecting millions of workers [1–3]. Within MSDs, low back pain (LBP) is the most common problem across workers, with sickness or absence episodes. Static positions, lifting, bending and twisting movements can be mechanical causes for LBP in the workplace [2–4].
MSD is related with several works and many researchers have tried to establish its prevalence and relations with age, body mass index and gender [5]. This pathology is one of the top 5 causes of disability in 2016 [6]. It is estimated that between 60–80% of the population will suffer at least one mechanical LBP episode during their life [3, 7–10] and 5–20% of them will become chronic [2, 11]. In Spain, the LBP prevalence in 2006 was 19.9% [12].
LBP interferes with numerous daily activities from walking and dressing to many work-related functions, thereby affecting quality of life [9]. LBP produces mobility restriction, long-term disability, and quality of life impairment [8]. It is also associated with an increased risk of depression and psychosis spectrum disorders, sleep disorders, anxiety and stress sensitivity, low mood, somatization tendency and adverse health beliefs [2, 13]. Because of its frequency as a chronic or recurrent problem, a treatment focusing on pain alleviation and functional recovery is needed [14].
MSD is the leading cause of absenteeism in Europe, the United States and Canada, with a high prevalence in nurses and nursing assistants [1, 8]. Absenteeism is the first economic indicator. 27.8% of subjects reported health-related absenteeism and 14.1% had problems in the low back [15]. The LBP total number from 1993 to 1997 reached an average of 55,388/year and represented 11.4% of the total temporary disability associated with all sick leave in Spain during this period [16].
Treatment and days lost from work make musculoskeletal pain the most common musculoskeletal disease [11]. An article recently published established a positive relation between suffering from LBP, jobs with physical demands and absenteeism [17]. LBP represents a loss of about 21.9 working days/worker and year. This pathology is a public problem, responsible for work disability and elevated direct and indirect health-care costs [8, 9]. There is no exact data on the economic impact of this pathology, though the literature suggests the absenteeism cost and healthcare expenses associated with musculoskeletal pain could exceed 3 million euros per year [18]. One article estimated the annual workers’ compensation cost for LBP in Spain during 1993–97 was 11 billion pesetas (approximately €67 million) [2] and in 1998 represented an average cost of 11,252,404,056 old pesetas [15].
There are numerous LBP treatments such as kinesiology, medication, electrotherapy, manual therapy, educational programs and exercises [8, 19]. The main objective is to relieve pain and prevent chronicity; however, these treatments have only short-term benefits [19]. There is not a clear superiority of one technique over the others, nonetheless, when the effectiveness of manual physiotherapy against other techniques such as clinical neurodynamics [20], exercises [21], or the influence of biopsychosocial factors [22] has been studied, it has been demonstrated that the group receiving manual physiotherapy improved compared to the group treated with the above-mentioned or untreated therapies.
In the 1970s, Dr. Kenzo Kase developed kinesiotape (KT) in Japan. It involves the application of elastic adhesive therapeutic tape for pain, swelling, oedema, scar healing, proprioceptive facilitation, and relaxation of muscles [4]. It is waterproof, does not contain chemical substances and is inexpensive [4, 11]. The mechanism can be inhibitory or excitatory, depending on the direction of tape application. It has several therapeutic benefits: “normalization of muscular function, increase in lymphatic and vascular flow, reduction in pain and contribution to correcting possible joint misalignments” [23, 24]; but the clinical effects are unknown [8]. The effectiveness found in the literature is not conclusive [19].
On the one hand, we have found studies that apply KT in LBP [25, 26], in femoro-patellar pain, ankle joint instability, external lateral ligament sprain, increased quadriceps strength, rotator cuff tendinosis and dystrophy sympathetic reflex [27], obtaining good results both analgesic and increase of amplitude, among others. On the other hand, Paoloni et al. [28] in chronic lumbar pain, Jaraczewska and Long [29] in hemiplegia and Yasukawa et al. [30] in upper limb muscle weakness, use KT as a complement in the treatment of different pathologies. It is in all cases an effective complement to achieve effects such as decreased pain and improved function or proprioception. Due to the importance of this pathology, the existence of a treatment that diminishes and/or eliminates the painful symptomatology with the consequent increase of the articular amplitude and the recovery of the function, allowing the return to the work and the reduction of the labor casualties.
