
Abstract
BACKGROUND:
Facilitating return-to-work (RTW) for working-age stroke survivors is a key component of stroke rehabilitation, however, research investigating the long-term outcomes of working-age stroke survivors is lacking.
OBJECTIVE:
To investigate the factors that influence long-term RTW for patients enrolled on a community-based early supported discharge (ESD) rehabilitation program in Singapore about five years post stroke.
METHODS:
Sixty-nine patients, aged between 18 and 60 years and were employed at the time of their hospitalization, were enrolled into the ESD program between 2012 and 2014. A prospective cohort design was adopted to examine the relationships between the factors— demographic, functional, personal, psychosocial factors and work related— and RTW at five-year follow-up. Details of RTW were collected through questionnaires via telephone follow-up.
RESULTS:
Sixty percent of the participants (n = 49) were selected for Cox and logistic regression analyses of RTW at five-year follow-up. The results indicated that having social problems is a negative predictor of RTW (OR 0.02; 95% CI 0.00–0.22) while being the breadwinner is a positive predictor of RTW (OR 13.79; 95% CI 2.46–77.52). The same factors were also significant in the time to RTW event at five-year follow-up, with a hazard ratio of 0.09 and 4.07, respectively.
CONCLUSIONS:
Early identification of the characteristics of stroke patients enrolled into an ESD program who have the potential to RTW would make interventions more targeted, increasing the likelihood of RTW.
Introduction
Stroke is a major cause of disability affecting 15 million people worldwide [1]. Globally, there is a rising trend of younger age stroke patients, with an estimated 20% of stroke survivors in the United States being of working age [2] and with one in 10 stroke patients in Singapore being aged under 50 [3]. Facilitating return-to-work (RTW) for working-age stroke survivors is a key component of stroke rehabilitation as it associates with the degree of functional capacity, presence of residual neurological impairments and depression, occupational history, and the formation of realistic vocational goal in a person’s recovery from a major disabling illness such as stroke [4].
However, research investigating the long-term outcomes of working-age stroke survivors is generally lacking, with the majority of the studies having only short-term follow-up (usually up to one year) or outcome measures that are largely impairment focused, often overlooking the psychosocial aspects of stroke recovery, such as facilitating RTW [5]. RTW is a complex and time-consuming process, with extensive literature reporting on the barriers and facilitators associated with RTW. These factors can range from personal factors to the broader social and legal context relating to employment [6, 7]. Most stroke patients were reported to have returned to work on two different time occasions: 3 to 6 months and 12 to 18 months post stroke, respectively [2]. RTW is only the first step to re-employment; stroke patients continue to face other challenges, such as job retention and maintaining work performance [8]. A recent review found that length of time post-stroke to RTW, health conditions, personal and environmental factors are associated with RTW after stroke [9].
Aim of the study
The objectives of this study were: (1) to investigate the factors which are predictive of the outcome of long-term RTW for patients enrolled in a community-based early supported discharge (ESD) program in Singapore about five years post stroke using a prospective cohort design, and (2) to examine the barriers to and facilitators of RTW for ESD patients so that interventions can be designed to optimize long-term RTW and improve work stability after stroke.
Methods
Study design
The ESD program was set up in 2007 by the National University Hospital (NUH) in Singapore. It is a community-based rehabilitation program which provides home therapy to help stroke patients maximize their functional outcomes and live as independently as possible in the community. The ESD program at NUH is led by a multidisciplinary team comprising a neurologist, an occupational therapist, and a physiotherapist. Interventions are mainly targeted at helping stroke patients to optimize their functional status and reintegrate into the community. All patients receive home-based treatment within 3 days of discharge that lasts from 2 to 6 weeks. Depending on their needs, patients usually receive home-based treatment by the occupational therapist and the physiotherapist for a total of 5 (minimum) to 20 (maximum) one-hour sessions. The occupational therapy interventions include ADL/IADL retraining, upper limb retraining, cognitive and perceptual retraining, and home modification advice. The physiotherapy interventions include strengthening exercises, indoor and outdoor ambulation, and stairs practice. There are weekly discussions on patients’ progress among the team, including the neurologist. It is not a specialized vocational rehabilitation program designed to target RTW specifically, but it addresses RTW goals depending on the needs of the ESD patients. Patients suffering from acute stroke with residual mild-to-moderate disability (≤3 months of stroke onset) and who have available caregivers are eligible for the program. All records of ESD patients, including demographics details, pre- and post-ESD outcomes, and one-year follow-up data, are recorded in an existing ESD standing database (registration number: NUH/2016-00027).
