
Abstract
BACKGROUND:
Although pulmonary rehabilitation programmes (PRPs) benefit patients with chronic obstructive pulmonary disease (COPD), poor adherence to these programmes is common.
OBJECTIVE:
This study aimed to analyse the factors associated with poor long-term adherence after completing a PRP.
METHOD:
We conducted a retrospective study of 70 patients with COPD who performed an 8-week outpatient PRP that included 24 sessions of aerobic training, skeletal muscle resistance exercises, physiotherapy and COPD education. The study classified the patients into 2 groups: (1) long-term adherence and (2) long-term non-adherence to the PRP. We considered long-term non-adherence when the patient did not attend the 32 weeks follow-up visit after beginning the PRP. We measured the degree of dyspnoea, quality of life, physical activity, anxiety-depression status, submaximal exercise capacity and COPD exacerbations in both groups.
RESULTS:
The patients’ median age was 69.6 [63.8–75.0] years, and 71.4% were men. The median forced expiratory volume in 1 second was 60.0 [47.7–68.0] % of that predicted. We observed total COPD exacerbations and severe COPD exacerbations in the last year in 32 (45.7%) and 22 (31.4%) patients, respectively. Dyspnoea, physical activity and quality of life significantly improved after completing the PRP. Long-term non-adherence to the PRP was observed in 32 (45.7%) patients. In the single regression model, severe COPD exacerbations (p = 0.04) and dyspnoea (p = 0.03) were associated with long-term non-adherence to the PRP. In the multiple regression model, only severe COPD exacerbations remained as an associated factor (OR 2.7; 95% CI 1.1–8,1; p = 0.04).
CONCLUSION:
Approximately half of patients who complete PRPs present long-term non-adherence to the programme. Severe COPD exacerbations are associated with long-term non-adherence.
Introduction
COPD is a multisystem disease with cardiovascular, metabolic and musculoskeletal manifestations that provokes physical deconditioning and loss of muscle strength at long-term progression [1–3]. Likewise, this disease is characterized by the presence of COPD exacerbations that impact on the dyspnoea, the quality of life, impair lung function, increase hospital admissions and are associated with higher mortality [3–5].
Pulmonary rehabilitation (PR) consists of a comprehensive intervention comprised of various therapies tailored to the patient’s needs and includes muscle training, education and changes in lifestyle habits [1–3]. PR is a non-pharmacological therapy for treating COPD as it improves dyspnoea, exercise capacity, anxiety, depression and other comorbidities [2–4].
Although COPD management guidelines recommend PR, the intervention is not adequately offered or provided to all patients [1–8]. In addition, an estimated 10% –32% of patients with COPD included in PR programmes (PRPs) do not properly adhere to them or do not experience clinical improvement [9–11]. A number of studies have reported that the quality of life, degree of dyspnoea and lung function affect short-term adherence to PRPs [11–14]. Furthermore, the reduced physical activity observed in COPD patients may impact on their behavior leading to less motivation, fear to injury and the onset of symptomatology compatible with depression or anxiety; all of them can also impact on the adherence to PRP [15, 16].
However, these studies are heterogeneous and often fail to provide a clear and concise definition of “adherence” and of the characteristics that affect it [11–14]. Moreover, other studies have shown that the absence of clinical improvement and the difficulty in attending training sessions are important aspects to consider when discussing PRP non-adherence [12–14]. Regarding to that, it has been recommended some alternatives like technology support, such as commercial activity monitor or motion capture devices, because they could improve the patients’ adherence to the PRPs [17, 18].
Likewise, it is important to consider that most previous studies have focused on the analysis of the short-term adherence to PRPs and not on the long-term monitoring of the recommendations provided by these programmes [13, 19]; there have been mixed results regarding the repercussion of COPD exacerbations on PRP adherence [14, 19]. Hence, long-term non-adherence to PRP in COPD would counter the beneficial health effects provided by this intervention.
There is therefore conflicting evidence regarding the conditions that lead to the long-term abandonment of PRPs. The aim of our study was therefore to analyse the features of patients with COPD that contribute to long-term non-adherence to PRPs after adequately completing the programmes.