Objective
This study consisted of a manual physiotherapy treatment by adding a KT or false kinesiotape (FKT) in nursing and cleaning auxiliaries with mechanical LBP to find an effective treatment which reduces sick-leave and guarantees a rapid recovery and return to work.
Methods
Design
This was a double blinded, randomized and controlled clinical trial.
Participants
Nursing and cleaning auxiliaries of Salamanca aged between 18 and 67 years old who suffer from LBP were included in the study. Pain associated with traumatism, specific pathology such as hernia, protrusion, pharmacological treatment, neurological process in low back, osteosynthesis in the area or being pregnant were the exclusion criteria.
The study was set at the Faculty of Nursery and Physiotherapy of the University of Salamanca. Over a period of months, 57 auxiliaries referred by their physician were contacted, of whom 14 did not want to participate and 15 had exclusion criteria (Fig. 1). We started the recruitment in October 2016 and treatment finished in December 2016. The final sample consisted of 28 nursing and cleaning assistants; they received an information sheet and signed an infor-med-consent form to be admitted. Sampling was non-probabilistic, consecutive, and randomly distributed in 2 groups using the Epidat program (version 3.1).
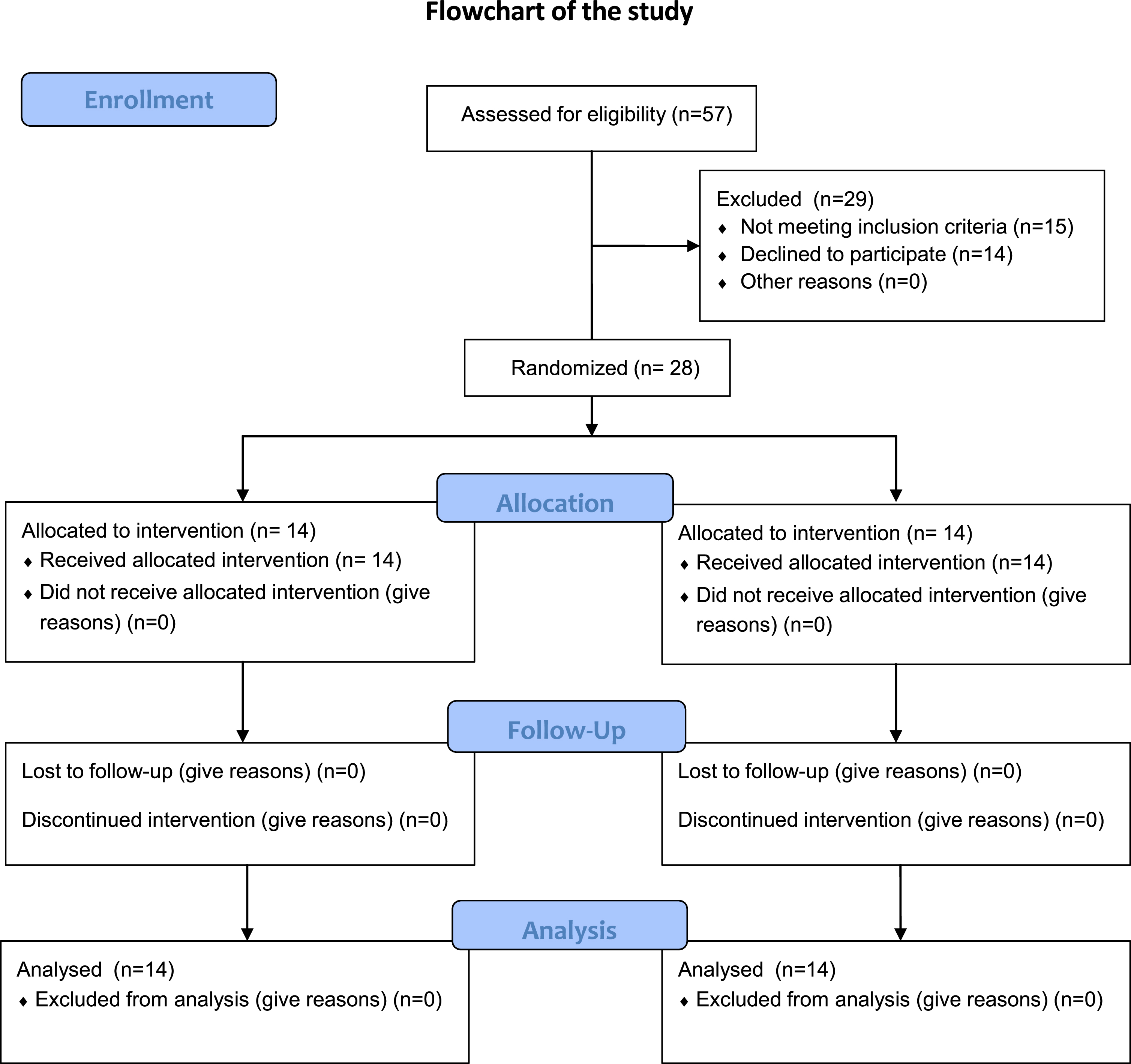
Flowchart of the study.
Since no previous studies were found to determine the sample size of the study, a pilot study was conducted with 11 patients to calculate the minimum sample size we needed for the study. We used the mean and standard deviation (SD) of the main variable (pain improvement). In the FKT group the mean was 6.636 (SD = 1.566) and for the KT group was 8 (SD = 1.183). With these conditions, the effect size or standardized difference of means (Cohen’s d) was equal to 1.03038. Using the Gpower program and considering hypotheses to a queue, alpha error of 0.05 and power of 80%, the required sample size was 26 subjects (13 in each group). We finished the recruitment with 2 more subjects than the minimum established to obtain significant results.
Interventions, blinding and randomization
Both groups received the same treatment of manual physiotherapy consisting of low back passive mobilizations (3 planes of movement), spinal erector massage techniques, lumbar muscle pressure inhibition, passive stretching and active exercises. One group additionally received KT and the other group FKT at the end of the session.
