
Abstract
BACKGROUND:
Mental disorders are among the leading causes of disability for which family physicians are often required to complete sickness certificates. Yet, little is known about family physicians’ sick-listing practices in Quebec.
OBJECTIVE:
This study aims to describe their practices, difficulties and needs.
METHODS:
Twenty-three family physicians completed a comprehensive questionnaire on sickness certification practices. Descriptive statistics were used.
RESULTS:
Despite being completed on a weekly basis, sickness certifications were deemed problematic by all participants. While they rarely refused to sick-list a patient, 43.5% reported suggesting accommodations as an alternative to sick leave. Waiting-time to access psychotherapy and delays to set-up workplace accommodations are responsible for many unnecessary sick-leave prolongations. Lack of time, long duration absences, situations where the physician held a different opinion than the patient/healthcare provider and assessing an individual’s capacity to work are the most common reported problems. More than half of participants indicated medical schools do not greatly prepare them to carry out these tasks.
CONCLUSION:
Sickness certifications are deemed problematic, and more training might be key. Our results can be used by medical schools or bodies responsible for continuous education to improve training.
Introduction
Sickness disability represents an economic burden for both organizations and society as a whole [1–3]. According to the Organisation for Economic Co-operation and Development [4] it is estimated that its member countries are among those with the highest share of disability benefits in the world. This includes Canada. In Quebec, this is particularly true, as although this province only makes up 23% of the Canadian population, 33% of all disability claims are recorded here [5]. Mental health disorders are known to affect a greater proportion of workers in their early and prime years, which can likely result in disability benefits claims [6]. In most countries, the decision regarding the allowance of disability benefits does not belong to the physician, but to the insurance system [7–9]. Nevertheless, when a family physician is of the opinion that a worker’s medical condition results in a reduction in his or her ability to work, the family physician will likely recommend a medical leave of absence. For the purposes of this study, and in accordance with the terminology used in many European studies [10, 11], this task will be referred to as sick listing. When sick listing a worker, the family physician is required to provide the insurer with a medical certificate to substantiate the worker’s limitations and restrictions [12, 13]. This information allows insurers to determine a worker’s entitlement to benefits based on contractual provisions [14]. While physicians frequently carry out sickness certifications tasks, most of them perceived these as problematic [14–18]. Most studies report that family physicians admit struggling when carrying out these tasks [19, 20]. In general, lack of time, handling conflicts with patients, assessing functional limitations and working capacity and estimating the optimal length of absence are among the most common difficulties [20–22]. Sick listing a worker with a mental disorder is thought to be more complex due to the more subjective nature of their symptoms [23, 24].
To date, fewer studies have been carried out on family physicians’ sick-listing practices in the context of mental disorders [24–28]. While we have little knowledge around family physicians’ sick-listing practices specific to mental disorders, it is thought that many sickness certificates are being completed for these, as mental disorders are becoming one of the leading causes of disability in Quebec.
Objectives
Primary care is generally the gateway to the health care system. Family physicians are the first to be consulted by patients when they are sick or no longer feel capable of working. Sick listing a worker with a mental disorder is thought to be more complex due to the more subjective nature of their symptoms [22, 23]. Many studies have focused on sickness certifications in general, but very few studies have been carried out to specifically investigate family physicians’ sick-listing practices in the context of mental disorders [23–27]. This is an important topic as mental health disorders are becoming one of the leading causes of disability. This is particularly true in Quebec, where mental disorders account for 41% of disability claims compared to the rest of Canada, for which the average is around 25% [5]. Since family physicians play a key role in disability management it is important to better understand their practices. Gaining more knowledge about their practices and needs will not only help customize trainings but may also help enhance the disability management field. Therefore, this study aims to describe Quebec’s family physicians’ practices surrounding sickness certifications of mental disorders, their perceived difficulties and training needs so as to ensure high quality sickness certifications.
Method
The first author met with the Fédération des Médecins Omnipraticiens du Québec (FMOQ) to inform them of the study. They agreed to share the link to the online comprehensive questionnaire to their members in their monthly newsletter. During the fall 2019, it is estimated that close to 7530 physicians received the newsletter. Three email campaigns to encourage participation were sent by the FMOQ. Others were also made aware of the project by their Regional Association of General Practitioners, social media, clinic directors and the GMF-Universitaire Maisonneuve-Rosemont. Analyses were conducted on twenty-three participants.