Materials and methods
Study design
We conducted a retrospective, observational study in the multidisciplinary pulmonary rehabilitation unit of a tertiary referral university hospital in the Community of Madrid, Spain, from January 2015 to December 2016.
Patients
The study included patients diagnosed with COPD, according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria [20], who were indicated for inclusion in a PRP according to the guidelines of the American Thoracic Society/European Respiratory Society and the Spanish Pneumology and Thoracic Surgery Society [1, 2]. The criteria were a dyspnoea score ≥2 on the modified Medical Research Council (mMRC) scale, accompanied by functional impairment, impaired quality of life or the presence of 1 or more COPD exacerbations [1, 2]. We just included only those patients who underwent at least 17 training sessions of a hospital PRP for 8 weeks (70% of the total training sessions programmed), which included aerobic training, skeletal muscle endurance, respiratory physiotherapy and education. We excluded patients with incomplete clinical data in their medical history, those included in a PRP in the last 2 years and those who participated in home-based programmes. Regarding to this, we created 2 groups: (1) long-term adherence to the PRP and (2) long-term non-adherence to the PRP.
Outcome
The primary outcome of the study was the factors associated with long-term non-adherence to a pulmonary rehabilitation programme for patients with COPD disease.
Variables
Long-term non-adherence to the pulmonary rehabilitation programme
The definition of PRP abandonment differs among studies [14, 19] but is typically considered when a patient attends less than 60% –70% of the stipulated sessions [14, 19]. To assess long-term drop-out, however, the definition is less clear. For this purpose, in this study, non-adherence were defined as the absence to the 32 weeks follow up visit.
Chronic obstructive pulmonary disease exacerbation
Exacerbation has been defined as acute and sustained worsening of a stable patient’s clinical condition (degree of dyspnoea, cough, purulent sputum), which exceeds the daily variability and requires a change in their usual treatment [21]. Severe exacerbations were those in which the patient presented the above conditions and required hospital admission [21].
Daily physical activity
The LCADL questionnaire is composed of 15 items that measure the degree of perceived dyspnoea during activities of daily life and consists of 4 subdimensions or scales (self-care and physical, leisure and domestic activities). The sum of the scores (in the theoretical range from 0 to 75) determines the degree of impairment. A higher score indicates an increased sense of dyspnoea while performing daily life activities [22].
Health-related quality of life
The CAT questionnaire is a standardised and specific questionnaire that evaluates the quality of life of patients with COPD [23] and consists of 8 questions, each of which can be weighed on a score ranging from 0 (best) to 5 (poorest). The overall score is therefore 0–40 points. Higher scores indicate a greater deterioration in health status or poorer COPD control [23].
The EuroQoL questionnaire is a generic instrument for measuring the health-related quality of life of relatively healthy individuals and patient groups with different diseases [24]. The individual assesses their health status by severity level and dimension and using a more general visual analogue scale (VAS) assessment. A third element of this questionnaire is the index of social values for each health state generated by the instrument (VAS and time-trade-off [TTO] scores). The descriptive system contains 5 dimensions of health (mobility, personal care, daily activities, pain/discomfort and anxiety/depression), and each has 3 levels of severity (no problems, moderate problems and serious problems) [24].
Emotional state
To evaluate anxiety and depression, we employed the HADS questionnaire [25], a screening instrument for patients in nonpsychiatric hospital departments, which contains 14 questions divided into 2 subscales: anxiety (7 items) and depression (7 items), with scores ranging from 0 to 21. The total score (anxiety and depression) ranges from 0 to 42 on a 4-point Likert scale, with an interval from 0 to 3, in which 0 is “never” and 3 “virtually all day” [25]. The results make it possible to classify patients as having anxiety and depression if their score is ≥11 [25].
Spirometry
Spirometry were performed within the previous seven days before 0 weeks visit and at the 8 weeks visit according to standardized ATS/ERS criteria [26]. To perform this, an integrated module has been used in the MasterLab-body 6.0 version equipment (Viasys, Wuerzburg, Germany). Patients were previously instructed about the manoeuvre to be performed and placed with a nasal clamp [26]. Forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1) were automatically selected as the best values from three acceptable, reproducible maneuvers [26].