The present study on RTW utilized a prospective cohort design to examine the relationships between various factors, such as demographic, functional, personal, psychosocial, and work-related factors, and RTW at five-year follow-up for ESD patients. RTW was defined as return to paid employment on a full-time or part-time basis. Details of RTW were collected through questionnaires administered by the Principal Investigator (PI) via phone follow-up. Additional medical records were extracted from the ESD standing database.
Participants
Consecutive stroke patients enrolled into the ESD program between 1st January 2012 and 31st December 2014 (i.e. 4–6 years, with an average of 5 years post stroke) were identified from the ESD standing database. Patients were included in the study if they were of working age (18–60 years old) and were gainfully employed at the time of their hospitalization.
Patients who met the inclusion criteria received an invitation letter by post (in both English and Chinese) providing details of the nature and content of the research study. Using a prescribed script, the PI contacted the potential participants two weeks after the letter was posted to obtain verbal consent for their participation in the research study. Verbal consent was documented on a data collection form, and if consent was given, the PI administered the questionnaire over the phone, which took around 10 to 15 minutes. The study was approved by the Human Ethics Committee of the Hong Kong Polytechnic University (reference number: HSEARS20180118001) and the NHG Domain Specific Review Board (reference number: 2018/00037) in Singapore for research involving human subjects.
Data collection
The following data were extracted from the ESD standing database: age, race, gender, type of stroke, medical history, length of hospital stay, inpatient functional independence measure (FIM) score, and pre- and post-ESD outcome measure scores, including FIM, to evaluate functional status [10]; the Frenchay Activities Index (FAI) to measure participation in instrumental activities of daily living [11]; Motricity Index (MI) to evaluate motor impairment [12]; Modified Rankin Scale (mRS) to measure the extent of disability after stroke [13]; level of assistance and aids required for ambulation; and FAI scores at one-year follow-up. Sociodemographic details, such as age, gender, race, and number of people working in full-time paid employment before stroke onset, were recorded at time of discharge from NUH. Comorbidities, including diabetes mellitus (DM), hypertension (HTN), hyperlipidemia (HL), atrial fibrillation (AF), ischemic heart disease (IHD), and the presence of repeated stroke; type of stroke, and length of stay in hospital (in days) were also recorded (Table 1).
Characteristics of ESD patients contacted at five-year follow-up (n = 49)
Characteristics of ESD patients contacted at five-year follow-up (n = 49)
Note: †Independent samples T-test to compare the differences between those working and those not working. ¥Fisher’s exact test to compare the differences between those working and those not working. *Total number of patients equal to 30 due to missing data. £ mRS score. mRS = 0: No symptoms at all. mRS = 1: No significant disability despite symptoms. mRS = 2: Slight disability. mRS = 3: Moderate disability. mRS = 4: Moderately severe disability. mRS = 5: Severe disability. DM: Diabetes Mellitus, HTN: Hypertension, HL: Hyperlipidemia, IHD: Ischemic Heart Disease, CVA: Cerebrovascular Accident, FIM: Functional Independence Measure, FAI: Frenchay Activity Index, mRS: Modified Rankin Scale, MI: Motricity Index.