Participants
Twenty-three family physicians including 18 women and 5 men, with an average of 16.8 years of practice, participated in the study. All participants worked within the Province of Quebec’s Public Health System and the vast majority worked in a family medicine group setting (FMG). Further demographic information is available in Table 1.
Sample description
Sample description
Note. N = 23. Participants had on average 16.8 years of practice (SD = 12.3); aSome participants worked in more than one clinical setting.
Selection criteria were as follows: French proficiency, having issued a minimal of one sickness certificate for mental disorder in their practice and being a member in good standing with le Collège des Médecins du Québec.
The study rolled over a period of eight months and was approved by the Research Ethics Committee from the University of Quebec in Montreal and by the Ethics Committee of the Integrated University Health and Social Services Centre of the East.
This study utilized a comprehensive questionnaire developed by Alexanderson for the Karolinska Instituet in Stockholm (2015). This questionnaire has been reviewed by clinicians, teachers, and researchers in the field of insurance medicine and has been frequently used in European studies [29–32]. For this study, an adaptation, and an in-house translation from English to French was carried out [29–31]. The preliminary version was evaluated by a psychiatrist and two psychologists, who were familiar with sickness certifications and who were not involved in the translation process. Minor adjustments were made, and the final version included a total of 142 items. For this study, 97 out of the 142 items are included for analysis. These are: frequency of different sick listing situations, the frequency and external factors leading to unnecessarily sick leave prolongations, perceived difficulties, the extent to which medical school has helped them develop proficiency in handling sickness certifications, perceived training needs and solutions to help enhance the quality of medical certificates.
Items in relation to specific sick-listing certification situations such as frequency, willingness to provide or to refuse a sick-leave, conflicts surrounding sickness certifications and alternatives to sick-listing a patient were offered a 6-points scale response (more than 10 times a week, six to ten times a week, one to five times a week, about once a month, a few times a year and never or almost never). For the analysis, more than ten times a week and six to ten times a week were combined to “more than 6 times per week” and once a month and a few times a year were combined. Difficulties encountered by family physicians’ category included items related to assessing the working ability and functioning limitations, handling sickness certification tasks and conflicts. Family physicians responded to items according to a 4-point scale ranging from very difficult to not at all. Items aiming at exploring to what extent each education level helped develop sickness certifications competency were provided a 4-point scale response ranging from very to not at all. Family physicians’ perceived needs for trainings such as conflict resolution and stakeholders’ responsibilities were answered on a 4-point scale ranging from to a large extent to not at all. Different solutions to enhance the quality of sickness certifications such as attending workshops or conferences were proposed to physicians. They were asked to rate on a 3-point scale (from very beneficial, moderately beneficial, and not beneficial) the relevance of each of element.
The questionnaire was hosted on Interceptum software (Acquiro System, 2017) as they commit to a highly secure and reliable software. To facilitate access to physicians and recruitment, the questionnaire was available online and participants were able to access it at any given time. Although they were encouraged to complete it all at once, they were also given the option to return to the questionnaire later, should they be interrupted. The consent form preceded the questionnaire and inclusion criteria were reiterated. Participants were required to confirm that these were met. Completion time ranged between 30 and 35 minutes.
Data analysis
Descriptive statistics were calculated for all variables
Results
Sickness certifications
In response to the general question “how often this type of consultation is deemed problematic”, more than three-quarters of the participants (82.6%) reported that this was problematic at least once a week (Fig. 1).