The study was carried out by 2 professionals (P1 and P2) in 2 different rooms. In the first room, P1 (blinded from the randomization) selected the sample and performed the initial exploration. In the second room, P2 randomly assigned the sample using numbers extracted from a computer program. Patients were coded as numbers; these numbers were randomly allocated to intervention or control group. When patients started treatment they received one consecutive number, in this way, just P2 knew the group of each patient. This procedure guaranteed the blindness of the evaluator and the patients. P2 also performed the manual treatment to both groups in this room and applied the KT to the KT group and the strips of adhesive tape (FKT) to the control group, ensuring masking of the patients (KT and FKT were the same color). After the session, patients returned to the initial room where P1 reassessed them. The following sessions were done in the same way. The review was carried out by P1 one month after the 6th session.
Outcomes
Pain was measured with the Visual Numerical Scale (0–10 points); joint amplitude was measured with a CROM goniometer (degrees of active movement), and the Oswestry questionnaire was used to measure function (0–100 points).
Pain and joint amplitude were measured at the beginning (pre-test), at the end of the second session (post-test1), at the end of the 6th session (post-test2) and at one month after the 6th session (post-test3). Function was obtained at the beginning (pre-test), at the end of the last session (post-test2) and in the revision at one month after the last session (post-test3).
Data analysis and statistical methods
All data were collected in individual evaluation sheets coded, to guarantee the anonymity and the group location of each patient. After the completion of all evaluations all data were extrapolated to a Microsoft Excel document to its posterior analysis.
Both treatments and the measurements taken at the beginning, at the end of the first week, at the end of the manual therapy treatment and during the review at the end of the treatment were compared and analyzed. The obtained data were organized and analyzed with the statistical package Jamovi version 1.2.27. Before starting any other analysis of the data, we checked the normality of our dependent variables using the Shapiro-Wilk test. A descriptive analysis of the socio-clinical-demographic variables of the sample was carried out.