An RTW questionnaire was designed and the content of the questionnaire was established after a comprehensive literature search on issues relating to RTW. The content was further refined and simplified after seeking the opinions of three experts in occupational therapy with a minimum of two years of working experience in stroke rehabilitation. The format of the questionnaire was mainly closed-ended multiple choice questions or one-word answers, except for one question which involved getting the participants to rate, on a scale of 0 to 100, their ability to perform at work. The questionnaire contained a total of 21 questions that included years of education, whether they had returned to work, duration to RTW, time sustained in current job, intention to resign, number of job changes within the last five years, type of services received to RTW, barriers to and facilitators of RTW, and self-perceived capacity to RTW. In addition, we also asked participants about their previous and current types of jobs, with “white collar” work defined as spending a large proportion of time engaged in performing administrative duties or holding office jobs and “blue collar” work as jobs that involve mainly manual labor [14]. The number of questions answered by patients who had returned to work differed from the number answered by those who had not. To achieve as many responses as possible, the PI called the patients at different times of the day (e.g. during lunch hours or after work hours) and at weekends over a period of 3 to 4 weeks.
The data were analyzed using IBM SPSS Statistics 24. The baselines of the demographics between patients who had and had not returned to work at five-year follow-up were compared using Fisher’s exact test and independent samples T-test for the categorical and continuous variables respectively. Logistic regression (stepwise forward) was used to identify the predictors of RTW at five-year follow-up for all patients. Odd ratios (ORs) with a 95% confidence interval (CI) were calculated to estimate the association between the predictors and RTW. Linear regression (forward selection) was used to identify the predictors of perceived ability to RTW at five-year follow-up for those who had returned to work successfully. Statistical significance was set at p≤0.05.
Survival analysis was conducted on the basis of the censored data of time until first job upon RTW, for which the Kaplan-Meier method was used. Then, the survival analysis was stratified further by age (young-young <50 and old-young ≥50) and disability (without disability (FIM score >100) and mild-to-moderate disability (FIM score 54–100)) [10]. Comparison of the survival curves of the two groups within each stratification was conducted using the log-rank test. Cox regression was used to identify predictors of RTW at five-year follow-up. Hazard ratios (HRs) with a 95% CI were computed to estimate the relative risk between the predictors and RTW. To maximize adequate data for analysis, the ‘last observation carried forward’ (LOCF) and the mean substitution (MS) methods were adopted for missing data less than 10 to 15 percent [15].
Results
Participants
Of the 69 patients who were initially identified from the database and recruited, six (8.7%) had passed away by the time of study, 11 (15.9%) remained uncontactable, and two (2.9%) declined to participate in the study (refer to Fig. 1). Fifty patients (72.5%) who completed the questionnaires were included in the analysis. However, one patient had missing pre- and post-ESD outcome measures and hence was excluded from the final analysis (n = 49). The proportion of missing data for the post-ESD outcome measures and the questionnaires was 4% and 8.2%, respectively; they were treated using LOCF and MS, respectively. There were only 30 patients who had completed the FAI scores at one-year follow-up.

Flowchart of participants through the study.
The characteristics of all the patients (n = 49), including those who did and did not RTW, are presented in Table 1. The majority of the patients were male (75.5%) and Chinese (63.3%). The mean age of the participants was 50 (±7.4), the mean years of education was 10.1 (±3.2), and the average length of stay in hospital was 13.8 days (±11.9). Ischemic stroke was observed in 77.6% of the study population, hypertension in 44.9%, diabetes mellitus in 30.6%, and hyperlipidemia in 26.5%. There were no significant differences in demographics, pre- and post-ESD outcome measures, and FAI one-year follow-up between the RTW group and the non-RTW group.