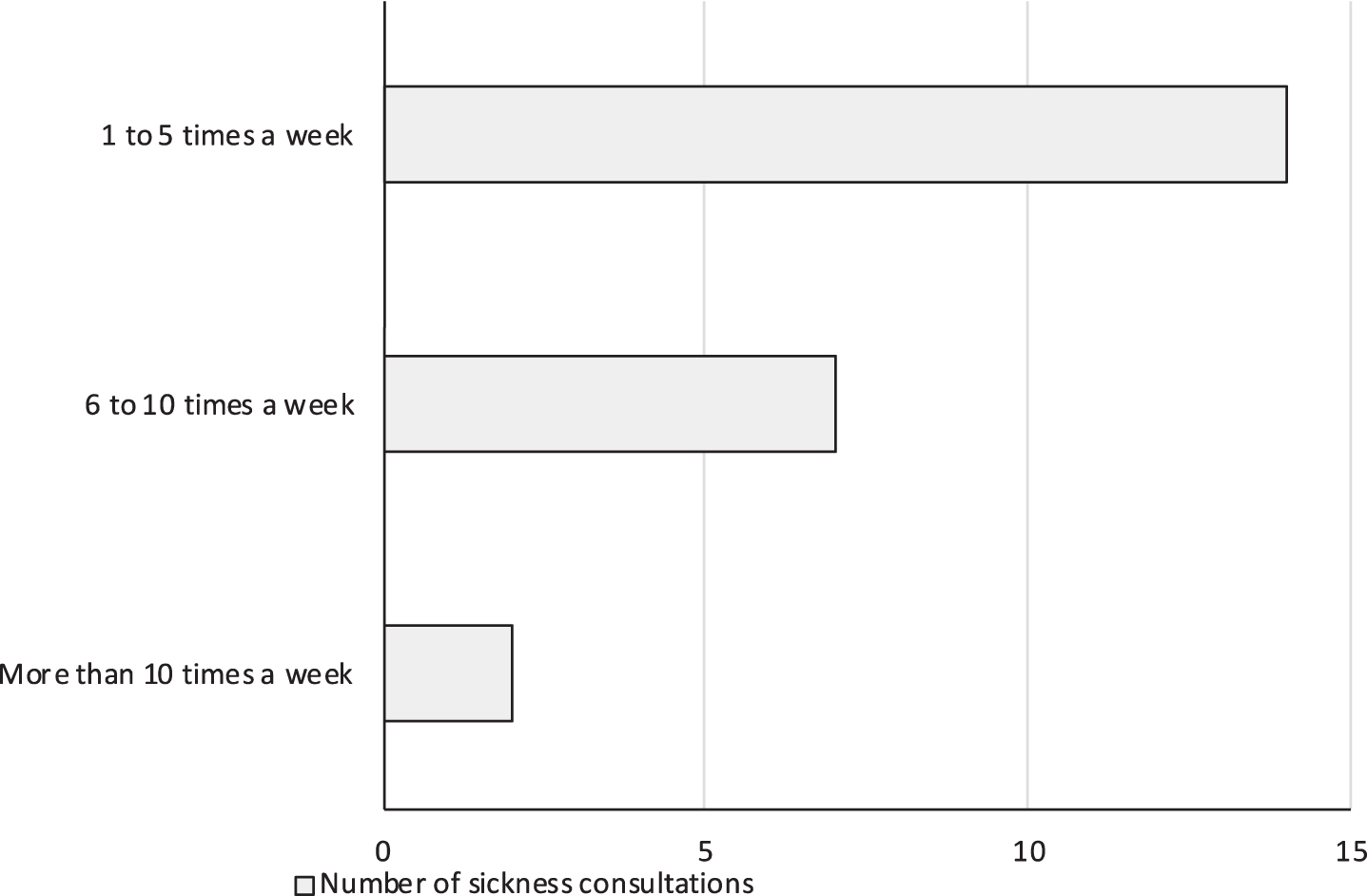
Number of sickness consultations.
For all participants, sickness certifications consultations occurred weekly. Close to 40% (39.1%) stated that these happen 6 times or more a week. As shown in table 2, most family physicians expressed lacking time at least once a week to accomplish sickness certification related tasks, with 82.6%, 78.2% and 73.9% of them reporting lacking time with patients, for administrative work including communication with stakeholders, and for education, respectively.
Frequency of FPs lacking time for different sickness related tasks (n = 23)
The frequencies of different situations related to the handling of sick-leave certifications are available in Table 3. More than a quarter (26.1%) of our participants perceived that, at least once a week, patients consulted them for a sickness certification for non-medical reasons and 52.2% believed that the reasons for these consultations were concealing a problem in the patient’s work environment. 43.5% of the participants indicated that every week they proposed accommodations as a mean to help maintain the patient at work. More than half of the participants (60.8%) never refuse or only refuse a few times a year to provide a sickness certificate. For most participants (78.2%) conflicts with patient surrounding a sick leave were deem rare.
Frequency of sick-listing situations encounter by FPs (n = 23†)
Frequency of sick-listing situations encounter by FPs (n = 23†)
Note. †=questions that were not applicable to every participant, so the total n is lower than 23.
Slightly over half of the family physicians held return to work discussions at the beginning of the sick-leave period (52.2%), while 47.8% shared having them only when the patient becomes partially functioning.
Sick leave prolongations due to external factors
While 95.7% of respondents believed that lengthy sick leave could have negative effects for a patient, most participants admitted prolonging unnecessary sick leaves, at least once a month, due to external factors such as waiting-time to access care such as cognitive-behavioral therapy (73.9%), psychotherapy (60.9%), psychiatrist’s appointment (34.8%) or next available medical appointment (39.1%). Other reasons included delays to set-up accommodations in the workplace (60.9%), patient’s poor treatment compliance (17.4%) and to avoid a conflict with a patient (17.4%).