Non-parametric repeated measures ANOVA (Frie-dman) to establish the difference between the initial and final average of each variable in the same group were used. These results inform about the effectiveness of KT and FKT independently.
Durbin-Conover pairwise comparisons were used to determine the difference between the initial and final average of each variable between groups. This test showed information about the effectiveness of KT versus FKT to establish potential comparisons to prove which bandage was better to apply.
Ethical considerations
All participants were informed about this study procedure, they received an information sheet and signed an informed-consent form to participate. The study obtained approval from the University Hospital of Salamanca Committee (Paseo San Vicente, 58-182, CP: 37007, Salamanca, Spain) on 23 May 2011. The guidelines of the Declaration of Helsinki and ethical considerations were followed as well as the anonymity of the data. Participants received an identification number to guarantee their anonymity across the implementation of the study and its posterior analysis.
Availability of the data
The research data extracted in this research were approved by the ethics committee of the University of Salamanca. Personal data was codified, every evaluation was registered on paper and was saved by the researcher team. Data was collected in a Microsoft Excel document for its posterior analysis. All study data are available under reasonable request to the corresponding author.
Results
The sample was composed of nursing and cleaning assistants. A total of 57 subjects were contacted from their work, 14 did not want to participate and 15 had exclusion criteria. A final sample of 28 nursing and cleaning assistants, 14 in each group (27 women and 1 man) completed and finished the study (Fig. 1).
First, a normality analysis of the data obtained in the pre-test and in the different post-tests of the dependent variables was performed, considering the treatment applied.
The homogeneity of the treatment groups regarding sex variable was checked using the Fisher exact statistic. The final sample was composed by 28 subjects: 1 male (3.6% of the total) and 27 female (96.4%). This statistic has shown that there were no significant differences between groups in the proportion of men and women (p = 1,000). In the FKT group the 14 included subjects were women (100%), whereas in the KT group 1 male (7.2%) and 13 women (92.8%) were included.
Two treatments were analyzed independently for each variable, to determine if they were effective without establishing comparisons between groups, and when these improvements began to be noticed. A non-parametric repeated measures ANOVA (Friedman) test was performed. It was found that for both treatments with KT and FKT the repeated measures ANOVA were significant (p < 0.001) for all variables. Patients reduced their pain and disability, and they improved their function.
The Durbin-Conover pairwise comparisons test to establish differences between groups, found that in the KT group and in the FKT group there were statistically significant differences (p < 0.001) from the first week of treatment (post-test1). After this first-week, improvements were perceived in all the variables measured. In addition, in the KT group, statistically significant improvements continued to be produced with each of the follow-ups (post-test2, 3 weeks from the start, and post-test3, one month after the last session) in all variables except OSWESTRY, FLEXION, and LEFT ROTATION variables. There were no improvements from post-test2 to post-test3. In the FKT group, statistically significant improvements (p < 0.05) were also found with the first week of treatment, and from the first week to post-test2, but from post-test2 to post-test3 the improvements were only statistically significant (p < 0.001) in EXTENSION and in LEFT LATERAL BENDING variables (Table 1).
Repeated measures ANOVA (Friedman) and pre-test, post-test1, post-test2 and post-test3 medians
Repeated measures ANOVA (Friedman) and pre-test, post-test1, post-test2 and post-test3 medians
*Pain measured with Visual Numeric Scale (VNS): 0–10 points. **Oswestry measured the functional status: 0–100 points. ***Range of motion measured in degrees.
As both techniques were effective, a new variable called “improvement” was created, which measured the magnitude of the change. This measure assessed the difference in scores from the pre-test to the last follow-up. The main improvement was statistically greater for the KT group than for the FKT in the variable OSWESTRY (t (26) = –2.277; p = 0.031), FLEXION (t (26) = –6.447; p < 0.001) and EXTENSION (t (26) = –3.030; p = 0.005) (Fig. 2).