Details on the patients who had returned to work (n = 33) are reported in Table 2. In the RTW group, 90.9% of the participants were the breadwinner of their family, with the majority earning an average income of between SGD $1 to $1999 (42.3%) and taking an average mean time of 5.7 (±4.6) months to RTW; 78.7% of them had returned to their “premorbid job”, with more patients having blue collar jobs (63.6%). Mean time in current job and the mean average of job changes in last five years were 46 (±20) months and 0.2 (±0.6), respectively, with only 6.1% expressing an intention to resign from their jobs in the next three months; 78.8% had received services to return to their current job, with hospital-provided services (96%) and alternative medicine (e.g. traditional chinese medicine or malay massage) (30.8%) being the two most common services received. Only 12.1% received assistance to help them sustain their current job, with adjustment to workload being the most common intervention (75%) given when they initially returned to work after stroke. At five-year follow-up, the patients gave a rating of 84.1 (±14.5) out of 100 for their perceived capacity to perform at work. The most common reason for returning to work was having support from family and friends (75.8%) (Table 3a), while the most common reason for not returning to work was physical impairments (40.8%) (Table 3b). The three factors ranked highest for a successful RTW were, in order of priority, 1) having support from family and friends; 2) financial factors, such as having to support family; and 3) having support from employers and coworkers (Fig. 2a). On the other hand, the three factors ranked highest as barriers to RTW were, in order of priority, 1) physical impairment, 2) cognitive impairment, and 3) social problems (Fig. 2b).
RTW details for those participants who managed to RTW successfully (n = 33)
RTW details for those participants who managed to RTW successfully (n = 33)
Factors for RTW or not RTW after stroke
Note: RTW: return-to-work.

Factors for RTW or not RTW after stroke. Note: RTW: return-to-work.
The median time from survival to RTW was 7 months, as shown by the Kaplan-Meier survival curve (Fig. 3a). The time to RTW was further divided into age group (Fig. 3b) and disability group (Fig. 3c). A statistically significance difference was found between the young-young group (median time to RTW = 6 months) and the old-young group (median time to RTW = 18 months), with p = 0.044, while only a marginally difference was found between the no disability group (median time to RTW = 5.7 months) and the mild-to-moderate disability group (median time to RTW = 12 months) at admission to hospital, with p = 0.074.
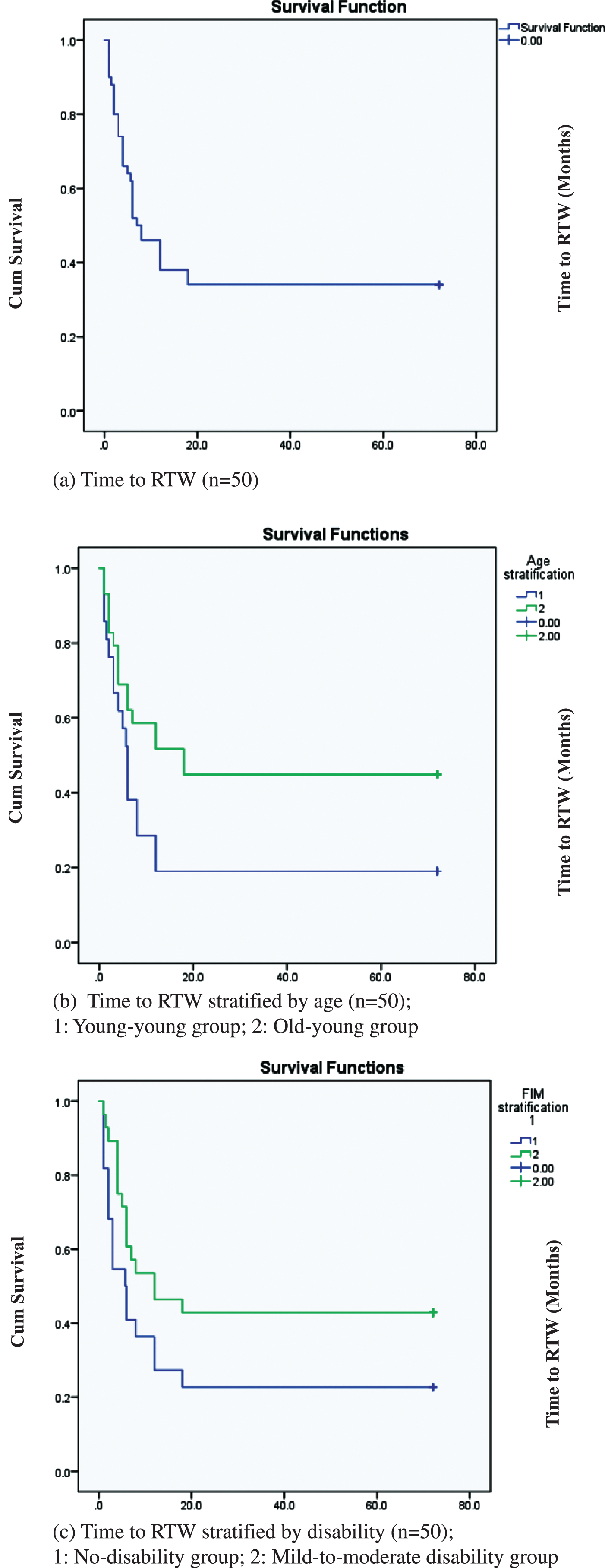
Time to RTW using survival analysis. Note: RTW: return-to-work.