Problems encountered by physicians when dealing with sickness certifications tasks
As seen in Table 4, of the 20 listed problems, 6 were deem very difficult for more than a third of the sample. For instance, handling sickness certifications ranging from 91 days to 180 days and over 180 days was deemed very difficult by 43.5% and 65.2% of the family physicians, respectively. These numbers are contrasting with shorter duration leave (90 days or less; and 15 days or less) for which only 8.7% and 4.3% of all family physicians perceived them to be very difficult, respectively. Handling situations in which family physician and patient or two health care professionals hold different opinions about sick listing is very difficult for 52.2% and 47.8% of all family physicians, respectively. Slightly over a third of the participants (34.8%) rated being the medical expert for the insurer while being the patient’s treating physician as being very difficult. Assessing the degree to which the reduced functioning limits a patient’s capacity to perform his/her work tasks and estimating the optimal sick leave duration were very difficult for 30.4% of the sample.
FPs perceived sickness certifications difficulties (n = 23)
FPs perceived sickness certifications difficulties (n = 23)
As shown in Table 5, a high proportion of family physicians believed that their initial training does not greatly prepare them to handle sickness certifications. For instance, only over a quarter believed that residency has “very” or “rather” helped develop these competences. Among the thirteen skills/training options that were presented to the participants, more than half of the participants opined that they largely or fairly need to develop their skills and knowledge around the rules/legal aspects of sickness insurance, stakeholders’ roles, information about other compensation systems, handling conflicts with patients around sick leave certifications, understanding the demands required in different occupations and assessing patients’ work capacity/work limitation. Table 6 provides a full summary of areas where further training may help enhance sickness certification quality.
Education and sickness certifications skills development (n = 23)
Education and sickness certifications skills development (n = 23)
FPs perceived needs for training (n = 23)
As shown in Table 7, family physicians were proposed sixteen different options that are thought to help ensure high quality medical certificates. Among those, the following six obtain the higher appreciation rate: to discuss with other healthcare professionals about a patient’s functional limitations, to have more contacts with insurance physician experts, to have a standardized instrument or protocol to assess functional limitations, to attend conferences or seminars, to have courses in insurance medicine and a better-informed general population about disability programs.
Perceived valued of solutions aiming at ensuring high quality sickness certifications (n = 23)
Perceived valued of solutions aiming at ensuring high quality sickness certifications (n = 23)
This is the first study in Quebec that uses a very extensive questionnaire to gather a more thorough understanding of sick-listing tasks, practices, difficulties and needs of family physicians when sick-listing a worker due to mental disorders. For all our participants sickness certifications consisted in a weekly task and close to 40% of the family physicians disclosed doing this more than 6 times a week. This task was qualified as problematic by most of the participants. Our results are consistent with those of qualitative and quantitative studies conducted both in Canada and internationally [19, 33]. Despite an average of 16.8 years of practice, one in five physicians felt that their insurance medicine skills were inadequate at least once a week. Few family physicians perceived that their medical training has helped them acquired these skills, which is in line with other international studies [21, 35]. Interestingly, of the two-family physicians who pursued an insurance medicine course as part of their continuous education, one of them felt that it was not helpful at all. Participants expressed the desire to obtain more training which also echoes other studies findings [36, 37]. Considering that mental disorders account for one-third of all disability claims and are reported to be more complex, it is important to develop specific trainings that meet physicians’ needs.
Performing functional assessments and determining an individual’s capacity to work, have been highlighted as areas requiring more substantial training. Family physicians could theoretically consult with occupational health physicians or occupational therapists to help assess a worker’s functional limitations. However, available resources do not currently allow for this. In Quebec, there is a shortage of occupational therapists, which results in longer delays for services [38, 39]. As such, the task of completing medical certificates often falls upon the family physician. Many studies show that these are often incomplete or ambiguous [40]. As a result, negative unintended consequences may include insurance claims being denied or delays in rendering a decision [8]. Therefore, while we believe that the gold standard could ideally include greater interdisciplinary collaboration, in the face of a glaring lack of resources it is important that initial medical training include more disability-related components.