6-minute walking test and lung function tests
The study followed the recommendations of the American Thoracic Society/European Respiratory Society [27]. The 6MWT was performed in a 30-m-long hospital corridor with air conditioning. There were avaible oxygen, sublingual nitroglycerine and salbutamol. In addition, it was located where a rapid and an appropriate response to an emergency was possible following the recommendations in the specific guidelines [27]. We registered the distance in metres, basal and minimal oxygen saturation and heart rate [27].
Intervention
In our unit, patients undergo a face-to-face PRP consisting of 3 training sessions per week, which involve aerobic training and skeletal muscle endurance exercises, physiotherapy and COPD education programmes (2 disease information sessions). Thus, participants included in a PRP attend 3 medical visits: at baseline (before starting the PRP); after completing the PRP (8 weeks after the baseline assessment and after attending at least 17 training sessions); and at 32 weeks after beginning the PRP (Fig. 1).
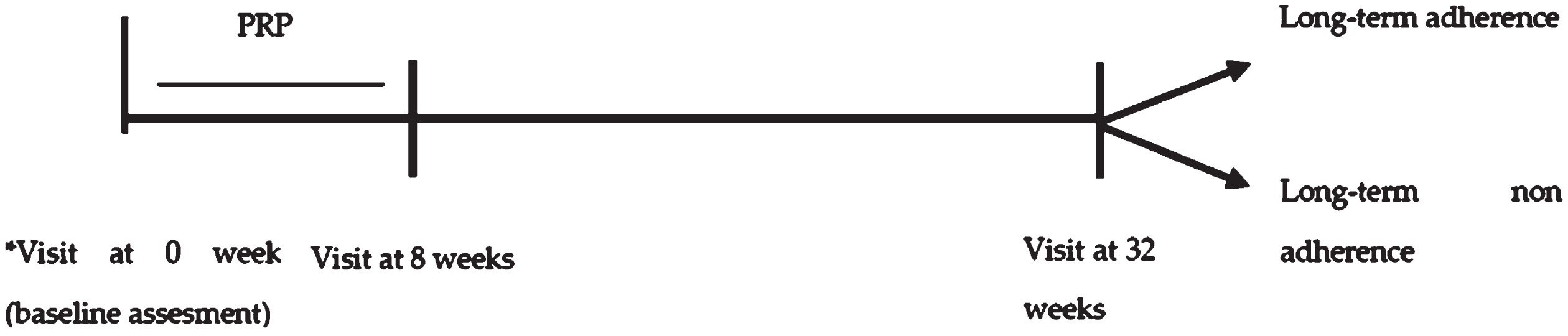
Study design. *Participants included in a PRP attend 3 medical visits: at baseline (visit at 0 week); after completing the PRP (visit at 8 weeks after the baseline assessment); and at 32 weeks after the baseline assessment. PRP: Pulmonary Rehabilitation Programme; *Patient is informed about the structure of the PRP.
In our unit, patients undergo a face-to-face PRP consisting of 3 training sessions per week, which involve aerobic training and skeletal muscle endurance exercises, physiotherapy and COPD education programmes (2 disease information sessions). Thus, participants included in a PRP attend 3 medical visits: at baseline (before starting the PRP); after completing the PRP (8 weeks after the baseline assessment and after attending at least 17 training sessions); and at 32 weeks after beginning the PRP (Fig. 1). This last clinical evaluation allows us to measure adherence to the recommendations provided during the PRP. In all of these visits, we performed a clinical evaluation of the anthropometric measures. We also tested exercise capacity (6MWT), quality of life, physical activity and emotional status, using questionnaires specifically validated for these purposes. A progressive incremental test was performed only at the baseline visit to determine the patient’s functional capacity and adjust the aerobic training during the PRP, as is recommended by the specific guidelines for PR [1, 2]. We sent a cell-phone text message to all patients to make sure they remember the appointment. On the other hand, patients with mobility limitations were provided with an ambulance to lead them to the hospital.
Ethics
The study was conducted according to the guidelines of the Declaration of Helsinki, and was approved by the Institutional Review Board (or ethics committee) of La Paz University Hospital (protocol code PI-4570; approval date January 12, 2021).