Using a logistic regression for RTW at five years post stroke (Table 4), social problems, such as stigmatization, lack of support from employers, family and coworkers, etc., was found to be a negative predictor of RTW (OR 0.02; 95% CI 0.002–0.22), while being the breadwinner was a positive predictor of RTW (OR 13.79; 95% CI 2.46–77.52). Similarly, with regards to the Cox regression for RTW at five years post stroke (Table 4), having social problems was negatively associated with RTW (HR 0.09; 95% CI 0.02–0.34), while being the breadwinner was positively associated with RTW (HR 4.07; 95% CI 1.74–9.51). Regarding the linear regression for perceived capability to perform at work (Table 4), the presence of cognitive impairment emerged as a significant predictor, with p = 0.001.
Factors for predicting return to paid work five years post stroke (n = 49)
Factors for predicting return to paid work five years post stroke (n = 49)
To the best of our knowledge, this study is one of the very few studies to examine long-term RTW in working-age stroke patients and to use survival analysis to identify the predictors of RTW at five-year follow-up. We found that having social problems is a negative predictor of RTW, while being the breadwinner is a positive predictor of RTW at five-year follow-up. The facilitators of a successful RTW at five-year follow-up for stroke patients of working age are support from family and friends; financial factors, such as having to support the family; and support from employers and coworkers. The barriers to RTW at five-year follow-up for stroke patients of working age are physical impairment, cognitive impairment, and social issues.
In the present study, 60% of the study population had returned to work by five-year follow-up. Previous studies where RTW was followed up between 2 to 4 years found an RTW rate of 39% [16], and another study found an RTW rate of 74.7% at six-year follow-up [17]. Comparing the RTW rates in different studies is difficult due to differences in methodology, patient recruitment procedures, sample size, length of follow-up, and definitions of work outcomes [18].
The median RTW time is 7 months. In our study, it was found that there were significant and marginal differences between the times to RTW when the study population was divided by age group (6 months for the young-young group and 18 months for the old-young group) and disability type (5.7 months for the no disability group and 12 months for the mild-to-moderate disability group), respectively. The results of our study coincided with the two peak periods for RTW [2], suggesting that patients who are aged <50 years or have no disability in ADLs at admission tend to RTW within the first peak period of 3 to 6 months, while patients who are older (≥50 years old) or have a mild-to-moderate disability in ADLs at admission take a longer time to RTW (within 12 to 18 months). This provides insight into the duration for which patients should be followed up and rendered the appropriate assistance for RTW depending on their age and level of disability upon admission to hospital. In this study, 78.7% of the patients managed to return to their previous/premorbid job and sustained their job for an average of 46 (±20) months; this contrasts with reports in the prior literature that stroke patients experience difficulties in keeping their jobs. This difference might be because the study population in the current study only suffered from mild disability and therefore could regain their ability to be gainfully employed. Previously, there have been some studies suggesting that stroke patients with mild disability have good rehabilitation potential and are expected to achieve almost full recovery with minimal or no intervention [19]. However, this paper argues that patients with mild disability and with the potential to RTW should receive post-acute rehabilitation services to help them RTW, given that 99.8% of the participants who returned to work received post-acute rehabilitation services, suggesting that they may still face residual impairments which make returning to work difficult.