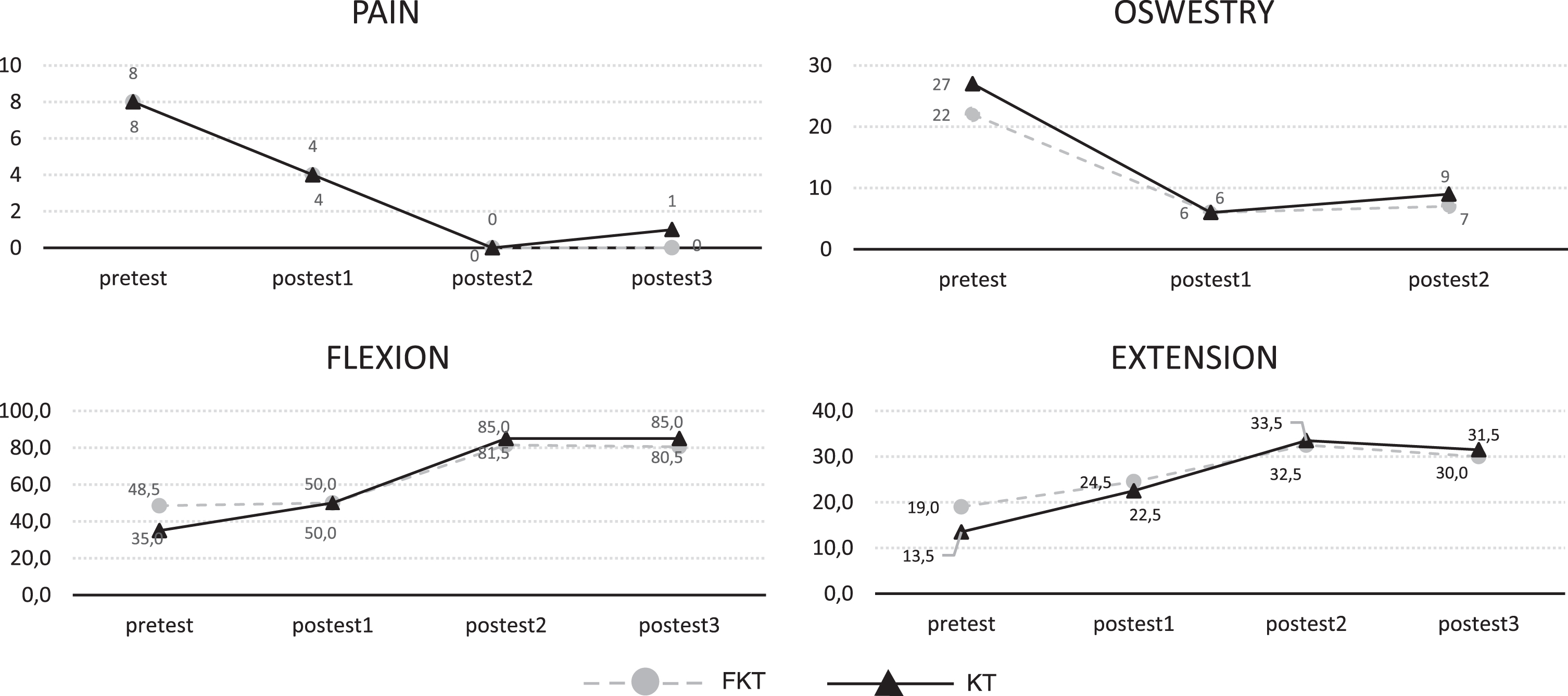
Pain (*), Oswestry (**), Flexion and Extension (***) pre-test and post-tests. *Pain measured with Visual Numeric Scale (VNS): 0–10 points. **Oswestry measured the functional status: 0–100 points. ***Range of motion measured in degrees.