The legal aspects of disability and the roles and responsibilities of all stakeholders involved in the disability management process are also competences that family physicians would like to develop further. Interdisciplinary conferences that could bring together several professionals such as insurers, insurance medicine experts, lawyers, human resources advisors and return-to-work coordinators can be key. For instance, most physicians indicated needing more knowledge around each stakeholder’s role and some admitted prolonging work disabilities due to delays in accessing services. However, many insurers have rehabilitation departments to help workers regain their functional abilities or to bridge the gap between residual symptoms and function. From this perspective, a better understanding of each stakeholder’s roles and responsibilities appears essential in enhancing collaboration and expediting recovery and return to work outcomes.
Conflict management also appears to be an area where more training might be needed. While our participants indicated that conflicts with patients around sickness certifications were uncommon, nearly one physician out of five admitted prolonging a sick leave at least once a month to avoid a conflict. These results are somewhat inconsistent and may attest more experienced conflicts than openly reported. From an instrumental conditioning perspective, certifying a patient to avoid a conflict is a form of negative reinforcement. Given that reinforcement increases the likelihood that a behaviour occurs again in the future, it is important to develop conflict resolution training that would allow family physicians to handle these challenging discussions differently. These results may not only raise ethical concerns but also questions pertaining to the cost and benefits of this approach. On one hand, an increase in absence duration reduces the likelihood of a worker returning to work [3]. On the other hand, lengthy absences are associated with negative outcomes for a patient. As such, developing trainings that meet physicians’ needs is important and may allow for not only greater patient-physician relationships, but also to less administrative work, more time with patients, and earlier rehabilitation interventions or return to work.
Limitations
Our results should be interpreted with caution due to the small sample size. Despite multiple recruitment campaigns, extensive solicitation efforts and the support of different medical associations and the FMOQ, few family physicians participated. While this may speak to a deeper problem, namely a lack of time which was highlighted by the participants, this could translate to a bias. For instance, there is a possibility that only family physicians who had strong interest in sickness certifications agreed to participate, or else, those who struggle the most with these tasks showed substantial interest in the study. Furthermore, it is well known that the use of questionnaires opens the door to social desirability. As such, we cannot exclude that participants may have over-reported “optimal” practices and under-reported other behaviors.
Future directions
Given that family physicians call for further education on disability, future studies should focus on training material development. So far, most of the family physicians’ knowledge around sick-listing practices is acquired by trial and error. Given this, future studies should measure social validity to ensure that training material is deem acceptable and satisfactory by the users. Additionally, given that nurse practitioner’s field of practice is expanding in Quebec, resulting in more autonomy in respects to sick listing a patient, it is recommended that future studies focus on their practices and needs.
Some studies suggested that asking physicians to complete fit forms instead of disability forms could reduce the number of workers on sick leave [41]. Completing fit forms and focusing on preserved abilities could potentially prompt physicians to recommend workplace accommodations. As such, insurers should reflect on the pertinence of requesting fit forms and perhaps collaborate with researchers in the field to determine whether this brings an added value to the process and results in better outcomes for all stakeholders.
Conclusion
In conclusion, results showed that family physicians perform sick-listing tasks weekly and most of them perceived these as problematic. Interestingly, 43.5% of the participants admitted recommending accommodations for their patient as an alternative to a sick leave. Work plays an important part in an individual’s health and wellness. It can beneficial, when appropriate, to offer workplace accommodations as an alternative to a sick leave. This would allow employees to maintain the structure and routine that a workplace provides, while seeking out or engaging in supports to address their mental health concerns. Unfortunately, family physicians stated that long waiting-times to set-up accommodations in the workplace are responsible for many unnecessary sick-leave extensions. Better collaboration and communication between all stakeholders could possibly bridge this gap.
More than half of the participants indicated that current training curriculum did not significantly prepare them to carry out sickness certification tasks. As such, training material would likely need to be revised as very few perceived that it prepares them for their clinical practice. Our findings are important and highlight main areas for training. The following represent the main areas of focus for future training opportunities: legal aspects of sickness insurance, stakeholders’ roles, other compensation systems, conflict management and assessing patients’ work capacity/work limitations. Insurers, medical schools and/or associations can develop targeted trainings to meet the needs of family physicians. Given the key role they play, improved training can help facilitate communication and coordination between all stakeholders and could ultimately improve the disability management process.
Footnotes
Acknowledgments
The authors would like to thank Vanessa Alborino for the linguistic revision and feedback.
Ethics statement
The study was approved by the UQAM/Comités d’éthique de la recherche avec des êtres humains (#2979, date: 29-05-2019).
Informed consent
Informed consent was obtained from all participants.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
Not applicable.