Understanding the factors which predict RTW at five-year follow-up are crucial for therapists to provide tailor-made interventions in order to improve the long-term outcome for patients of working age. In our study, we found that experiencing social problems was negatively associated with RTW and that patients with such issues are less likely to RTW (HR 0.09; 95% CI 0.02–0.34). The social problems commonly reported by participants in this study included the negative perceptions of employers and employees and the lack of support from family and friends for RTW. Other social problems, such as marital and child-related issues, are also common in working-age stroke survivors, as reported in other studies [20]. Therefore, addressing the social problems that may occur during or upon completion of the ESD program is crucial. During the ESD program, ESD therapists may have to focus their interventions in the socioeconomic environments of the stroke patients, involving immediate family members, educating employers and colleagues about the nature of the condition, and advocating for the rights of their patients [7]. The social problems that arise during the course of ESD therapy should be flagged early to other professionals, such as medical social services, so that appropriate support from different resources can be offered to patients.
It is also recommended that patients discharged from the ESD program be provided with support service contacts so that they can seek help from the relevant professional bodies if necessary [7]. On the other hand, in this study, participants who were the breadwinner of the family were found to be four times more likely to RTW than those who were not (HR 4.07; 95% CI 1.74–9.51). This finding concurs with other studies that found that there is a value to returning to work as it provides monetary benefits and social status [21]. Lastly, the results of the linear regression found that cognitive impairment was a significant factor influencing the capacity of stroke patients to perform at work (p = 0.001). Some studies have found that improving the cognitive ability of stroke patients increases the likelihood of returning to work [22]. It is therefore important to screen for cognitive impairments in all working-age stroke patients so that they can be identified earlier and receive cognitive rehabilitation to increase their chances of returning to work.
In this study, many stroke patients (33%) had still not returned to work at five-year follow-up despite their good functional recovery. The main barriers to RTW were the visible and invisible symptoms of stroke, which were often poorly understood by the support systems of stroke patients (such as family, friends, employers, and colleagues) and thus often led to stigmatization. However, it was also these support systems that the stroke patients found most valuable to their recovery and well-being. It has been commonly reported in the literature that strong interpersonal support could serve as an asset to RTW and reduce experiences of discrimination [23]; this highlights the need for healthcare professionals to proactively educate the support systems of stroke patients about their symptoms and the management of symptoms, effectively turning these support systems into assets to aid their recovery from stroke. A recent study found that absence of environmental restrictions is the strongest predictor for higher rates of RTW after stroke [24]. Workplace accommodations to improve RTW rates have been strongly recommended in the literature [6]; however, only 12.1% of the stroke patients in this study received such services to sustain them in their current job. It may be possible that the RTW rates could be higher if the non-RTW group was referred to specific vocational rehabilitation services upon discharge from the ESD program.
This study has several limitations, and interpretation of its results should be made with caution. First, the sample size was small and not sufficiently representative of the whole stroke population as the patients who were recruited mainly had a mild-to-moderate disability. Second, there might be recall bias as the patients were asked to retrospectively recall their employment before their stroke. Thirdly, important determinants, such as duration of sick leave and other comorbidities that emerged within the five-year period, were not available, which may have influenced the result findings.
Conclusion
In this study, we found that 67% of the patients had returned to work by the time of the five-year follow-up after stroke. Early identification of the characteristics of stroke patients enrolled into the ESD program who have the potential to RTW would make interventions more targeted, increasing the likelihood of them returning to work.
Footnotes
Acknowledgments
None to report.
Conflict of interest
All authors declare that they have no conflict of interest.
Funding
The authors report no funding source.
Ethical approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki of 1975, as revised in 2000.
Informed consent
Informed consent was obtained from all individual participants included in the study.