It must be considered that before starting the treatment both groups were not equal in the mean of all the variables. In the variables VNS (t (26) = –2.182; p = 0.038) and OSWESTRY (t (26) = –2.114; p = 0.044) the scores of the KT group were higher than the FKT group, and in the FLEXION (t (26) = 4.811; p < 0.001) and EXTENSION variables (t (26) = 2.128; p = 0.043) the scores of the FKT group were higher than those of the KT group. Therefore, the score of both treatments was compared at the end of the follow-up (post-test3) regardless of the improvement in relation to (with respect to) the initial moment since a ground effect could occur. In this case, the differences are statistically significant only for the variable EXTENSION (t (26) = –2.209; p = 0.036), being the final ones in favor of the KT group.
The application of KT and FKT with manual physiotherapy treatment has been demonstrated to be effective. It is important to highlight the decrease in pain and the increase in mobility and function, with significant differences (p < 0.001) in both groups between the values obtained before applying the treatments and those achieved after implementing them. OSWESTRY, FLEXION and EXTENSION variables show significant results in favor of the KT group over the FKT group.
At least, 24% of the Spanish population has suffered from some type of back pain in the last year. This pathology is more frequent in women (30.2%) than in men (17.5%) [18]. This agrees with our sample, where 96.4% were women.
Several articles have also investigated this type of population in relation to the physical and psychological factors at work (shift work, long hours and the patient’s stress management) [1, 32]. Juniper et al. [33] reported a 17% LBP prevalence in female nurses, nursing aides and head nurses in Italy in the last 12 months; however, Samaei et al. [31] expressed a prevalence of 69.5% in the previous 12 months too.
Another study [1] stated the association between work-related psychosocial factors and MSD in hospital nurses and nursing aides, and, the “frequent and extreme trunk awkward postures” could develop LBP [32]. Preventive and ergonomic strategies are needed to reduce this prevalence [1, 32]. Although this study has been focused on nursing and cleaning aides, other health professionals are exposed to these work factors too [34].
There are more than 150 diagnoses of musculoskeletal conditions which affect the locomotor system. These pathologies affect more than 1.7 billion people worldwide, are the second-greatest cause of disability and have the fourth-greatest impact on the overall health of the world’s population [19]. Coggon et al. [35] recruited a sample of 861 participants from 47 occupational groups (nurses, office staff and other workers) and 18 countries across five continents, of which 10% reported MSD pain in the last month. The highest risk of absenteeism was attributed to LBP in 235 people.
The high prevalence of this pathology makes an effective therapeutic alternative necessary. The use of KT has increased in popularity among physical therapists. KT is an inexpensive, easy and quick treatment method [7]. The effectiveness of KT has been researched, but due to the great heterogeneity in the interventions and combinations of treatments, the results are controversial [7, 19]. Several studies have demonstrated a significant beneficial effect of KT when compared to various placebo applications. It has been shown that KT can normalize muscle tone, increase concentric muscle strength and isometric contraction. The main difference compared to traditional tapes is the proprioceptive and nociceptive stimulation. KT provides muscle support, joint malalignment correction, endogenous analgesic system activation and congestion fluids elimination [11].
KT has also been proven in other types of population such as young subjects to determine the resistance to fatigue of lumbar extensor muscles. This study supports the paravertebral application of KT to prevent lumbar fatigue. Subjects could maintain the position for a longer duration than those without any taping [11].
In the present study, the application of KT was in “H” without tension. There are different applications of KT in the lumbar region as well as different tensions at the time of its application. It seems that different tensions do not influence pain sensitivity and lumbar mobility [7].
After KT application in chronic non-specific LBP, subjects experienced a significant improvement in postural control [36]. The motion improvement has been attributed to a greater recruitment of motor units in spinal erector muscles [7]. In line with our study, Castro-Sánchez et al. [8] published a study where, after comparing KT with FKT, disability was reduced in LBP patients; however, the effects were too small to highlight them clinically. We cannot make an exact comparison in our study due to the great difference in duration between both. Although the effects have been small, the application is quick, the bandage is maintained for a week and does not require as much effort as a therapeutic intervention would normally involve, so these aspects make it worthwhile to use, in addition to its low cost and possible combination with other techniques such as exercises [8].