Statistical analysis
The quantitative variables were expressed as medians with interquartile range [IQR]. For the categorical variables, we employed frequencies and proportions. To compare variables between baseline and 8 weeks visit, we used paired samples Student’s t-test for quantitative variables and chi-squared test for qualitative variables. To compare quantitative variables between the groups long-term adherence vs. long-term non-adherence, we employed a Student’s t-test for independent groups. For cases in which the normality criteria were not fulfilled, we employed Mann- Whitney U test. For the qualitative variables, we employed the chi-squared test or the Fisher’s test. To investigate the variables related to long-term non-adherence to the PRP, we first performed a univariate regression to test each variable separately, in order to select those to be integrated into the multivariate model, selecting those variables with a p < 0.20. Statistical significance was set at a p-value ≤0.05. We analysed the data using SPSS (IBM SPSS Statistic version 19.0).
Results
General characteristics
The study included 70 patients (71.4% men; median age, 69.6 [63.8–75] years). The median degree of dyspnoea on the mMRC scale was 2 [2-2], and the median Charlson comorbidity index was 2 [1–3]. According to the GOLD classification, most patients were class B and D (55.7% and 37.1%, respectively). With respect to airflow limitation, 70% of the patients had a forced expiratory volume in the first second (FEV1) of 50% –79% predicted. We observed COPD exacerbations in 32 (45.7%) patients, and 22 (31.4%) patients experienced severe COPD exacerbations. Table 1 lists the patients’ baseline characteristics.
Patients’ baseline characteristics
Patients’ baseline characteristics
*Values are expressed as median [IQR] or number (percentage). **Anthropometric data is expressed as a mean±variance.
6MWT, 6-min walking test; BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; IC, inhaled corticosteroids; EuroQL, European Quality of Life questionnaire; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HADS, Hospital Anxiety Depression Scale; LABA, long-acting beta-adrenergic agent; LAMA, long-acting muscarinic antagonist; LCADL, London Chest Activity of Daily Living Scale; LTOT, long-term oxygen therapy; mMRC, Modified Medical Research Council; NIV, non-invasive ventilation; SpO2, arterial oxygen saturation by pulse oximetry; TTO, time-trade-off; VAS, visual analogue scale.
After undergoing at least 17 training sessions, the patients had a significant improvement in the degree of dyspnoea (p < 0.001), LCADL-self-care score (p = 0.04), EuroQoL-VAS score (p = 0.01), EuroQoL-TTO score (p = 0.02), and in the depression subscales of the HADS questionnaire (p = 0.02). We also noted an almost significant increase in the distance walked during the 6MWT (p = 0.053) (Table 2). At the 32 weeks follow-up visit, there was significant improvement in the degree of dyspnoea (p < 0.001) and an almost significant improvement in the 6MWT distance (p = 0.082).
Short-term impact of the pulmonary rehabilitation programme
Short-term impact of the pulmonary rehabilitation programme
*Values are expressed as median [IQR] or number (percentage). **Comparisons between groups by paired samples Student’s t-test, and chi-squared test.
6MWT, 6-min walking test; CAT, COPD assessment test; EuroQoL, European Quality of Life; HADS, Hospital Anxiety Depression Scale; LCADL, London Chest Activity of Daily Living Scale; mMRC, Modified Medical Research Council; SpO2, arterial oxygen saturation by pulse oximetry; TTO, time-trade-off; VAS, visual analogue scale.
Thirty-two weeks after the end of the PRP, 32 (45.7%) patients did not attend the follow-up visit. When comparing the 2 groups (long-term adherence vs. long-term non-adherence), we observed significant differences in the degree of dyspnoea (2 [1-2] vs. 2 [2-3], respectively; p = 0.03) and in the number of severe COPD exacerbations in the past year (0 [0-0] vs. 0 [0-1], respectively; p = 0.04) (Table 3).