Our patients agreed that the use of KT added a subjective positive sensation of comfort. This correlates with the study of Bataller et al. [3] where “wearing a lumbar support is a sensation of comfort, or even of pain relief”. The long-term use of a lumbar orthosis seems to generate a weakening of the trunk muscles; for that reason, we chose KT instead of a lumbar support to guarantee lumbar mobility.
It is thought that when there is pain, physical activity should be avoided [35]. However, physical activity should be part of the treatment since a sedentary lifestyle implies a deterioration in physical condition. It seems that people with chronic back pain do not do less exercise but do it at a lower intensity. According to these authors “vigorous activity should be considered not only a strategy to prevent this pathology, but also a therapeutic objective in these patients” [18]. In the present study, exercises in the 3 planes were explained and patients were encouraged to integrate them into their daily routines.
The European guidelines for chronic non-specific LBP treatment recommend therapeutic exercise to increase muscular flexibility and endurance [7]. In our study, we have tried to combine these recommendations with the conventional treatment of LBP with KT as stated by Nelson et al. [4] in their study.
The evidence that supports KT effectiveness app-lied in isolation in LBP is low despite being superior to the fake bandage [19]. Although KT has “a small effect in alleviating musculoskeletal-related disorders such as arthritis, knee pain or LBP”, it has not shown superiority compared to other treatments in this modality alone or in conjunction with other treatments in relation to pain and disability [4, 19]. The evidence for KT vs FKT in relation to joint mobility is limited [4]. However, pain reduction does seem to improve postural control in LBP [36]. Additionally, the tape contact with the skin is a sufficient proprioceptive stimulus to generate cutaneous mechanoreceptor inputs to the central nervous system; to decrease nociceptive inputs (gate control pain theory); and to activate descending pain inhibitory systems. It may also increase muscle blood circulation and reduce oedema, which will decompress sub-cutaneous nociceptors, decreasing pain perception [7]. These results support the use of KT as a complement to LBP treatment. Its own creator established that it is not a substitute for treatment but that it allows a better quality of movement, an increase in movement and an improvement in motor control [4].
Recent studies show new applications of KT that need to be investigated. Mohammad Forozeshfard et al. [37] have tested the efficacy of KT in young females with menstrual LBP, with good results in relation to pain and disability. Finally, Lee Jung-Hoon et al. [38] in their study applied KT in chronic LBP with sacroiliac joint dysfunction, to increase sacral horizontal angle. In the present study, any low back pathology was excluded; therefore, to compare our results is not possible.
Despite not obtaining statistically significant results, our sample improved through the reduction of pain perception and increased mobility, which seems to indicate the benefit of adding KT to conventional LBP treatment. Álvarez-Álvarez et al. [11] indicated that correct application of KT is more beneficial than non-specific application (placebo), and non-specific application has more benefit than no application. This would explain the improvement in our sample despite the statistical data.
Limitations
It should be noted that the study has limitations. On the one hand, the existence of significant differences in pain, oswestry, flexion and extension variables in the pre-test should be considered. There has been a bias in these four variables which may be due to the fact of having performed a random distribution of the subjects by simple chance. In future investigations, a stratified random sampling will be performed as a control mechanism. On the other hand, some patients reported skin irritations as well as itchiness with FKT. Unfortunately, there was no follow-up after post-test3 (one month after the last session), so it is not known if the results were maintained or if the pain and limitation of movement as well as the decrease in function were again present. Long-term studies must be implemented.
Conclusion
KT and FKT have shown similar results, but it is recommended to use the first one to avoid possible skin irritations. Significant improvements were found in both groups between the initial and the final evaluation. Participants reduced pain and did not need a sick leave to recover from this pathology. KT has proven to be an effective complement to manual therapy treatment which could avoid sick leaves and prevents the absenteeism at work of this population.
Long-term future studies that demonstrate an effective protocol treatment for LBP are needed to reduce work loss (with its economic cost) due to this pathology.
Footnotes
Acknowledgments
The authors thank the patients who made this study possible.
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical considerations
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.