Comparison of baseline characteristics between patients with long-term vs. long-term non-adherence to the pulmonary rehabilitation programme
Comparison of baseline characteristics between patients with long-term vs. long-term non-adherence to the pulmonary rehabilitation programme
*Values are expressed as median [IQR] or number (percentage). **Anthropometric data is expressed as a mean±variance. ***Comparisons between groups by Student’s t-test, and chi-squared test. When non-normal distribution, comparisons by Mann- Whitney U test.
6MWT, 6-min walking test; BMI, body mass index; CAT, COPD assessment test; COPD, chronic obstructive pulmonary disease; IC, inhaled corticosteroids; EuroQL, European Quality of Life; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; HADS, Hospital Anxiety Depression Scale; mMRC, Medical Research Council; LABA, long-acting beta-adrenergic agent; LAMA, long-acting muscarinic antagonist; LCADL, London Chest Activity of Daily Living Scale; LTOT, long-term oxygen therapy; NIV, non-invasive ventilation; SpO2, arterial oxygen saturation by pulse oximetry; TTO, time-trade-off; VAS, visual analogue scale.
The logistic regression analysis showed that a higher degree of dyspnoea (p = 0.03) and severe COPD exacerbations (p = 0.04) were associated with an increased risk of long-term PRP abandonment, and the patients’ age was an almost significant factor (p = 0.06). In the multivariate analysis, only the presence of severe COPD exacerbations remained as an independent factor in the long-term non-adherence to the PRP (OR 2.7; 95% CI 1.1–8.1; p = 0.04) (Table 4) with an area under the curve of 0.613.
Multiple logistic regression of factors associated with long-term non-adherence to the pulmonary rehabilitation program
Multiple logistic regression of factors associated with long-term non-adherence to the pulmonary rehabilitation program
CI = Confidence interval; OR = Odds ratio.
For patients with COPD, PRPs have a positive impact on the treatment of the disease [12–14, 19–25]. Our results therefore confirm that PR improves dyspnoea, quality of life, daily physical activity and the emotional state of patients. Nevertheless, our findings also confirm that a high percentage of patients drop out of these programmes in the long term. In addition, severe COPD exacerbations might be associated with this higher rate of abandonment.
This study shows the effect of COPD exacerbations on PRP adherence. The number of COPD exacerbations in our patients was lower than that reported in other studies. This is probably due to the fact that we included a larger percentage of patients with greater COPD severity than other studies [12–14, 19]. In addition, we evaluated patients three times during the follow-up (baseline, eight weeks and 32 weeks) by both pneumologists and rehabilitation physicians that work jointly in our respiratory rehabilitation unit. We observed that severe COPD exacerbations that occurred one year before the onset of this treatment behaved as a risk factor for long-term PRP non-adherence. However, Almadana-Pacheco et al. [14], Braeken, et al. [28] and Steele, et al. [29] did not detect this association in their studies. This conflicting finding might be explained by the differences observed in the lung function between the compared groups (PRP drop-out vs. non-PRP drop-out). Hence, in contrast to the study by Almadana-Pacheco et al. [14], in which the participants who abandoned PRPs had poorer FEV1, our series showed no statistically significant differences in FEV1 between the two groups. Unlike Braeken, et al. [28], we observed no positive impact of PRP on the anxiety state (HADS questionnaire) or on the COPD health-related quality of life (CAT questionnaire), which could explain the tendency of not continuing the PRP in the long-term. We can therefore tentatively suggest that long-term non-adherence to PRPs associated with severe COPD exacerbations could be influenced by a poorer COPD-related quality of life and by a higher anxiety state. It has been demonstrated that COPD exacerbations result in a worsening of dyspnoea in the moderate-long term. Almadana-Pacheco, et al. [14] found that dyspnoea was associated with a higher rate of PRP abandonment, and we observed a higher degree of dyspnoea in the group that dropped out of the PRP. New hypotheses, are therefore needed to investigate why severe COPD exacerbations affect the long-term adherence of PRP and thereby reduce PRP abandonment.
As noted above, we detected a higher degree of dyspnoea in the group with long-term PRP non-adherence, which is probably related to the occurrence of COPD exacerbations, whose negative impact on quality of life, lung function and degree of dyspnoea has been shown in various studies [5,20, 5,20]. Nevertheless, we observed no significant differences between the patients who dropped out and those who did not in terms of quality of life and lung function, which is consistent with the results of previous studies [13–19, 29]. Future studies with larger numbers of participants would therefore be required to clarify the role of quality of life and lung function in the long-term abandonment of PRP.
The drop-out rate reported in this article is 45%, which is somewhat higher than the 9% –32% rate reported in other published studies [30,31, 30,31], a difference that might be due to the fact that 31% of our patients experienced at least one severe COPD exacerbation in the past year, a higher rate than in other reports [27–34]. Nevertheless, our study focused on the long-term abandonment of PRP in a defined patient group who did not drop out of PRP in the short-term (attended more than 70% of the PRP sessions). The study therefore assessed the long-term abandonment of patients, defined in other studies as “fulfillers”, which might explain this higher drop-out rate when comparing our results with those of other studies [10].
We employed endpoints that have been accepted in other studies to assess the positive effects of PR. We therefore evaluated the degree of dyspnoea, quality of life, physical activity and 6MWT. Nonetheless, we did not consider the patient activation measure, which could have been useful in our study. Our observations showed that, after an 8-week PRP, the positive effects of PR were consistent with the results reported in other articles [1–3, 29]. We also observed a positive impact on the degree of dyspnoea, in contrast to other studies that detected no such effect on this major symptom, which is a frequent complaint in subjects with COPD [23]. There was also a notable improvement in the quality of life, the level of anxiety and in the distance walked in the 6MWT; however, the improvement did not reach statistical significance (Table 2).
This study has a number of limitations. First, the sample size was relatively small, which could have affected the discovery of more factors associated with the abandonment of long-term PR. Nonetheless, other studies used similar or even smaller sample sizes [12,14, 12,14]. Second, there were problems resulting from the retrospective analysis in terms of patient selection. Another issue were the data obtained in relation to exposure, given that the exposure to the PRP and its effects had already occurred when the protocol began. Nevertheless, we were careful in selecting the included population, unlike other studies that also included patients who attended less than half of the scheduled PRP sessions, with the potential selection bias this might induce [12–14, 19]. Our population was younger, had more comorbidities and a greater COPD severity than those of other studies [13–15, 23]. Last, with respect to the recorded data, we did not analyse the detailed patient activity, lifestyle habits and socioeconomic variables. However, we attempted to include most of the factors already analysed in other studies and even characteristics that had not been previously evaluated, such as each of the comorbidities that constitute the Charlson index, specific therapies for treating COPD and the GOLD classification according to the latest guidelines [12–14, 20]. Furthermore, we did not measure the smoking history at 32 weeks after the onset of PRP, which might be an interesting aspect to evaluate in both groups after completing the PRP.
Conclusion
This study suggests that severe COPD exacerbations affect the long-term abandonment of PRP. These results require more research, with larger sample sizes and more than 1 medical centre, with the aim of standardising the programmes and the criteria for patient inclusion. We therefore need to continue this line of research with future protocols that help to determine more precisely the factors involved in PRP abandonment, thereby modifying programmes to ensure a greater impact for a larger number of patients with COPD.
Footnotes
Acknowledgments
The authors would like to thank the IdiPaz Institute for their excellent technical assistance.
Funding
This research received no external funding.
Author contributions
Conceptualisation, C.C. M.M. and R.A.S.; Methodology, C.C. M.M. and R.A.S.; Software, P.M. A.T. E.Z. and E.V.; Validation, C.C. P.M. A.T. E.Z. E.V. M.M. and R.A.S.; Formal Analysis, P.M. A.T. and E.Z.; Investigation, P.M. C.C. M.M. and R.A.S.; Resources, P.M. C.C. A.T. E.V. M.M. and R.A.S.; Data Curation, P.M. A.T. and E.Z.; Writing –Original Draft Preparation, P.M. C.C. and R.A.S; Writing –Review and Editing, P.M. C.C. A.T. E.Z. E.V. M.M. and R.A.S.; Visualisation, P.M. C.C. A.T. E.Z. E.V. M.M. and R.A.S.; Supervision, C.C. E.V. M.M. and R.A.S.
Conflict of interest
The authors declare no conflicts of interest.